After a year (6 months if the woman is over 35-38 years old) of having sexual intercourse seeking pregnancy without success, it is possible that the couple may have fertility problems and, therefore, at that point, it would be advisable for both the man and the woman to undergo the necessary fertility tests.
In the woman's case, the female fertility study basically consists of a hormone analysis, an ultrasound, and a karyotype. It is also possible to perform other tests, such as a hysterosalpingography (HSG). Similarly, the fertility study for women is the same whether it is a female couple or a woman seeking to become a single mother.
Once the fertility study has been completed, it will be possible to apply the most appropriate assisted reproduction treatment to help the woman or couple achieve pregnancy.
Provided below is an index with the 11 points we are going to expand on in this article.
- 1.
- 1.1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 6.1.
- 6.2.
- 7.
- 7.1.
- 7.2.
- 7.3.
- 7.4.
- 7.5.
- 7.6.
- 7.7.
- 8.
- 9.
- 10.
- 11.
When to see a specialist?
When problems conceiving arise, both partners should undergo tests for a fertility study to try to find the cause that is making it difficult for them to become parents.
It is necessary for both to undergo the fertility study, since the origin of infertility can be due to male factors, female factors, or even mixed factors (in both the man and the woman).
In general, it is recommended to see a specialist and perform a fertility study when the couple has been having unprotected sexual intercourse for at least one year and, even so, has not achieved pregnancy. However, this time is reduced to 6 months if the woman is over 35-38 years old.

At that point, it would be advisable for the couple to see a specialist to perform both a female and male fertility study.
Basic female fertility study
Specifically, to diagnose female infertility, the gynecologist opens a medical history and asks the woman about aspects of her reproductive life: whether she has previous children, if she has had any miscarriages, if she has taken contraceptives, if she has undergone any surgery, etc.
Next, the doctor will request the usual fertility tests, which are typically the following:
- Hormonal tests
- used to check the patient's sex hormones as well as other hormones that play a role in the menstrual cycle.
- Gynecological tests
- to evaluate the anatomy of the uterus and if the ovaries are working properly.
- Hysterosalpingography
- to check tubal patency.
- Chromosome testing (karyotyping)
- to dismiss the possibility for a chromosomal alteration to be present.

If the result of any of these tests is abnormal, the doctor may request further complementary tests, such as an endometrial biopsy or a hysteroscopy, which we will discuss later.
Hormone blood tests
This is one of the first tests performed in order to verify that there are no endocrine problems affecting the menstrual cycle. In addition, hormonal values also provide information about the status of the ovarian reserve and the functionality of the woman's ovaries and pituitary gland.
In short, these are the main hormones evaluated through this blood work:
- Follicle-stimulating hormone (FSH)
- Secreted by the pituitary gland, FSH is responsible for stimulating the ovaries and cause the follicles to grow. The follicles are the structures that contain the eggs.
- Estradiol (E2)
- It is released by the cells that surround the egg as it matures inside the follicle.
- Luteinizing hormone or lutropin (LH)
- It is produced by the pituitary gland as well. Its role is to control the menstrual cycle along with FSH. It increases substantially halfway through the cycle (LH surge) to induce ovulation.
- Progesterone (P4)
- It is secreted by the follicle that remains in the ovary following ovulation in order for the endometrial lining to prepare for embryo implantation after egg fertilization.
- Anti-müllerian hormone (AMH)
- The follicles in the ovaries are responsible for its production. The levels of AMH are proportional to the egg count, and for that reason it is used to measure the ovarian reserve. It is usually measured on day 3-5, although it can be evaluated at any point through the cycle, as its levels do not vary.
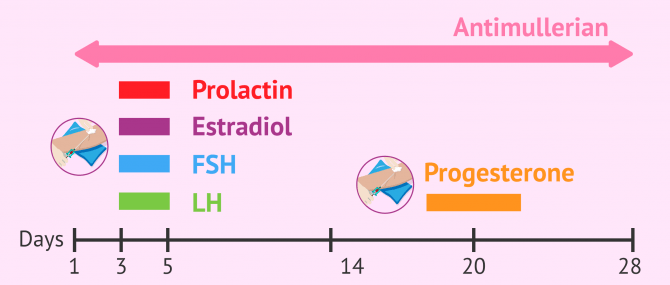
Regarding progesterone, this analysis should be performed around day 20 of the menstrual cycle to determine if ovulation has taken place.
Tests to measure FSH, estradiol, prolactin, and LH should be done between days 3-5 of the cycle, that is, on day three through day 5 of the patient's menstrual period. They are used to measure the values of these hormones on the first days of the cycle.
Blood tests to evaluate hormones such as TSH (thyroid-stimulating hormone), free thyroxine (T4), free triiodothyronine (FT3), prolactin, and total testosterone may also be required. Although these are not sex hormones, if their levels are above or below the average, they can have a negative impact on the hormones that control the menstrual cycle and the ovulation in particular.
Ultrasound
In a female fertility study, a transvaginal ultrasound is performed on the woman to observe the uterus and ovaries with two clear objectives:
- To check whether there exists a malformation in the uterus or any other uterine anatomical abnormality
- To count the number of antral follicles during the first days of the cycle
To this end, the gynecologist uses a catheter, which is covered with a condom, and inserts it through the vagina with a lubricant gel. The catheter sends sound waves that allow the specialist to see on a screen the structure of the uterus and the ovaries when it touches them. Although the pressure exerted by the catheter can cause certain discomfort, it should be clear that this test is totally painless.
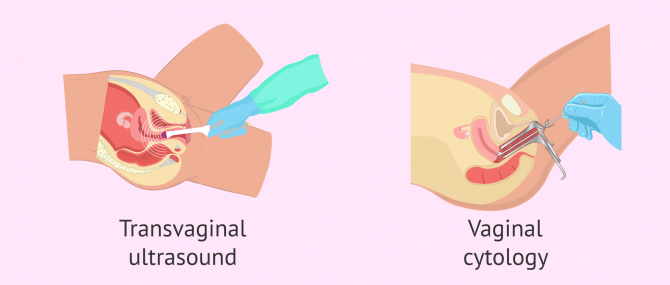
Also, you are likely to undergo a pap smear, pap test, or cytology test. The purpose of this test is to analyze a small amount of cells from the cervix, which are gently scraped with a curette, to look for the presence of infections or cellular alterations that can compromise the woman's fertility. To do this, a small amount of cells is obtained from the cervix through a gentle scraping and sent for analysis.
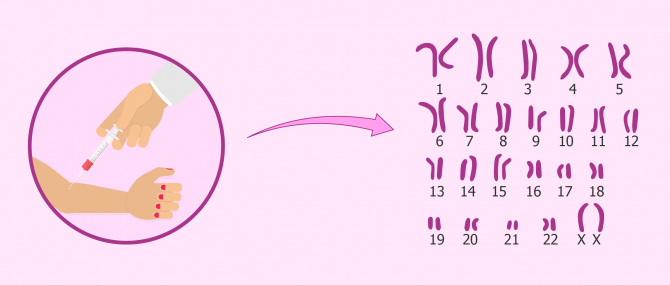
Chromosome testing (karyotyping)
The karyotype is the set of chromosomes contained in each cell. In total, humans have 46 chromosomes, out of which we can find 22 pairs of non-sex chromosomes (autosomal), and 2 sex chromosomes (XX for females, XY for males).
Karyotyping is one of the most important procedures performed in a fertility lab. It is a chromosome analysis used to look for the presence of abnormalities that may be affecting fertility. Such abnormalities can be related to the number of chromosomes (incorrect amount) or to their structure (structural alterations).
Given that all the cells with a nucleus have chromosomes, this test can be done by means of a blood test. The cells to focus on are white blood cells (WBC) or lymphocytes.
The karyotype test is usually performed in both female and male fertility studies, but it is especially important in cases of recurrent miscarriage or implantation failure.
Hysterosalpingography (HSG)
Hysterosalpingography or uterosalpingography is a diagnostic test used to observe the structure of the uterus and the Fallopian tubes, as well as their functionality through X rays (radiography), aided by a fluid that contains a dye.
This is a key diagnostic test when it comes to evaluating a woman's fertility, as lacking tubal patency means that the sperms are unable to go through the tubes, reach the egg, and fertilize it. Also, the existence of an anomaly in the anatomy of the uterus or the tubes can prevent you from getting pregnant.
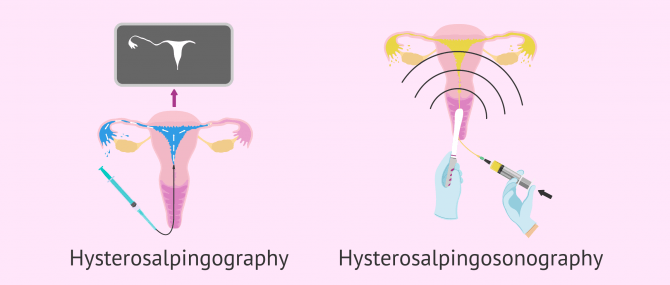
For a HSG to be done, the woman lies in lithotomy position on an examining table, and a catheter is inserted through her cervix. The catheter contains a radiopaque dye that will pass through her cervix, uterus, and tubes. Unless there exists a blockage, the fluid will exit the pelvic cavity easily.
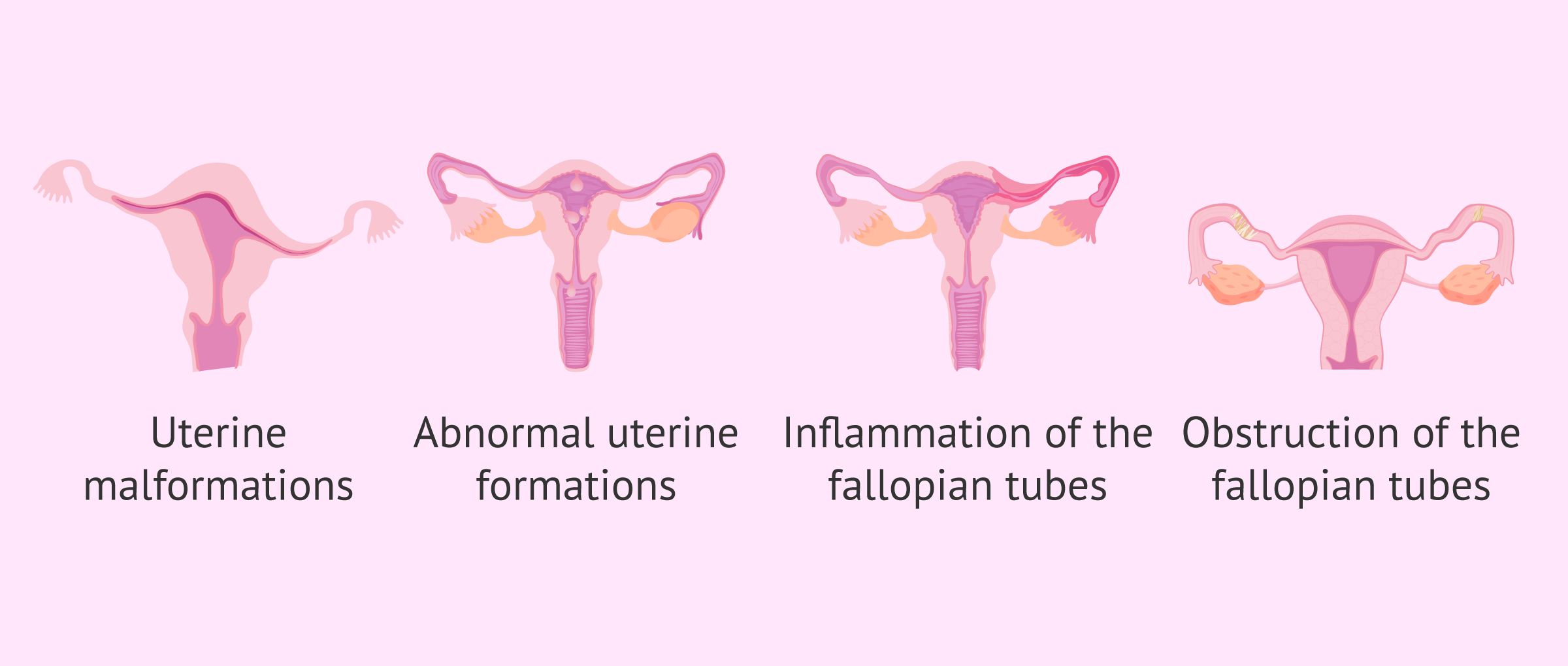
In short, this test allows us to diagnose the following problems:
- Structural abnormalities of the uterine wall
- Abnormal formations in the uterus, including myomas, polyps and adhesions
- Pathologies that cause inflammation of the tubes, e.g. salpingitis
- Pathologies that block the tubes, e.g. hydrosalpinx
Also, a hysterosalpingography can also be used to open the Fallopian tubes thanks to the passage of the radiopaque dye. For this reason, some women are able to achieve pregnancy naturally after undergoing a HSG.
Get detailed information about the definition of hysterosalpingography and the steps involved in this diagnostic test here: How is a hysterosalpingography done?
Other fertility tests
On occasion, a more comprehensive study is necessary to determine or confirm the cause of female infertility.
Below, we will discuss other relevant complementary tests in the female fertility study:
Hysteroscopy
It allows the uterine wall to be observed entirely. This way, the specialist can diagnose potential uterine abnormalities like, polyps, myomas, or lesions of the endometrium that could no be detected accurately by ultrasound or hysterosalpingography.
This gynecological test can be done at the doctor's and involves the insertion of a thin viewing tool called hysteroscope through the vagina and the cervix. By doing this, the doctor is able to observe the patient's uterine cavity.
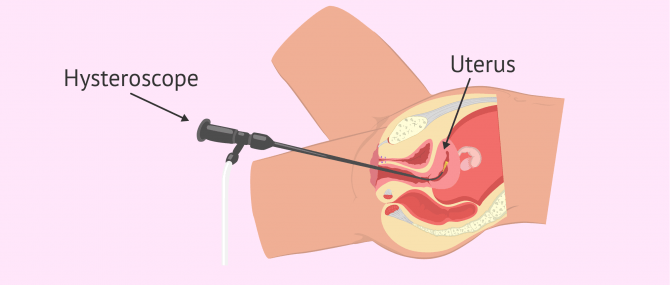
Moreover, it allows the specialist to see the entrance to the Fallopian tubes, but the hysteroscope cannot be inserted through them due to their reduced diameter.
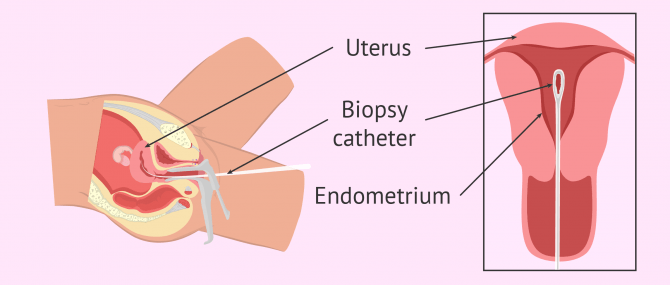
Endometrial biopsy
This diagnostic test involves the removal of a tissue sample from the innermost layer that lines the cavity of the uterus (i.e. endometrium). Then, it is examined under the microscope to look for the existence of an anomaly in its cells.
The specialist inserts a small tube inside the uterus to take a small sample of endometrial lining. This outpatient procedure can be done using local anesthesia or not at the doctor's office.
The tissue obtained in the endometrial biopsy can also be used to perform the ERA test for endometrial receptivity or tests to evaluate the uterine microbiome (EMMA and ALICE tests). These are complementary tests that can be performed for a more comprehensive evaluation of the endometrium, as it is the uterine layer where the embryo must implant. Therefore, these types of tests are usually indicated in cases of implantation failure.
FAQs from users
What are the main female infertility tests?
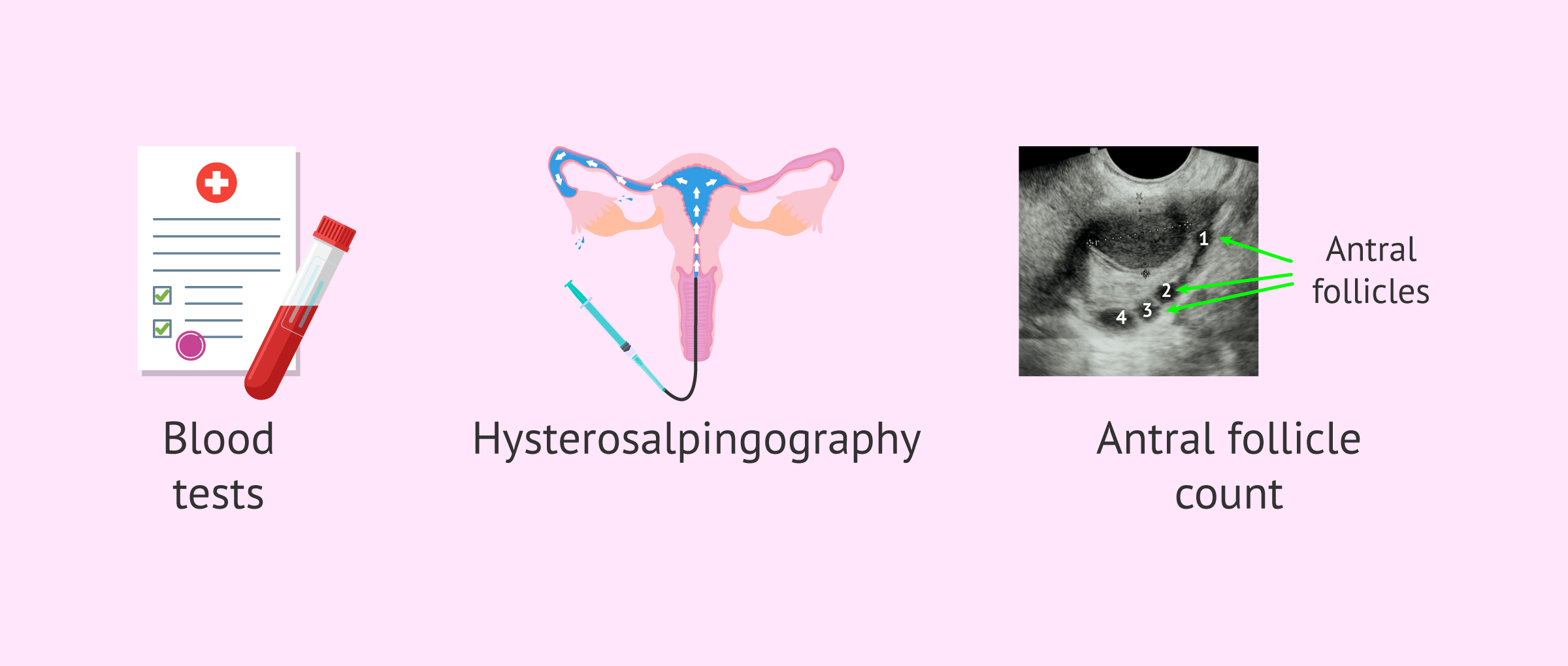
The main tests for studying female fertility are as follows:
- Blood tests where different hormones are analyzed, such as FSH, LH, estradiol, Anti-Müllerian Hormone (AMH), TSH, prolactin, and progesterone.
- Test to evaluate tubal patency known as hysterosalpingography.
- Ultrasound with antral follicle count (AFC).
Although these are the basic tests in the study of female fertility, it is also possible to request complementary tests such as karyotype analysis, a hysteroscopy, or an endometrial biopsy if the specialist considers it appropriate.
How is a Hysterosalpingogram performed?
A HSG is a type of x-ray examination that aims to examine the presence of pathologies in the uterine cavity, and well as tubal patency. It is recommended to evaluate potential causes of primary sterility. It involves inserting a cannula until the entrance of the uterus, through which a special radio-opaque contrast material dye is inserted. The contrast material dye will fill in the cavity and the tubes. Then, a series of x-rays will be done to detect potential abnormalities or blockages in the different structures. It is a simple procedure that is typically done in the first 10 days of the cycle. During its performance, the woman may feel period-like symptoms. Hospitalization is not required, and its duration ranges between 15 and 30 minutes approximately.
How much does a female fertility test cost?
It depends on the tests required and the location where they are performed, but in general the cost of a basic female fertility study can range from $150 to $500 on average.
A hysterosalpingography can cost up to $800-3,000. As for a pelvic ultrasound, a pap smear, and a gynecological exam, the price can be $200 in total, and hormone blood tests can cost up to $50-200 each.
How do you know if you are infertile?
You should visit your doctor to undergo fertility testing. If you and your partner have just started trying to conceive, being checked is unnecessary yet—a basic gynecological exam which includes a pelvic ultrasound to dismiss the possibility of having some kind of uterine abnormality may be enough. Conversely, if you have been trying to conceive for 1 year without success, it is important for both of you to have your fertility checked.
Your gynecologist can answer all the questions you may have regarding female fertility, so our advice is that you do not hesitate to ask.
Is there a DIY female fertility test to check if I am fertile or not?
No, fertility tests for women can only be done in a gynecological clinic. There is only one over-the-counter test that can be done at home to predict the moment of ovulation: an Ovulation Predictor Kit (OPK). It should be clear that this test measures the LH surge that occurs when ovulation is about to happen. Yet, there is no possible way for you to make sure whether ovulation is occurring as it should or not unless you visit a fertility specialist.
What are signs of not being able to get pregnant?
Sometimes, infertility cannot be seen or felt through physical symptoms or signs. However, there are certain conditions that can lead to infertility and can be considered signs of female infertility, including but not limited to, endometriosis (which can cause tubal blockages), ovulation problems, painful periods, deep pain during intercourse, painful bowel motions, chronic pelvic pain, etc.
Nevertheless, the most obvious sign that a woman may be infertile is in fact the inability to get pregnant.
Check this post to learn more: Female infertility: definition, causes, signs and treatment.
Is the study of female fertility the same for all women?
Normally, the tests to assess female fertility are similar for most women. The first step is a gynaecological examination to assess the state of the ovaries and uterus, followed by a hormone analysis.
In this analysis the values of the hormones FSH, LH, oestradiol, AMH, prolactin and progesterone will be determined. It should be noted that the hormone analysis should be done on day 3-5 of the menstrual cycle, except for progesterone, which will be evaluated on day 21.
It is increasingly common to request a karyotype at the first consultation to assess whether there are genetic alterations that may be influencing the desired pregnancy.
Occasionally, it is necessary to perform additional tests such as hysterosalpingography to assess the patency of the fallopian tubes and hysteroscopy. There are also women who should undergo an endometrial biopsy if they have had previous unsuccessful cycles.
Suggested for you
If you want to learn more about fertility in men and women, we recommend that you have a look at the following guide: Male and female fertility.
On the other hand, if you are a woman, do not miss this: Guide to female fertility.
Also, this post gives you a complete overview on the most common fertility tests performed in couples when they visit the fertility specialist after 1 year trying to conceive without success. Want to learn more? Check this out: What fertility tests will I go through?
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Brodin T, Hadziosmanovic N, Berglund L, Olovsson M, Holte J. Antimüllerian Hormone Levels Are Strongly Associated With Live-Birth Rates After Assisted Reproduction. J Clin Endocrinol Metab. March 2013, 98(3):1107–1114 (View)
Carvajal R, Alba J, Cortínez A, Carvajal A, Miranda C, Romero C, Vantman D. Niveles de hormona antimüllerina y factor neurotrófico derivado del cerebro como predictores de función ovárica. Rev Hosp Clín Univ Chile 2012; 23: 159-67 (View)
Guzman L, Ortega-Hrepich C, Polyzos NP, Anckaert E, Verheyen G, Coucke W, Devroey P, Tournaye H, Smitz J, De Vos M. A prediction model to select PCOS patients suitable for IVM treatment based on anti-Müllerian hormone and antral follicle count. Human Reproduction, 2013, 28 (5): 1261–1266 (View)
Pellerito JS, McCarthy SM, Doyle MB, Glickman MG, DeCherney AH. Diagnosis of uterine anomalies: relative accuracy of MR imaging, endovaginal sonography, and hysterosalpingography. Radiology 1992; 183:795-800 (View)
Practice Committee of the American Society for Reproductive Medicine. Electronic address: asrm@asrm.org; Practice Committee of the American Society for Reproductive Medicine. Fertility evaluation of infertile women: a committee opinion. Fertil Steril. 2021 Nov;116(5):1255-1265. doi: 10.1016/j.fertnstert.2021.08.038. Epub 2021 Oct 2. PMID: 34607703. (View)
Ramalho de Carvalho B, Gomes Sobrinho DB, Vieira AD, Resende MP, Barbosa AC, Silva AA, Nakagava HM. Ovarian reserve assessment for infertility investigation. International Scholarly Research Network. ISRN Obstetrics and Gynecology. Volume 2012, Article ID 576385, 10 pages. doi:10.5402/2012/576385 (View)
Romero Guadix B, Martínez Navarro L, Arribas Mir L. Esterilidad: manejo desde la consulta del médico de familia. AMF. 2002; 8 (6): 304-311.
FAQs from users: 'What are the main female infertility tests?', 'How is a Hysterosalpingogram performed?', 'How much does a female fertility test cost?', 'How do you know if you are infertile?', 'Is there a DIY female fertility test to check if I am fertile or not?', 'What are signs of not being able to get pregnant?' and 'Is the study of female fertility the same for all women?'.
Authors and contributors




Hello, what fertility test for woman measures egg count? Is it done at doctor’s? I am interested in knowing this because i’m 35 already and planning to have a baby alone…
Dear muse,
A woman’s ovarian reserve, egg supply or egg count can be evaluated by assessing the levels of AMH (anti-müllerian hormone). This is done along with the analysis of other hormones, such as FSH, LH, progesterone, estradiol, etc. through a blood test. You can find all of them explained above.
Learn more about it here: Ovarian reserve test.
I hope I have been able to help,
Best wishes