Huntington's disease, also known as Huntington's choreais a hereditary, degenerative neurological disorder. This disease affects both men and women.
It is a pathology caused by neuronal wasting in certain areas of the brain. Huntington's disease most commonly appears in adulthood, but there are also cases detected in adolescence.
Those with Huntington's chorea can have a baby, although it is important to receive genetic counseling beforehand. One option would be to resort to in vitro fertilization with preimplantation genetic diagnosis to prevent the transmission of the disease to the offspring.
Provided below is an index with the 10 points we are going to expand on in this article.
- 1.
- 1.1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 6.1.
- 6.2.
- 6.3.
- 6.4.
- 7.
- 8.
- 9.
- 10.
What is huntington's chorea?
Huntington's chorea, Huntington's disease or chronic progressive chorea is a neurodegenerative and hereditary pathology that is transmitted from parents to children. The disease is named after an American physician who discovered it in 1872, Dr. George Huntington.

The most common form of this disease is the one that appears in adulthood. What happens is that patients are born with the genetic alteration, but it is not until the age of 30-40 years that the typical clinical manifestations of Huntington's disease emerge.
The most prominent feature of the disease is the neuronal degeneration in several points of the brain, so there will be an affectation at the level of mobility and coordination.
What symptoms does it cause?
At the onset of the disease, symptoms are usually subtle. However, in adulthood, around the age of 30-40 years, the clinical manifestations of Huntington's disease are usually more noticeable.
Each of the signs of Huntington's chorea is detailed below:
- Chorea or involuntary movements
- these are rapid and abrupt movements that occur without any apparent cause. This type of movement can occur in different areas of the body, such as the legs, arms or even the face.
- Bradykinesia
- unlike chorea, bradykinesia consists of voluntary movements that are performed slowly.
- Behavioral and personality changes
- that is usually one of the first symptoms of Huntington's chorea. Apathy, irritability or being impulsive are some of the characteristics of this disease.
- Loss of cognitive skills
- people suffering from Huntington's disease often have difficulty concentrating, forgetfulness, etc.
- Anxiety and depression
- problems at the psychiatric level is also one of the symptoms of the disease.

Apart from all these symptoms, difficulty in speech, problems in swallowing food, muscle stiffness, etc. have also been seen. However, these symptoms associated with Huntigton's disease may vary from one person to another and also depending on the degree of severity, speed at which the disease progresses, etc.
Causes of Huntington's disease
It is a monogenic disease, i.e. Huntington's disease is caused by alterations in a single gene (the HTT gene). In addition, its inheritance is autosomal dominant, which means that only one copy of the altered gene is necessary for the individual to have Huntington's chorea. Although Huntington's chorea is most often inherited, there are a small percentage of cases where the disease occurs de novo.
The gene that causes Huntington's disease is located on the short arm of chromosome 4 and encodes a protein known as huntingtin huntingtin. When a gene mutation occurs, what happens is that there are more CAG triplet repeats in the HTT gene than there should be.
A healthy person has 10-27 repeats of the CAG triplet; whereas if he/she has inherited the Huntington's disease-causing mutation, he/she will have 36-120 repeats. If she is only a carrier of the disease, she will have between 27 and 35 repeats of the triplet.
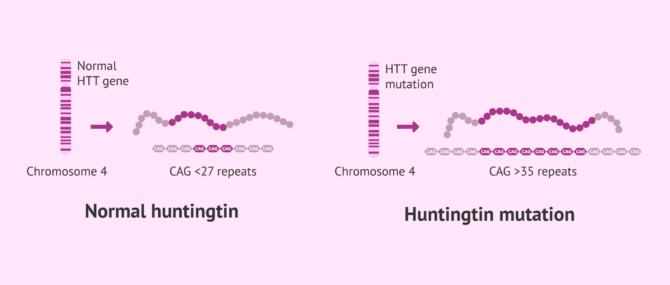
Notably, as the gene mutation is passed on to offspring, the number of CAG triplet repeats increases. As a result, symptoms of Huntington's disease may appear earlier and earlier.
How is huntington's disease diagnosed?
The diagnosis of Huntington's disease begins with a physical examination where an attempt is made to detect motor, sensory and psychiatric symptoms, as well as a neuropsychological analysis where aspects related to memory, reasoning, mental agility, etc. are evaluated. In addition, it is important to know the family history.
If Huntington's chorea is suspected, the specialist will order complementary imaging tests, such as a CT scan or MRI. The images of the brain obtained through these tests will inform the specialist of possible changes detected and will rule out other pathologies that could be the cause of the symptoms manifested.

Confirmation of the diagnosis of Huntington's chorea is through genetic testing. To do this, only a blood sample will be taken from the patient and his DNA will be extracted to study the number of CAG triplet repeats in the gene coding for Huntingtin.
Treatment
Huntington's disease has no definitive cure, but there are different therapies to control the symptoms, although not to stop the neurological deterioration caused by this disorder.
The following are some of the therapies to alleviate the clinical manifestations of Huntington's disease:
- Use of medications such as benzodiazepines or tetrabenazine that help control chorea, i.e. involuntary and jerky movements. In addition, antidepressants or mood stabilizers, among other drugs, are also indicated.
- Psychotherapy to address behavioral problems.
- Physiotherapy focused on improving muscle strength, coordination in movements, etc.
In addition, speech therapy can be performed with the help of a speech therapist since Huntignton's disease can affect speech and/or swallowing.
Huntington's disease and pregnancy
Thanks to advances in medicine, people who are carriers of Huntington's disease can have offspring without passing on the mutation. To do so, they must resort to assisted reproduction techniques, specifically in vitro fertilization with preimplantation genetic diagnosis(IVF with PGD).
In this case, fertilization occurs in the laboratory and the embryos generated are genetically analyzed. In this way, the genetically altered embryos will be discarded, and only healthy embryos will be transferred and, therefore, without the Huntingtin gene mutation.
To perform a PGD, one should undergo IVF as the main treatment. If you are looking for a clinic to get started, we recommend that you generate your individual Fertility Report now. It is a useful, simple tool that, in just 3 steps, will give you a list of the clinics that have passed our rigorous selection process. You will receive an email in your inbox with a report that contains tips and recommendations to get started.
In addition to IVF with PGD, there is also the option of performing the amniocentesis technique once pregnancy has been achieved. However, this invasive prenatal test poses more risks to the fetus.
FAQs from users
Can the transmission of Huntington's disease be prevented?
Yes, Huntington's chorea can be prevented by achieving pregnancy through in vitro fertilisation (IVF) with pre-implantation genetic diagnosis (PGD).
With PGD, only healthy embryos that do not contain the Huntington's disease-causing gene mutation will be transferred.
Can I become a mother if I have Huntington's disease?
Huntington's disease is an inherited pathology that is characterised by its onset in adulthood. In many cases, when the patient debuts and is diagnosed with this pathology, he or she has already had natural decency. This is why the majority of cases presented in assisted reproduction are second generation patients with a history of this disease.
The most common way to proceed is through In Vitro Fertilisation treatment that allows the laboratory to carry out a Genetic Diagnosis. Through this technique, embryos with the disease can be detected and discarded. Only those embryos free of the disease will be transferred to the patient.
Another possibility is the donation of donated gametes (eggs or sperm), thus eliminating the possibility of inheriting the pathology.
Huntintong disease presents a challenge for patients with a family history of the disease who wish
For this purpose, a sophisticated protocol has been developed to avoid the transmission of the disease to the embryos created by IVF and, at the same time, to maintain the right of the parent with the possibility of being a carrier not to want to be informed of the possibilities of having the Huntington's disease gene. In this way, the genes of the parent with the possibility of being affected by the disease are analysed, and if necessary, the embryos undergo genetic diagnosis. As a result, it is ensured that the embryos to be transferred are completely healthy and free of Huntington's disease while preserving the right of the possible carrier to not want to know if he/she has inherited the disea
Read more
What type of inheritance does Huntington's chorea have?
Huntington's disease, or Huntington's chorea, named after its discoverer, is a genetic condition with autosomal dominant inheritance. This means that only one copy of the altered gene is required to inherit the disease.
Does Huntington's disease affect fertility?
Huntington's disease is a rare inherited neurological disorder that affects the central nervous system. It is inherited through a specific genetic mutation. Given that it is a genetic disease, it is understandable that concerns are raised about its effects on reproductive health, including fertility.
In terms of direct impact on fertility, Huntington's disease itself is not associated with decreased fertility. People with Huntington's disease are generally able to conceive naturally. Fertility problems related to Huntington's disease are usually secondary and linked to neurological and health complications in later stages of the disease. Therefore, the initial reproductive capacity is usually not directly affected.
However, several issues are critical to consider when it comes to family planning in Huntington's disease. The biggest dilemma lies in the transmission of the condition to offspring. Since it is an autosomal dominant genetic disorder, there is a 50% chance of passing on the mutated gene to offspring. This raises a legitimate concern for couples in which one or both parents are carriers of the disease gene.
In these cases, many couples resort to genetic counseling and preconception genetic testing to determine the risk of transmitting the disease to their offspring. Depending on the result, they may opt for in vitro fertilization (IVF) with preimplantation genetic diagnosis (PGD) to select embryos that do not carry the mutation. This prevents the disease from being transmitted to the offspring.
Suggested for you
For information about other diseases that can be prevented by PGD, please visit the following article: What are monogenic diseases - Avoiding them with PGD.
In addition, if you would like to know more about this complementary assisted reproduction technique to analyze embryos, then we invite you to access the following link: What is preimplantation genetic diagnosis or PGD?
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Amy Kim, Kathryn Lalonde, Aaron Truesdell, Priscilla Gomes Welter, Patricia S Brocardo, Tatiana R Rosenstock, Joana Gil-Mohapel. New Avenues for the Treatment of Huntington's Disease. Int J Mol Sci. 2021 Aug 4;22(16):8363. doi: 10.3390/ijms22168363 (View)
Eric Fields, Erik Vaughan, Deepika Tripu, Isabelle Lim, Katherine Shrout, Jessica Conway, Nicole Salib, Yubin Lee, Akash Dhamsania, Michael Jacobsen, Ashley Woo, Huijing Xue, Kan Cao. Gene targeting techniques for Huntington's disease. Ageing Res Rev. 2021 Sep;70:101385. doi: 10.1016/j.arr.2021.101385. Epub 2021 Jun 5 (View)
Jae Wook Hyeon, Albert H Kim, Hiroko Yano. Epigenetic regulation in Huntington's disease. Neurochem Int. 2021 Sep;148:105074. doi: 10.1016/j.neuint.2021.105074 (View)
James F Gusella, Jong-Min Lee, Marcy E MacDonald. Huntington's disease: nearly four decades of human molecular genetics. Hum Mol Genet. 2021 Oct 1;30(R2):R254-R263. doi: 10.1093/hmg/ddab170 (View)
Monia Barnat, Mariacristina Capizzi, Esther Aparicio, Susana Boluda, Doris Wennagel, Radhia Kacher, Rayane Kassem, Sophie Lenoir, Fabienne Agasse, Barbara Y Braz, Jeh-Ping Liu, Julien Ighil, Aude Tessier, Scott O Zeitlin, Charles Duyckaerts, Marc Dommergues, Alexandra Durr, Sandrine Humbert. Huntington's disease alters human neurodevelopment. Science. 2020 Aug 14;369(6505):787-793. doi: 10.1126/science.aax3338. Epub 2020 Jul 16 (View)
Nicholas E Karagas, Natalia Pessoa Rocha, Erin Furr Stimming. Irritability in Huntington's Disease. J Huntingtons Dis. 2020;9(2):107-113. doi: 10.3233/JHD-200397 (View)
Nóra Zsindely, Fruzsina Siági, László Bodai. DNA Methylation in Huntington's Disease. Int J Mol Sci. 2021 Nov 25;22(23):12736. doi: 10.3390/ijms222312736 (View)
Sarah J Tabrizi, Carlos Estevez-Fraga, Willeke M C van Roon-Mom, Michael D Flower, Rachael I Scahill, Edward J Wild, Ignacio Muñoz-Sanjuan, Cristina Sampaio, Anne E Rosser, Blair R Leavitt. Potential disease-modifying therapies for Huntington's disease: lessons learned and future opportunities. Lancet Neurol. 2022 Jul;21(7):645-658. doi: 10.1016/S1474-4422(22)00121-1 (View)
Sarah J Tabrizi, Rhia Ghosh, Blair R Leavitt. Huntingtin Lowering Strategies for Disease Modification in Huntington's Disease. Neuron. 2019 Mar 6;101(5):801-819. doi: 10.1016/j.neuron.2019.01.039 (View)
Sigita Lesinskienė, Darja Rojaka, Rūta Praninskienė, Aušra Morkūnienė, Aušra Matulevičienė, Algirdas Utkus. Juvenile Huntington's disease: two case reports and a review of the literature. J Med Case Rep. 2020 Oct 1;14(1):173. doi: 10.1186/s13256-020-02494-7 (View)
T Maiuri, C E Suart, C L K Hung, K J Graham, C A Barba Bazan, R Truant. DNA Damage Repair in Huntington's Disease and Other Neurodegenerative Diseases. Neurotherapeutics. 2019 Oct;16(4):948-956. doi: 10.1007/s13311-019-00768-7 (View)
FAQs from users: 'Can the transmission of Huntington's disease be prevented?', 'Can I become a mother if I have Huntington's disease?', 'What type of inheritance does Huntington's chorea have?' and 'Does Huntington's disease affect fertility?'.
Authors and contributors

In addition, the doctor has participated in several scientific publications and lectures, as well as taking complementary training courses More information about John Peay Pinacho


