
Get Answers from JOFREFIV
In Spain, it is possible to use the same sperm donor for a second pregnancy, provided the requirements established by Law on Assisted Human Reproduction Techniques are met.
Spanish legislation sets a legal limit of six children born in Spain per donor. As long as this limit has not been reached and the clinic (or donor bank) still has available samples from that donor, the same donor may be used for a subsequent pregnancy.
A semenogram and REM are related tests, but they are not the same.
A semenogram —also known as a basic semen analysis— provides an overall assessment of male fertility and is typically the first step in evaluating reproductive potential.
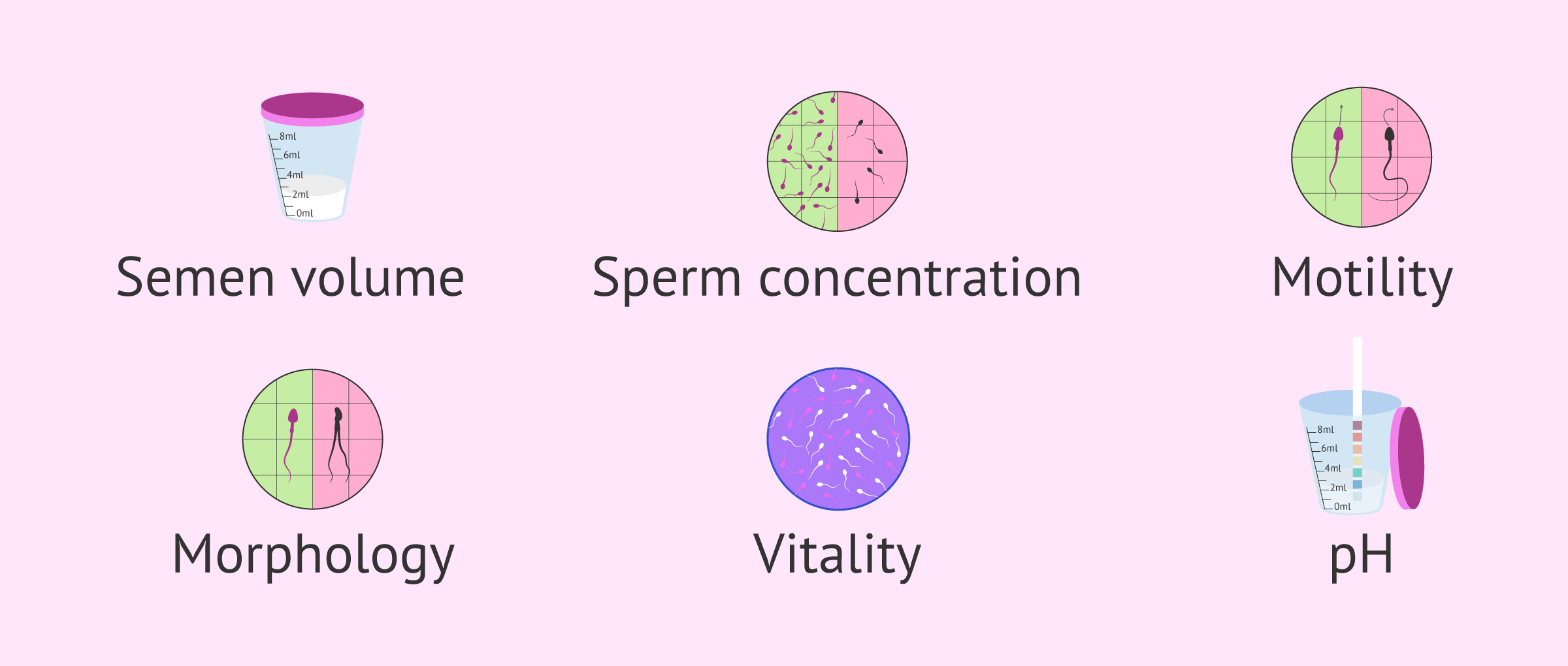
It examines parameters such as:
- Semen volume.
- Sperm concentration.
- Motility.
- Morphology.
- Vitality.
- pH.
REM stands for Recuperación de Espermatozoides Móviles (in Spanish), which translates to Recovered Motile Sperm in English. It is a specialized, preparation technique used in assisted reproduction, often referred to as a "sperm capacitation test".
The result provides the number of motile sperm per milliliter recovered after the washing and centrifugation process of the sample. This parameter is especially important when determining the most appropriate fertility treatment.
In summary, the semenogram offers a complete overview of semen quality, while REM focuses specifically on the number of motile sperm recovered after processing the sample, and plays a key role in treatment planning.
The probability of having no embryos suitable for transfer depends on several factors such as age, ovarian reserve, DNA fragmentation:
- Decreased Ovarian Reserve: in these patientes fewer oocytes are retrieved. Ovarian reserve and ovarian response are inversely related to maternal age; as maternal age increases, both ovarian reserve and response decrease. Consequently, advanced maternal age affects the number of oocytes retrieved, their quality, and the number of embryos available for biopsy.
- Reduced Embryo Yield: a lower starting number of oocytes translates to fewer embryos reaching the blastocyst stage suitable for biopsy. Is important to understand that biopsy for PGT can only be performed on blastocysts; if embryos arrest earlier, they cannot be analyzed.
- Increased Aneuploidy: oocytes from patients with advanced maternal age have a higher risk of chromosomal abnormalities (aneuploidy), further reducing the percentage of "healthy" embryos available for transfer.

Another factor to consider is the quality of the sperm:
- Male factor: high sperm DNA fragmentation can negatively affect the genetic quality of embryos.
If you (or your partner) are a carrier of a structural rearrangement or a monogenic disease, the risk of not having embryos available after PGT will also depend on the probability, in each individual case, of having embryos free of the mutation, and on whether you choose to have them analysed for aneuploidies as well.
In summary, the greater the number of embryos available for PGT, the higher the chances of obtaining healthy embryos suitable for transfer to the uterus.
