Male infertility is the inability of male semen to provoce pregnancy. There are several causes that can lead men to infertility, including the prestesticular factor.
Male sterility caused by pretesticular factor is due to problems in the endocrine system, resulting in incorrect sperm formation. In this way, defects in the morphology, quantity or mobility of the spermatozoa will be produced.
Sperm are formed by a complex hormonal system that begins in the brain and ends in the testicle, and which is self-regulating. Various hormones, Y chromosome genes and intratesticular autocrine and paracrine factors will be involved in its formation.
The most frequent pretesticular factors include diabetes, thyroid problems, hyperprolactinemia, etc.
Provided below is an index with the 8 points we are going to expand on in this article.
- 1.
- 2.
- 3.
- 3.1.
- 3.2.
- 3.3.
- 3.4.
- 3.5.
- 4.
- 4.1.
- 4.2.
- 4.3.
- 5.
- 6.
- 7.
- 8.
Hypothalamus-hypophysis testicle hormone axis
The hypothalamus of the man in the brain secretes a hormone called GnRH (gonadotropin-releasing hormone) that acts on the pituitary gland, a small neuroendocrine gland.
On the other hand, the pituitary gland is responsible for secreting the hormones necessary for the formation of sperm: FSH (follicle stimulating hormone) and LH (luteinizing hormone).
A neuroendocrine gland is a type of gland where nerve orders are combined with neurons and hormonal signals, that is, they are responsible for sending hormones to the blood in response to stimulation by the nervous system.
Within the testicle, spermatogonies are stem cells that specialize in differentiating themselves to give rise to sperm. However, there are also other cells that are necessary for the regulation of the process and for correct hormonal communication.
In general, the cells of the testicle are:
- Leydig cells: have specific membrane receptors for LH (luteinizing hormone). When LH reaches the Leydig cells, the secretion of testosterone is produced, a hormone necessary for the formation of spermatozoa.
- Sertoli cells: these are the support cells and when FSH arrives they also act on the Leydig cells to secrete more testosterone.
- Germ cells or spermatogonies: stem cells that will give rise to sperm by successive divisions. For this, they need the existence of hormonal stimuli.
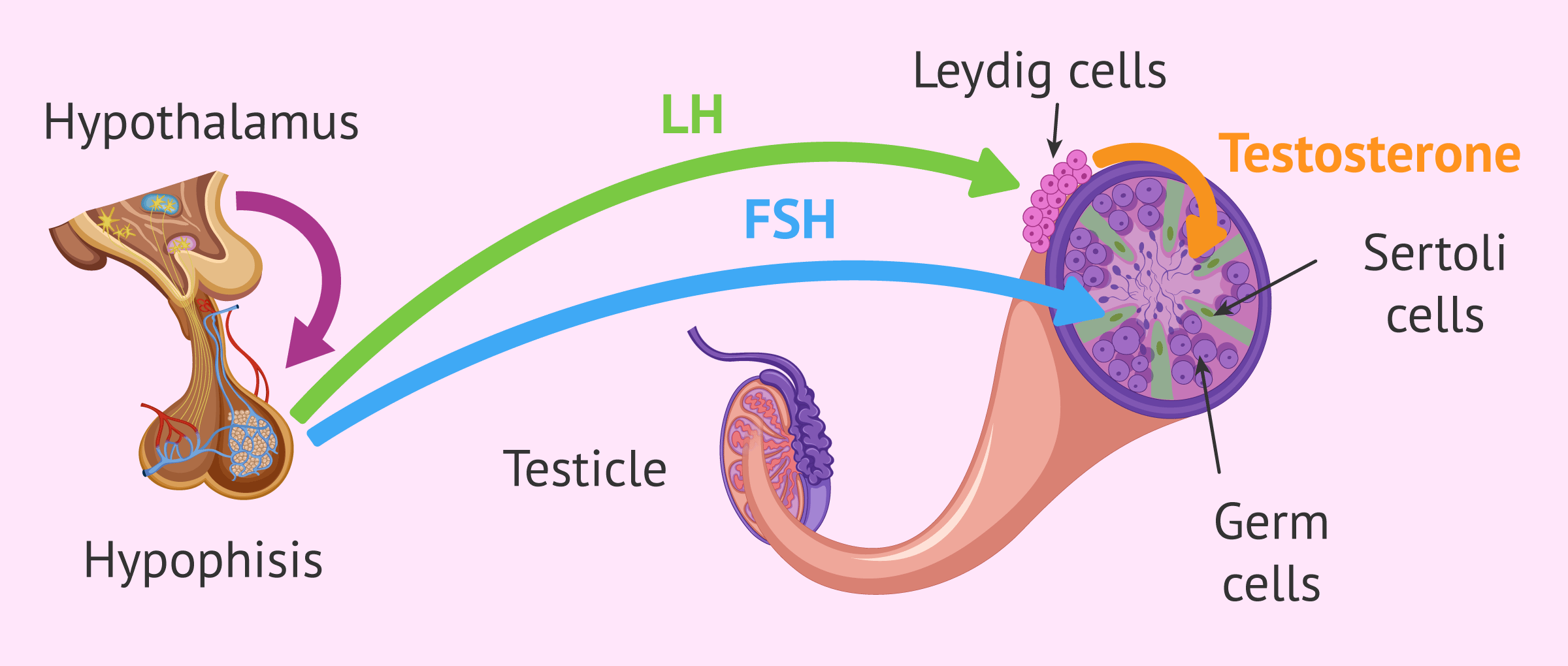
When testosterone levels are high and sufficient, the secretion of the hormone LH is inhibited, which reaches the brain through the blood and tells the brain that the levels are adequate. In this way, the secretion of GnRH and FSH will be regulated, maintaining the appropriate levels of hormones for the formation of spermatozoa.
Basic male assessment
In short, a basic evaluation that will be carried out on the man who comes to a center for infertility problems would be:
- Medical and sexual history
- general examination of the patient.
- Semen Analysis
- determining the different parameters of the semen such as concentration, mobility or morphology in order to check its quality.
- Endocrine evaluation
- to determine primary testicular failure. This evaluation consists of a blood test where the parameters of different hormones are determined.
- Genetic testing
- allows us to rule out alterations in the karyotype or microdeletions in the Y chromosome, which are common in patients with alterations in spermatogenesis.
- Specialized tests
- DNA fragmentation.

If you would like to read more in-depth information on this topic, we recommend you visit the following article: Male Fertility Testing - How Do You Know if You Are Infertile?
Causes
As we have seen, the hormonal process has to be perfectly adjusted so that the signals result in an adequate formation of sperm. Some causes of pretesticular factor infertility are shown below.
Hypogonadotropic hypogonadism
Hypogonadism is an alteration characterized by a failure of the testicles to secrete testosterone and/or sperm.
In the case of hypogonadotropic hypogonadism, also called primary hypogonadism, the hypothalamus and pituitary gland function normally. The problem is that Leydig cells are not capable of generating enough testosterone, despite having the necessary amount of FSH. As a result, sperm are not generated correctly. Therefore, the problem here is found in a primary, congenital or acquired lesion in the testicles.
The causes can be diverse and include:
- Genetic alterations, such as Klinefelter Syndrome, Reifenstein Syndrome, Ullrich-Noonan Syndrome, etc.
- Systemic diseases, such as chronic kidney failure, Liver cirrhosis, etc.
- Infectious diseases.
- Alteration in the gonadotropin receptor.
- Others such as autoimmune testicular failure or anorchia, i.e. absence of testicles.

As a consequence of hypergonadotropic hypogonadism, the testicles may be small and reflected by oligozoospermia or azoospermia, meaning low or complete absence of sperm respectively.
The treatment consists of the direct application of testosterone. A stimulation of the testicle would not make sense in this case, since the production of FSH and LH at the cerebral level is adequate.
Hypogonadotropic hypogonadism
To be more specific, the term hypogonadotropic hypogonadismrefers to a type of hypogonadism caused by testicular failure secondary to a hypothalamic-pituitary disease. Generally speaking, this means that it can be attributed to alterations of the hypothalamus or pituitary gland.
Some of the risk factors are:
- Damage to the pituitary gland or hypothalamus from surgery, injury, tumor, radiation, etc.
- Genetic abnormalities.
- By hemochromatosis, i.e., an accumulation of iron in the body.
- Intense stress.
- Prolonged chronic illnesses.
- Use of drugs, steroid medications, or opioids
There is an inheritable alteration of this hypogonadism called kallmann syndrome in which patients may also have an absence of smell (anosmia).
The treatment will depend on the origin of the problem, but a possible solution would be a hormone replacement treatment that stimulates the action of the testicle and increases the concentrations of sex hormones.
Diabetes
Diabetes is characterised by an increase in blood glucose levels leading to a reduction in sperm quality. There will be alterations in the DNA and defects in its repair, which leads to an accumulation of damage by fragmentation in the DNA of the spermatozoa.
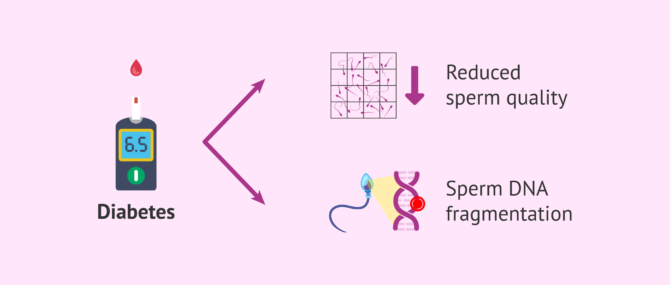
Sterility can be attributed to metabolic changes or secondary to other complications, such as nerve damage or blood vessel involvement in uncontrolled and untreated diabetes.
Thyroid problems
The thyroid gland is an endocrine gland that secretes various hormones. Hypothyroidism or hyperthyroidism, i.e. a defect or excess production of thyroid hormone respectively, causes alterations in various metabolic processes. All this can have consequences on the maturation of the sperm and affect the quality of the sperm, causing a decrease in the degree of fertility.
It should be kept in mind that, in the case of goiter or the appearance of nodules where an anatomical alteration of the thyroid gland is produced but not functional, fertility is not affected.
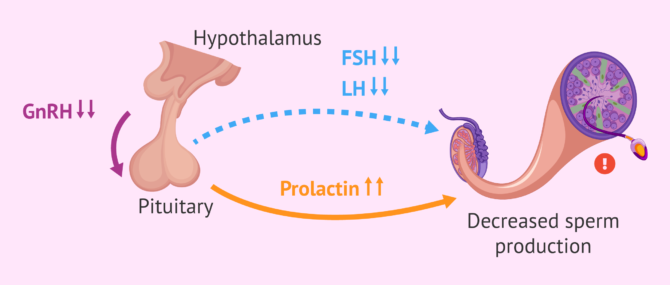
Hyperprolactinemia
Prolactin is a disorder characterized by elevated levels of prolactin, a hormone secreted in the front of the pituitary gland. It is usually derived from a hypogonadotropic hypogonadism.
In the sperm production process, prolactin is essential. Increased prolactin levels lead to reduced secretion of FSH and LH. As a result, oligozoospermia may occur, i.e. a decrease in sperm count or even erectile dysfunction and loss of sexual desire.
The diagnosis is carried out by means of a blood test in the morning and avoiding stress situations, as it is part of the stress hormone circuit. If positive, a second determination is made.
Once hyperprolactinemia has been diagnosed and its cause (hypothyroidism, use of a medication, pituitary adenoma, etc.), treatment must be established in order to restore reproductive capacity by normalizing prolactin levels.
FAQs from users
Can endocrine-related male sterility be cured?
For the correct function of male fertility, normal hormonal stimulation is essential to achieve the correct formation of sperm and normal sexual function. Various hormones are involved in male endocrine function and the balance between them is essential.
There are illnesses or hormonal alterations that can affect male fertility, which is why an adequate hormonal evaluation is very important in situations of male sterility.
Endocrine diseases that affect fertility in men are multiple, but the most common are hypogonadotrophic hypogonadism, benign androgenic hyperplasia and hypothalamic dysfunctions. Others such as obesity and elevated prolactin also play an important role in male sterility. Most of these disorders have medical treatment with a very good response, being possible in most cases to recover fertility and achieve pregnancy.
Can hypothyroidism cause sterility in men?
Hypothyroidism or thyroid problems can be a cause of infertility in men, since it causes alterations in the sperm maturation process due to problems in the metabolic processes involved. For this reason, it is advisable to carry out an endocrine study.
Could a presticular factor such as a pituitary adenoma be a cause of male sterility?
Yes, a pituitary adenoma could be a cause of male sterility.
Pituitary adenoma is a tumor in the cells that form the pituitary gland which will affect the secretion of the various hormones, either by an excess or a defect in their production. As a consequence, the sperm production process is altered.
Suggested for you
For more information about other causes of male sterility due to testicular factors, read on here: Testicular Disorders & Infertility - Impact on Reproductive Function.
Besides, if you’re interested in the effects of anabolic steroid consumption, we recommend you this post: Anabolic Steroids: Do They Cause Male Sterility?
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
A Ferlin, A E Calogero, C Krausz, F Lombardo, D Paoli, R Rago, C Scarica, M Simoni, C Foresta, V Rochira E Sbardella, S Francavilla, G Corona. Management of male factor infertility: position statement from the Italian Society of Andrology and Sexual Medicine (SIAMS) : Endorsing Organization: Italian Society of Embryology, Reproduction, and Research (SIERR). J Endocrinol Invest. 2022 May;45(5):1085-1113. doi: 10.1007/s40618-022-01741-6 (View)
Krausz C. Male infertility: pathogenesis and clinical diagnosis. Best Pract Res Clin Endocrinol Metab. 2011 Apr;25(2):271-85. doi: 10.1016/j.beem.2010.08.006 (View)
Devoto E, Madariaga M, Lioi X. Causes of male infertility. The contribution of the endocrine factor. Rev Med Chil. 2000 Feb;128(2):184-92.
Condorelli RA, La Vignera S, Mongioì LM, Alamo A, Calogero AE. Diabetes Mellitus and Infertility: Different Pathophysiological Effects in Type 1 and Type 2 on Sperm Function. Front Endocrinol (Lausanne). 2018 May 25;9:268. doi: 10.3389/fendo.2018.00268 (View)
FAQs from users: 'Can endocrine-related male sterility be cured?', 'Can hypothyroidism cause sterility in men?' and 'Could a presticular factor such as a pituitary adenoma be a cause of male sterility?'.




