Artificial insemination (AI) is a low-cost, low-complexity assisted reproductive technique. Normally, it is indicated when it is difficult for the sperm to reach the uterus naturally.
However, this technique does not always make it possible to achieve pregnancy, as a number of essential requirements must be met. For this reason, you might wonder when artificial insemination should be performed.
Depending on the infertility problem and the circumstances of each patient, conjugal AI or donor AI will be indicated. In this article we are going to explain in detail the cases in which each of the types of artificial insemination is recommended.
Provided below is an index with the 8 points we are going to expand on in this article.
- 1.
- 1.1.
- 1.2.
- 1.3.
- 1.4.
- 2.
- 2.1.
- 2.2.
- 3.
- 4.
- 4.1.
- 4.2.
- 4.3.
- 4.4.
- 4.5.
- 4.6.
- 4.7.
- 4.8.
- 5.
- 6.
- 7.
- 8.
Indications of AIH
Artificial insemination with husband’s sperm (AIH) is a procedure in ART in which the spouse's own sperm is used. It is recommended when the woman is less than 35-37 years old.
The same couple may be involved in one or more of the situations discussed below. If both members of the couple are affected, this is a case of sterility of mixed origin, as the inability to achieve pregnancy is caused by both male and female problems.
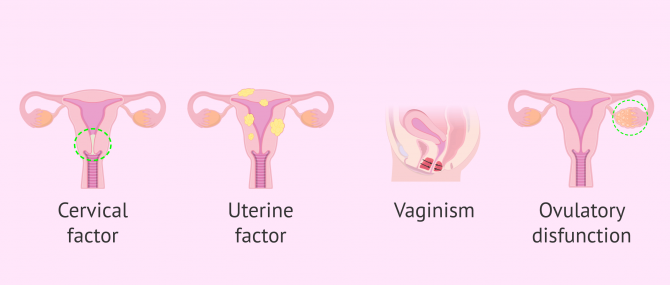
Sterility of female origin
The AIH is indicated in cases where the problem is due to sterility on the part of the woman, as long as the cause is:
- Cervical Factor
- alterations in the quality of mucus from the cervix that prevent sperm from reaching the uterus or fallopian tubes, as it acts as a barrier.
- Uterine Factor
- anomalies in the anatomy or functioning of the uterus, such as uterine malformations, uterine fibroids, endometriosis, intrauterine adhesions, etc.
- Vaginism
- involuntary contraction of the muscles of the vagina, which prevents the deposit of semen.
- Ovulatory dysfunction
- there are irregularities in ovulation such as anovulation, polycystic ovary syndrome (PCOS), etc.
If you want to read more in-depth information about this, you can visit the following link: What causes female infertility & sterility? Symptoms and treatments.
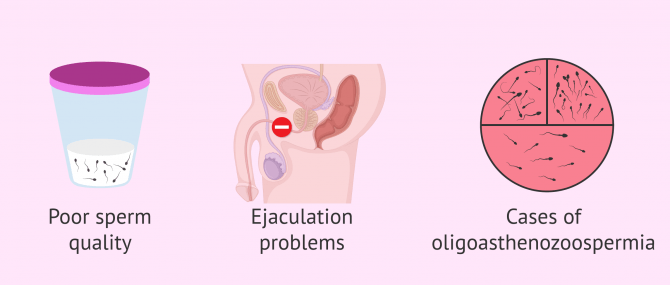
Sterility of male origin
Artificial insemination by husband is also indicated in cases where the problem is caused by the man, as in:
- Alterations in sperm quality that can be observed after a seminogram in a man. It refers to a reduction in the quality, quantity and morphology of spermatozoa.
- Inability to deposit semen in the vagina, which may be due to premature ejaculation, psychogenic impotence, hypospadias, or retrograde ejaculation.
- Cases of oligoastenoteratozoospermia: seminal samples with low quantity, problems of mobility and morphology of the spermatozoa.
For more information, we invite you to continue reading this article: What are the causes of male infertility? - Symptoms & solutions.
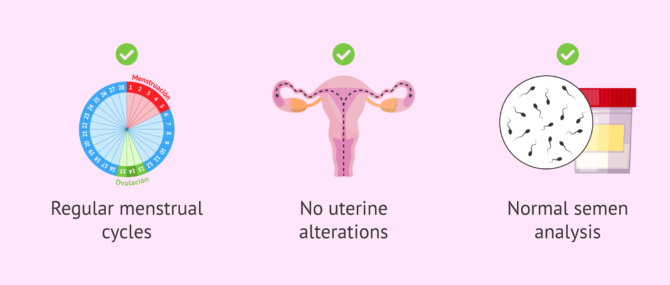
Sterility of unknown origin
Sterility of unknown origin is that form of sterility that occurs when fertility tests in the couple (both man and woman) indicate normal results, but even so, pregnancy is not achieved.
On the one hand, the woman has regular menstrual cycles and a uterus with normal morphology. In addition, it lacks polyps or fibroids, that is to say, it has no uterine alterations.
On the other hand, the male has no anomaly and his seminogram shows values within the normal range, so his sperm quality is good in relation to morphology, quantity, mobility, etc.
Si te interesa saber más acerca de la EOD, entonces visita este post: What Is Unexplained Infertility? - Causes, Diagnosis & Treatment.
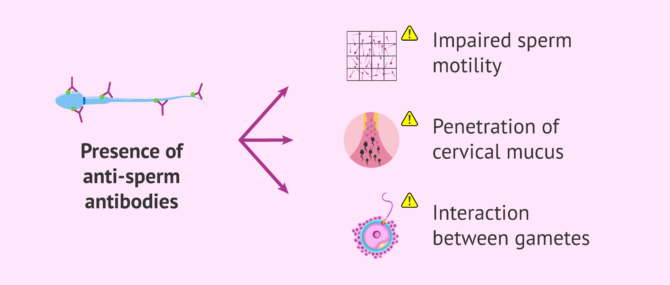
Immunological sterility
The AIH is recommended when there is some immunological alteration that can be due to the presence of antispermatozoid antibodies (ASA), which affects the motility of the spermatozoid, the penetration in the cervical mucus or even the interaction between the gametes (ovum and spermatozoid).
If these ASA antibodies are present in the cervical mucus, the solution would be to deposit the spouse's semen directly in the uterus. This prevents the defenses of the woman's vagina from attacking.
In the following link you will find in-depth information about it: Immunologic infertility: types, causes and treatments.
Indications of AID
In artificial insemination with donor (AID), as its name suggests, semen from an anonymous donor is used and is indicated in the cases discussed below.
Absence of male partner
In cases where there is no male partner and there is a desire to achieve pregnancy, an artificial insemination with donor sperm can be performed. These include single women who choose to become mothers or female couples.
To do so, they must meet the following requirements:
- For women without a male partner who do not appear to have fertility problems, the age limit is 40 years instead of less than 35-37 years as was the case in AIH.
- No history of genital infections and pelvic surgery.
- Not having endometriosis type III or type IV, that is, moderate or severe endometriosis respectively.

With male partner without the possibility of sperm contribution
In the case of couples between a man and a woman, artificial insemination with donor sperm may have to be used due to various factors. These are detailed below:
- Severe male infertility such as a secretory azoospermia. In this case, no sperm appear in the semen and fertilization cannot take place.
- History of genetic disease in the male and lack of treatment with preimplantation genetic diagnosis (PGD).
- Sexually transmitted disease in the male after several sperm washings. This means that in seropositive patients (affected by HIV, Hepatitis B...) it is necessary to perform sperm washings. This separates the sperm from the other components of the semen and reduces the risk of transmission to the mother and baby. If, after the molecular tests to check the successive washes, viral load is still identified, insemination with donor semen is used.
- Rh incompatibility of the couple. This occurs when the mother is Rh negative and the father is Rh positive. If the fetus inherits the Rh-positive from the father, maternal and fetal blood contact will produce maternal antibodies (defenses). This has negative consequences on the pregnancy, as it can lead to misscarriages. The mother is normally isoimmunized so that there is no problem, but in certain cases a solution is still not possible and AID is used.

Below, you will find a link with more detailed information: Donor intrauterine insemination: What is it and how much is it?
When not to perform artificial insemination
Artificial insemination is the assisted reproduction technique that requires less intervention by the specialist. Many people opt for it because it is more comfortable and economical. However, if the necessary requirements are not met, there may not be a chance of achieving pregnancy through this method.
In order to do artificial insemination, both by husband and donor, it is necessary for the woman to comply with the following:
- Having permeable tubes, i.e. the passage through them is not blocked. This can be checked by laparoscopy or hysterosalpingography (HSG).
- Being able to ovulate, either spontaneously or through hormonal medication.
- Age of the woman less than 35-37 years. This is because, with age, the ovarian reserve decreases, and the likelihood of pregnancy is reduced. It does not mean that it will be impossible for these women to get pregnant by this method, but the chances often are so low that it is not worth it. In these cases in vitro fertilization is recommended.

Thus, if, for example, it is a woman who has had a tubal ligation, under no circumstances may she undergo artificial insemination, either with semen from her spouse or from a donor. The reason for this is that her fallopian tubes are blocked and sperm will never be able to meet the egg to fertilize it, so she does not meet one of the basic requirements for artificial insemination. The solution, in this case, would be to carry out an in vitro fertilization treatment.
In relation to the masculine part, it is necessary that the semen has a good quality so that the spermatozoa are able to cross by themselves the whole feminine reproductive system, reach the fallopian tubes and fertilize the ovum.
If the seminal quality of the future father is not adequate, the possibilities would be to carry out in vitro fertilization (IVF), or to use donor sperm with excellent sperm quality.
FAQs from users
When is AI recommended?
Artificial insemination (AI) is a low-complexity assisted reproduction technique that consists of placing the partner's or donor's sperm into the woman's uterus. The most frequent indications are sterility without apparent cause and cases of male factor with slight alterations.
Can the same sperm donor be used for a second pregnancy?
In Spain, it is possible to use the same sperm donor for a second pregnancy, provided the requirements established by Law on Assisted Human Reproduction Techniques are met.
Spanish legislation sets a legal limit of six children born in Spain per donor. As long as this limit has not been reached and the clinic (or donor bank) still has available samples from that donor, the same donor may be used for a subsequent pregnancy.
What are the causes of failure of artificial insemination?
Artificial insemination (AI) is a low-complexity assisted reproductive technique and its pregnancy rate is around 13-25% if conjugal sperm is used and 18-29% if donor sperm is used.
There are several reasons for AI failure: age, infertility time, semen quality, ovarian response to medication, etc.
I have tubal patency in only one tube. Can I become a mother through IUI?
In the artificial insemination process, fertilization takes place in the Fallopian tubes and, therefore, it is necessary that at least one of them is permeable, that is, it allows the egg and sperm to meet.
If only one of the tubes is functional, achieving pregnancy is more complicated, but not impossible, since fertilization can take place in the other tube.
Is preparation necessary before artificial insemination?
It is necessary to stimulate your ovaries before artificial insemination. Various ultrasound controls will be carried out to determine the most appropriate moment for the insemination.
Can you undergo IUI with moderate asthenozoospermia?
Asthenozoospermia refers to motility issues in the sperm. If the percent of sperm with poor or non-existent motility is high, it is unlikely that sperm are able to swim toward the egg and fertilize it after the insemination. Thus, although it depends on the level of severity of asthenozoospermia, it is better if you go directly for IVF with ICSI.
What are the risks of artificial insemination?
Although this is not a very dangerous technique, among the most important risks are possible multiple pregnancies, ectopic pregnancies and ovarian hyperstimulation.
Get more answers to your question in this post: Risks of Artificial Insemination.
How is ovulation monitored to determine the best day for insemination?
To schedule insemination for the optimal moment, that is, for the day of ovulation the woman is prescribed low doses of hormonal medications. This treatment allows you to regulate and control your ovarian cycle. To this end, you doctor monitors the treatment with transvaginal ultrasounds and blood tests to measure estradiol levels.
Suggested for you
In this article we have referred to the two fundamental requirements that the patient must meet to guarantee a minimum of success in an artificial insemination. For other necessary conditions, click here: Basic requirements for artificial intrauterine insemination.
If you are considering artificial insemination as an assisted reproduction treatment to have a child, we recommend that you carefully read the following article to understand the process in detail: How is an artificial insemination done step by step?
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Anca Huniadi, Erika Bimbo-Szuhai, Mihai Botea, Ioana Zaha, Corina Beiusanu, Annamaria Pallag, Liana Stefan, Alin Bodog, Mircea Șandor, Carmen Grierosu. Fertility Predictors in Intrauterine Insemination (IUI). J Pers Med. 2023 Feb 23;13(3):395. doi: 10.3390/jpm13030395 (View)
Carleigh B Nesbit, Misty Blanchette-Porter, Navid Esfandiari. Ovulation induction and intrauterine insemination in women of advanced reproductive age: a systematic review of the literature. J Assist Reprod Genet. 2022 Jul;39(7):1445-1491. doi: 10.1007/s10815-022-02551-8 (View)
Corson SC, Batzer FF: Homologous artificial insemination. J Reprod Med 26:231, 1981.
Dixon RE, Buttram VC Jr, Schum CW: Artificial insemination using homologous semen: a review of 158 cases. Fertil Steril 27:647, 1976 (View)
Kim YJ, Park CW, Ku SY. Indications of intrauterine insemination for male and non-male factor infertility.Semin Reprod Med. 2014 Jul;32(4):306-12. doi: 10.1055/s-0034-1375183 (View)
Levine BA, Grifo JA. Intrauterine insemination and male subfertility. Urol Clin North Am. 2008 May;35(2):271-6, ix. doi: 10.1016/j (View)
Mette Petri Lauritsen, Pernille Fog Svendsen, Anne Zedeler, Anna Klajnbard, [Intrauterine insemination with or without ovarian stimulation is often a first-choice treatment for infertility] Ugeskr Laeger. 2021 Nov 29;183(48):V04210377 (View)
FAQs from users: 'When is AI recommended?', 'Can the same sperm donor be used for a second pregnancy?', 'What are the causes of failure of artificial insemination?', 'I have tubal patency in only one tube. Can I become a mother through IUI?', 'Is preparation necessary before artificial insemination?', 'Can you undergo IUI with moderate asthenozoospermia?', 'What are the risks of artificial insemination?' and 'How is ovulation monitored to determine the best day for insemination?'.
Authors and contributors






Hi, I’m writing to see if you can help me. I’ve been with my husband for three years, but I can’t get pregnant.
My husband got the following results in his spermiogram test:
ph 7.6
color: white opalescent appearance, semi-viscous
volume , 7.80
viscosity: 7.20
liquefaction 20
agglutination 0
observations: hyperspermia and azoospermia ..
Is my husband sterile? Will I be able to get pregnant?
Does NHS cover the costs of AI?
If you’re eligible for fertility treatment on the NHS or not varies across the UK as well as the eligibility criteria.
Contact your GP or your local clinical commissioning group for further advice.
Best wishes,
Romina
Hi there,
do US insurances cover the cost for single women who need AI?
Hi Mara,
this question is difficult to answer. Each insurance has its own criteria as to whom grant insurance coverage and under which conditions.
It’s best to directly contact your insurance company for a more accurate answer.
Wish you all the best!