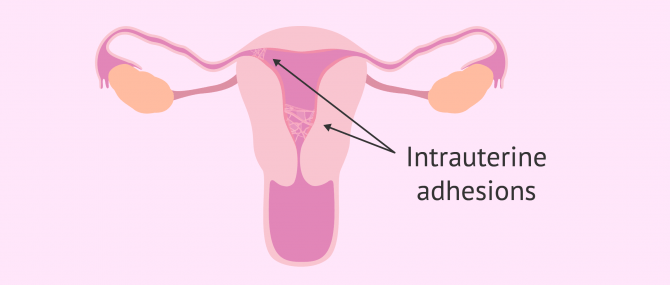
The Asherman's syndrome, or intrauterine adhesions, is a uterine disease characterized by the formation of adhesions (scar tissue) inside de uterus. In many cases, the uterus walls get distorted and sometimes stuck to each other. Therefore, for its diagnosis, it is necessary to perform an ultrasound to evaluate the state of the uterus.
The extent of the adhesions defines whether the case is mild, moderate, or severe. When the uterus walls get stuck, it can lead to serious infertility issues. The adhesions can be thin or thick, spotty in location, or confluent. In other cases, adhesions only occur in a small portion of the uterus.
Provided below is an index with the 9 points we are going to expand on in this article.
- 1.
- 2.
- 2.1.
- 2.2.
- 2.3.
- 3.
- 4.
- 5.
- 5.1.
- 5.2.
- 5.3.
- 5.4.
- 5.5.
- 5.6.
- 6.
- 7.
- 8.
- 9.
Causes of uterine adhesions
Asherman syndrome occurs when the normal healing process in the uterus is initiated. Most commonly, intrauterine adhesions occur after a dilation and curettage, performed because of a miscarriage. The practice of curettage after the loss of a pregnancy is the most common cause of Asherman syndrome.
Bleeding from a cesarean section or natural delivery can also cause scarring. Myomectomy or other gynecological conditions can also cause this syndrome.
These traumas cause, as in any situation, a subsequent healing process in which scar tissue is generated. This tissue has a high adhesive capacity due to its high content of fibrous filaments. The uterus walls get stuck together or get distorted. This fact compromises the uterus's main function: gestate.
Asherman syndrome is, therefore, an acquired condition. Nobody is born with it, but it occurs as a result of a previous clinical case.
How is the diagnosis made?
To determine if the woman suffers from this disease, the gynecologist must carry out several tests to see if there are adhesions through a series of tests detailed below.
It is very important to have the patient's clinical history in mind. It must be checked whether the patient has previously undergone curettage or gynecological operations since, in the case of a curettage after spontaneous abortion, there is an 8% chance of contracting Asherman syndrome. This risk may increase by up to 30% if 3 scrapes have been performed.
Ultrasonography
Ultrasonography or ultrasound is a diagnostic test that takes pictures of the inside of the body. In this case, transvaginal ultrasonography must be inserted through the vagina and into the uterus to observe this cavity.
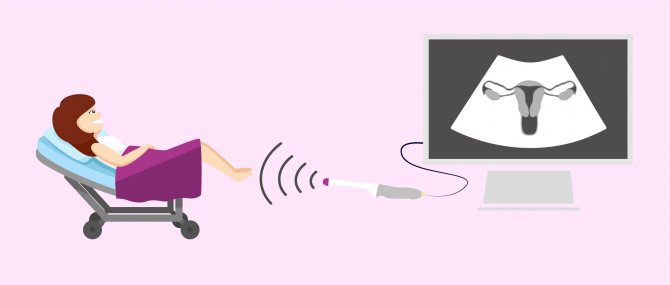
This is usually done in the first instance, as it is simple, non-invasive, and can easily be performed in consultation. However, sometimes its results are not conclusive due to the difficulty in interpreting the images obtained. Therefore, it is necessary to resort to more specialized techniques.
Hysterosalpingogram (HSG)
This medical test consists of a radiograph combined with the use of a contrast medium. This fluid is essential in this test, as it is introduced into the uterus and expands throughout the cavity until it reaches the fallopian tubes and is expelled into the peritoneal space. In this way, the contrast agent "draws" the shape of the uterus and tubes. Once the contrast has been injected, an x-ray is taken.
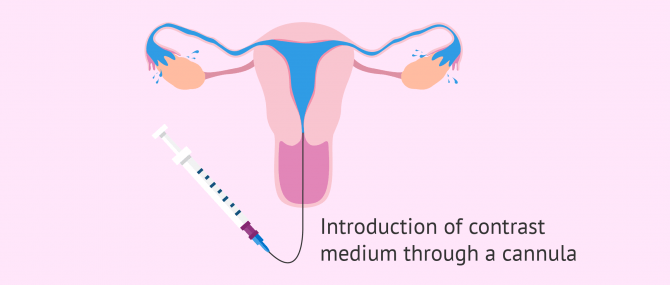
Hysterosalpingogram is a more complete test than ultrasound, as the presence of adhesions, obstructions, or alterations such as fibroids or polyps is easier to detect.
However, although it does not require anesthesia or is not very painful, it is a complicated procedure that must be scheduled and performed in a specialized unit.
Hysteroscopy
Finally, if the diagnosis after the above tests remains unclear, a diagnostic hysteroscopy may be performed. This test consists of inserting a camera into the uterine cavity to observe it.
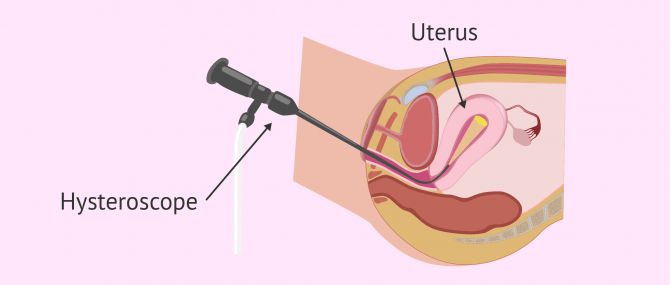
The determination of Asherman's syndrome is much clearer with this test since the visualization of the adhesions is more direct. This is why hysteroscopy is the ideal method for its diagnosis.
Symptoms of Asherman's syndrome
The most common symptoms of Asherman Syndrome are:
- Menstrual disorders: Long periods of no menstrual bleeding (amenorrhea) usually occur, mainly because adhesions block blood clots from the uterus to the vagina.
- Pelvic or abdominal pain: As a result of the retention of menstrual bleeding, women may experience pain during periods or between periods.
- Retrograde Menstruation: Preventing endometrial tissue from leaving can cause endometrial tissue to be released retrogressively into the abdominal cavity through the fallopian tubes. Blood released can settle into cysts or endometriomas.
- Recurrent miscarriage: the deformation of the uterine cavity as a result of the adhesion of its walls makes the correct development of gestation impossible. If this condition is not treated, recurrent miscarriage may occur.

These symptoms are very common and may be related to many other gynecological pathologies in addition to Asherman syndrome. Therefore, extensive testing is necessary to determine the cause of these signs.
However, these symptoms are much more likely to indicate Asherman's syndrome if they occur suddenly after curettage, curettage, or other uterine surgery.
What is the treatment like?
If the results of the above tests show that you have this syndrome, surgery is necessary, since this condition can be quite painful and have very negative consequences for a woman's fertility.
Assisted procreation, as any other medical treatment, requires that you rely on the professionalism of the doctors and staff of the clinic you choose. Obviously, each clinic is different. Get now your Fertility Report, which will select several clinics for you out of the pool of clinics that meet our strict quality criteria. Moreover, it will offer you a comparison between the fees and conditions each clinic offers in order for you to make a well informed choice.
Treatment for Asherman syndrome involves the removal and cauterization of adhesions so that the uterus regains its normal shape and size. Generally, this procedure is performed using a surgical hysteroscopy during which, in addition to the optical system through which the uterus is visualized, specialized microsurgical instruments are used to section the adhesions.
Once the scar tissue has been removed, the uterine cavity must remain expanded to prevent the recurrence of adhesions. There are several methods available:
- Intrauterine balloon: is a small probe that is inserted into the uterus and, once positioned inside, expands, keeping the uterine walls separate, while they heal.
- Oestrogen Treatment: Oestrogen-based pharmacological treatment may also be necessary during the days following surgical hysteroscopy. This hormone stimulates the natural growth of the initially damaged endometrial tissue, preventing the growth of the tissue and causing adhesions.
- Continuous hysteroscopies: some doctors recommend more exhaustive check-ups for women who have suffered this syndrome since they have a greater predisposition to suffer it again.

However, the doctor will probably also prescribe hormonal treatment with estrogens for the patient.
On the other hand, treatment may require more thorough examinations and more hysteroscopies for women who have suffered from this syndrome, as there is a possibility of recurrence.
FAQs from users
Can I know if I have Asherman’s syndrome by just checking my hormone levels?
No, it can be suspected by ultrasound, and diagnosed by hysteroscopy.
Can Asherman syndrome be completely cured?
It depends on the degree of the condition, the more severe it is, the more likely the adhesions will reappear in the patient.
Can intrauterine adhesions appear after a cesarean section?
Yes, cesarean section may be a reason for intrauterine adhesions to develop because it is a surgical procedure that requires healing after the incisions made to extract the baby.
Is a pregnancy viable with Asherman Syndrome?
The presence of intrauterine adhesions seriously compromises the fact that a pregnancy can develop normally. To do this, it is necessary to remove the tissues before the woman becomes pregnant.
Can Asherman syndrome be the cause of endometriosis?
It is possible that blood clots retained by the adhesions can be evacuated retrograde into the abdominal cavity, landing on the tubes or ovaries and forming cysts. Suffering from Asherman syndrome may be a reason to develop endometriosis, as the retrograde menstruation mechanism results precisely from it.
Is Asherman's syndrome related to tuberculosis?
Yes, Asherman's syndrome can appear after some infections such as genital tuberculosis, which can lead to fertility problems in women.
Recommended readings
According to most clinical sources, performing a curettage is the most frequent cause of contracting this syndrome. Curettage is a surgical procedure that is often necessary after the loss of a pregnancy. We tell you what it consists of in the link below: Uterine curettage: procedure, recovery, and complications.
The formation of adhesions causes the uterus to narrow and its internal cavity to shrink. This obviously prevents a pregnancy from being carried to term, as the fetus cannot develop normally due to the lack of space. As a result, a miscarriage ends up occurring. If you want to know what signs are symptoms of miscarriage and what other causes can provoke it, click on the following link: Miscarriage: symptoms, causes, and consequences.
At the end of this post, we have commented that the incurable Asherman's syndrome arises from the total destruction of the endometrium. This tissue is very important in a woman's reproductive cycle. We recommend that you read the following article to learn more about it: What is the endometrium? - Thickening, types, and pathologies
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Di Guardo F, Della Corte L, Vilos GA, Carugno J, Török P, Giampaolino P, Manchanda R, Vitale SG. Evaluation and treatment of infertile women with Asherman syndrome: an updated review focusing on the role of hysteroscopy. Reprod Biomed Online. 2020 Jul;41(1):55-61.
Doroftei B, Dabuleanu AM, Ilie OD, Maftei R, Anton E, Simionescu G, Matei T, Armeanu T. Mini-Review of the New Therapeutic Possibilities in Asherman Syndrome-Where Are We after One Hundred and Twenty-Six Years? Diagnostics (Basel). 2020 Sep 17;10(9):706.
Dreisler E, Kjer JJ. Asherman's syndrome: current perspectives on diagnosis and management. Int J Womens Health. 2019 Mar 20;11:191-198.
Khan Z, Goldberg JM. Hysteroscopic Management of Asherman's Syndrome. J Minim Invasive Gynecol. 2018 Feb;25(2):218-228.
March CM. Asherman's syndrome. Semin Reprod Med. 2011 Mar;29(2):83-94.
Salazar CA, Isaacson K, Morris S. A comprehensive review of Asherman's syndrome: causes, symptoms and treatment options. Curr Opin Obstet Gynecol. 2017 Aug;29(4):249-256.
Smikle C, Yarrarapu SNS, Khetarpal S. Asherman Syndrome. 2021 Jan 5. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan–.
FAQs from users: 'Can I know if I have Asherman’s syndrome by just checking my hormone levels?', 'What are the causes of Asherman syndrome?', 'Can Asherman syndrome be completely cured?', 'Can intrauterine adhesions appear after a cesarean section?', 'Is a pregnancy viable with Asherman Syndrome?', 'Can Asherman syndrome be the cause of endometriosis?' and 'Is Asherman's syndrome related to tuberculosis?'.
Authors and contributors





More information about Cristina Algarra Goosman

Hello, I am going to have a cesarean section and I have read that it can produce this syndrome, is that so? How can I avoid it?
Hi Robbie,
Cesarean section can cause pelvic adhesions if not performed correctly. Since this surgical intervention produces a scarring process in the incisions.
In general, if the procedure is performed correctly and active recovery is attempted, pelvic adhesions will be reduced. I recommend you read the following article: Cesarean section.
I hope I have helped you,
Best regards
Hello, I had a curettage a few months ago for an abortion I had and since then I do not have my period well and I have intense pain in the pelvic area. could it be this syndrome?
Hello Albannie,
Menstrual disturbances and pelvic pain may be indicative of Asherman’s syndrome but they are not symptoms that can be reduced to this alone.
For this, I recommend that you see a doctor so that he/she can make a diagnosis and therefore prescribe treatment. This can combine both surgical intervention and hormone supplementation treatment.
I hope all goes well,
Best regards