The term infertility refers to the failure to achieve pregnancy after one year or more of regular unprotected sexual intercourse , or after more than six months if the woman is over 36 years old. It affects 15% of couples.
Specifically, female infertility is the cause in approximately 33% of the cases. Many different factors and diseases can cause fertility problems in women, such as alterations affecting the ovaries, fallopian tubes, or uterus.
Nevertheless, this doesn't mean that for example, all uterine derformoties or alterations result in problems in the reproductive capacity of the woman.
Provided below is an index with the 10 points we are going to expand on in this article.
- 1.
- 1.1.
- 1.2.
- 2.
- 2.1.
- 2.2.
- 2.3.
- 2.4.
- 2.5.
- 2.6.
- 2.7.
- 3.
- 3.1.
- 3.2.
- 3.3.
- 3.4.
- 3.5.
- 4.
- 4.1.
- 4.2.
- 4.3.
- 5.
- 5.1.
- 5.2.
- 6.
- 6.1.
- 6.2.
- 6.3.
- 6.4.
- 6.5.
- 7.
- 8.
- 9.
- 10.
Hormonal factors
Hormonal factors are one of the causes of infertility in women, as they can cause hormonal imbalances that affect the menstrual cycle.
Hyperprolactinemia
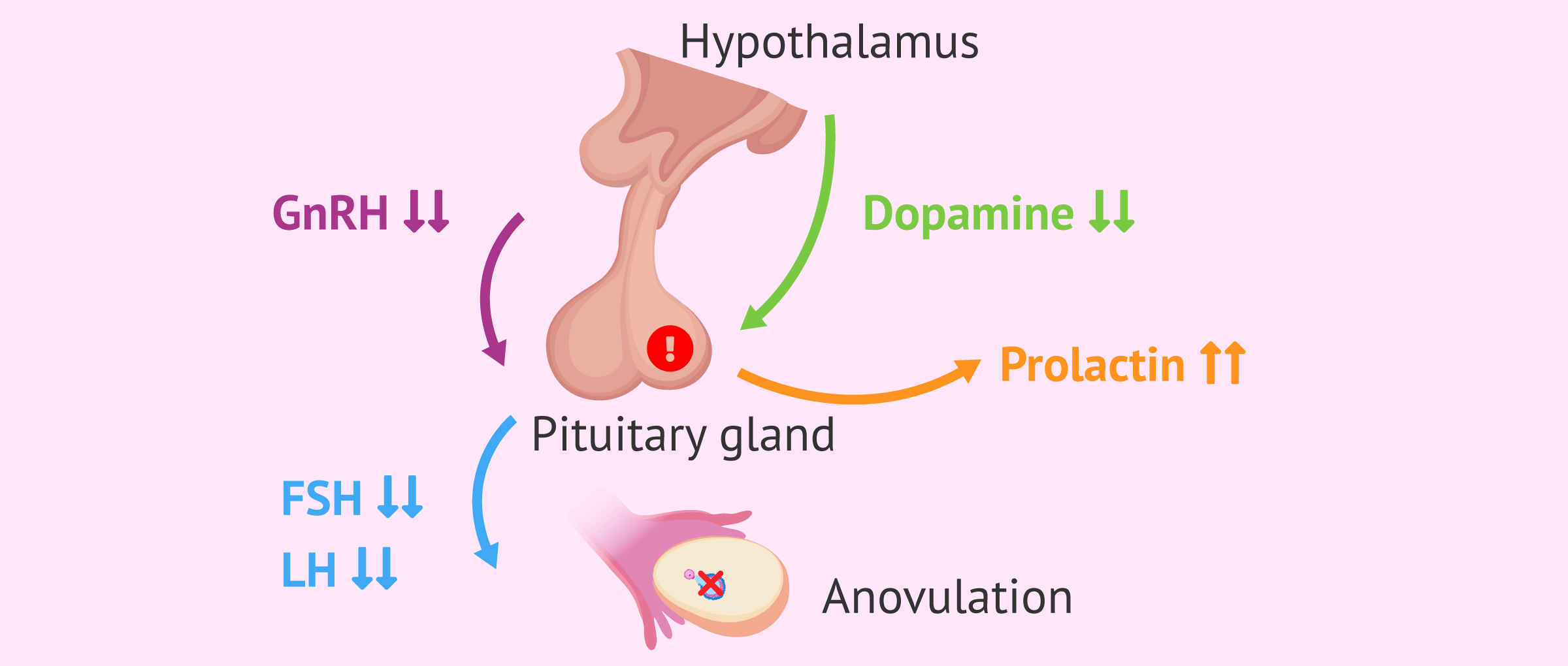
This is a disorder characterized by an increase in the hormone prolactin in the blood, which is produced by the pituitary gland. Prolactin is responsible for the production of breast milk after childbirth and also has an effect on sex hormones.
The pituitary gland is located at the base of the brain and is responsible for the production of growth hormones. It also controls the functions of other glands in the body.
A very common cause of hyperprolactinemia is the appearance of tumors in the pituitary gland, known as prolactinoma.
A change in the levels of prolactin in the bloods can alter ovulation and the menstrual cycle, potentially leading to female infertility.
If you would like more information about hyperprolactinemia, you can visit the link: What is hyperprolactinemia - Causes, symptoms and treatment.
Hypothyroidism
Hypothyroidism is an endocrinological disorder related to a deficit in the production of thyroid hormones. These hormones interact with female sex hormones (estrogens and progesterone) regulating the functioning of the ovaries and the maturation of the eggs inside them.
In general, hypothyroidism can affect female fertility as follows:
- Preventing the production of oocytes.
- Producing irregularities in the menstrual cycle.
- Increasing the levels of prolactin in the blood thereby inhibiting ovulation.

When TSH (Thyroid Stimulating Hormone) values of 5mU/l or higher appear in a blood test, it is indicative of hypothyroidism. TSH values lower than 5 mU/l but higher than 2.5 mU/l are associated with implantation failure and early pregnancy loss.
Ovarian factors
This refers to all disorders that cause alterations in the ovulatory cycle resulting in infertility in women.
Below, we are going to detail the different types.
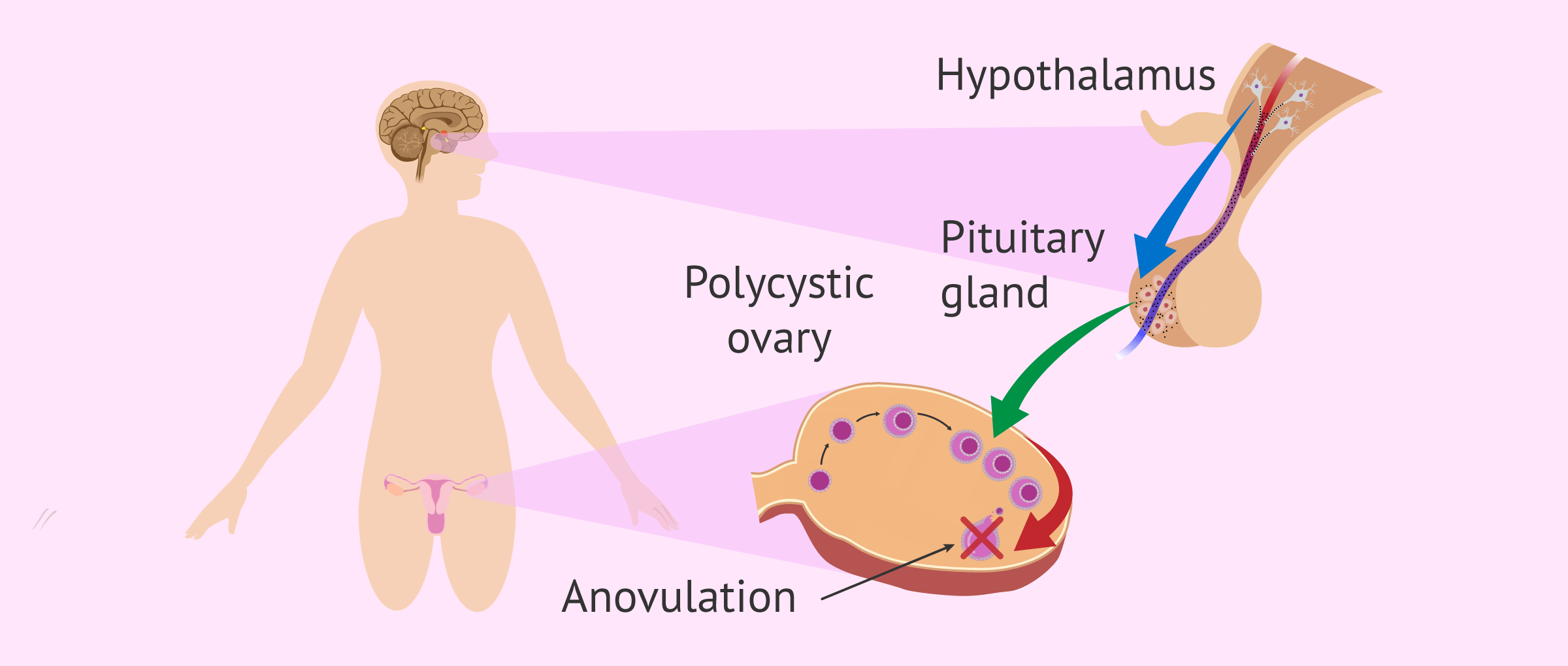
Polycystic ovary syndrome (PCOS)
Polycystic ovary syndrome (PCOS), also called Stein-Leventhal Syndrome, consists of an imbalance of reproductive hormones. The main consequence of this syndrome is problems ovualtion problems.
In 2026, polycystic ovary syndrome was renamed polyendocrine metabolic ovarian syndrome. This name change was made because not all women with this condition had ovaries that appeared polycystic. Therefore, the former name, PCOS, was inaccurate, and the focus has now shifted to hormonal and endocrine abnormalities rather than the appearance of the ovaries.
Women with PCOS produce more androgens than normal and the regulation of the menstrual cycle is not correct. In the ovary, the follicles do not release the eggs due to the lack of their maturation and cysts are produced.
For more detailed information on this syndrome, we encourage you to read on here: Polycystic ovary syndrome (PCOS): causes, symptoms, and treatment.
Premature ovarian failure
Premature ovarian failure (POF), also known as primary ovarian insufficiency (POI), is the loss of function of the ovary before the onset of menopause.
It usually appears in women under the age of 40 and perimenopausal symptoms or amenorrhea (absence of one or more menstrual periods) begin.
When the function of the ovaries fails, the necessary amounts of estrogen are not produced and eggs won’t be released. This alteration will result in female infertility.
The most prominent general symptoms of premature ovarian insufficiency are:
- Absent or alternating menstrual periods, i.e., amenorrhea.
- Difficulty in carrying out a pregnancy.
- Night sweats.
- Vaginal dryness
- Decreased libido.

If you would like to read more about this subject then you can read the following article: Premature Ovarian Failure - Causes & Symtpoms
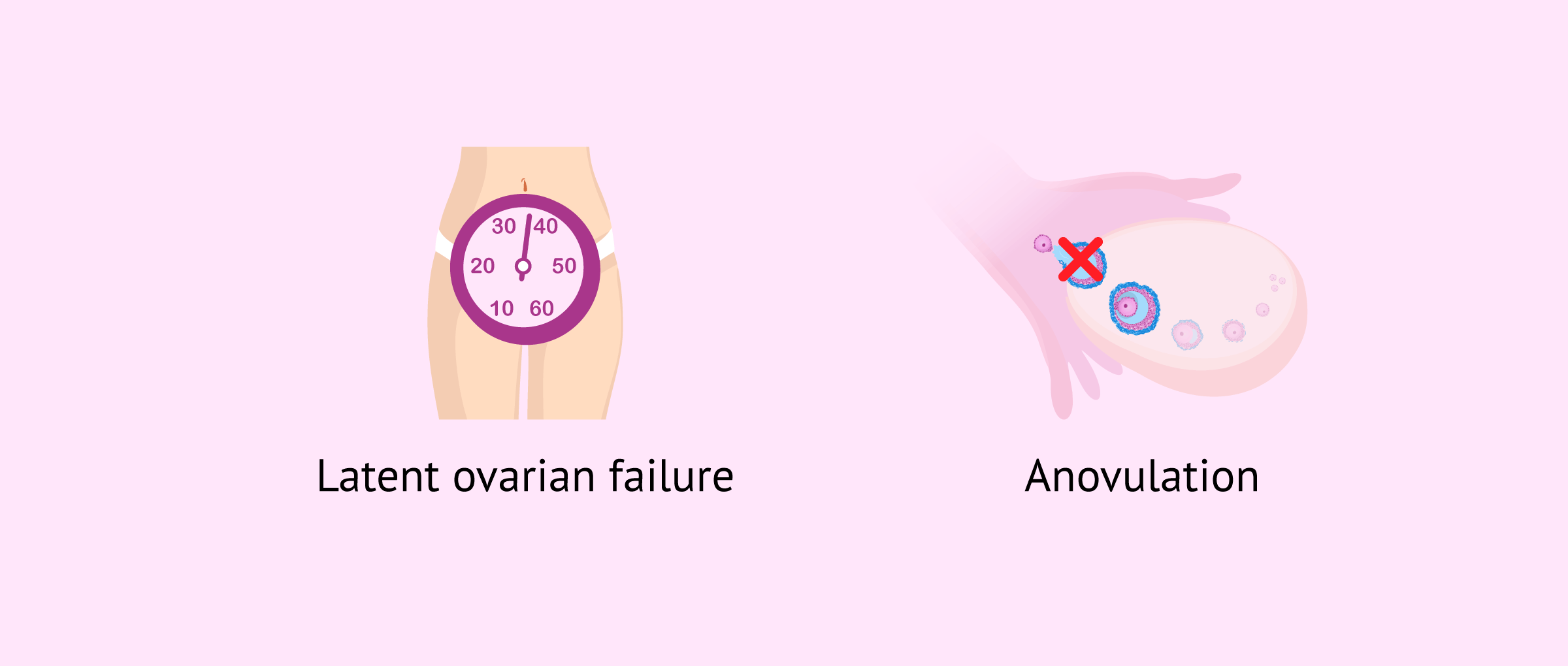
Occult premature ovarian failure
Occult ovarian insufficiency is due to ovarian dysfunction and is characterized by regular menstrual cycles and elevated FSH hormone levels. The main cause is the accelerated aging of the ovary.
Unlike POI, in occult ovarian insufficiency there are no symptoms of menopause.
The only way to diagnose this disorder is through a blood test of female sex hormones.
Anovulation
Anovulation is defined as a lack of release mature eggs from the ovaries in the woman, so there will be no encounter of the egg and sperm in the fallopian tubes for fertilization to take place.
Considering seeing a fertility specialist? Don't forget that, in the field of Reproductive Medicine, as in any other medical area, it is crucial that patients rely on the doctors and staff that will help them through their treatment cycle. Logically, conditions vary from clinic to clinic. For this reason, we recommend that you generate your Fertility Report now. It will offer you a list of clinics that have passed our rigorous selection process successfully. Furthermore, the system will make a comparison between the fees and conditions of each clinic so that you can make a better-informed decision.
There are two types of anovulation:
- Circumstantial anovulation
- also known as sporadic anovulation. It results from periods of stress, after the first menstruation. In principle, there is no need to worry in these cases as menstrual cycles are usually restored.
- Chronic anovulation
- where women have long periods of time without ovulation, so it is not possible to for the egg to unite with the sperm.
Currently, there are treatments to correct this alteration and return fertility to the woman.
Diminished ovarian reserve
Ovarian reserve refers to the quantity and quality of oocytes available to a woman at any given time. There is an inverse relationship between age and ovarian reserve; that is, the older the woman, the lower the reserve and the quality of her eggs.

If the ovarian reserve is good, the chances of achieving a pregnancy are high. On the other hand, if the woman has a low ovarian reserve it will cause a fertility problem.
For this reason, the evaluation of the ovarian reserve by a specialist is essential to determine the reproductive prognosis of the couple. It is carried out by means of a blood test where the Antimüllerian Hormone (AMH) is determined.
If you would like more information, we recommend continuing your reading with this article: What is ovarian reserve and how does it affect fertility?
Luteal dysfunction
The luteal phase is one of the phases of the female menstrual cycle that occurs between the day of ovulation, caused by an LH peak, and the last day before menstruation.
Luteal phase disfunction, also known by the names luteal phase deficiency (LPD) or corpus luteum insufficiency, can be exclusively an ovarian dysfunction or caused by endocrine diseases such as thyroid disorders or hyperprolactinemia.
The symptoms of this alteration are:
- Bleeding after ovulation
- Low blood levels of progesterone.
- Sensitive breasts.
- Miscarriages.

Female infertility results because the implantation of the embryo in the woman's uterus occurs between 6-10 days after ovulation. If there is a deficiency of the luteal phase, the endometrium does not prepare properly with the correct thickness. The final consequence will be a delay in or failure of embryo implantation.
Turner syndrome
Turner syndrome is also known as Ullrich-Turner Syndrome or Monosomy X. It is a chromosomal alteration characterized by the partial or total absence of the X chromosome.
60% of affected people have a 45,X0 karyotype with the absence of an entire X chromosome. The remaining 40% are due to other genetic alterations in the chromosomes.

Women with this disorder present with short stature, absence of menstruation, and a lack of secondary sexual characteristics. In addition, in 98% of cases, these women have early ovarian failure and absence of eggs, causing infertility problems.
For more in depth information about this topic, we recommend visiting the following post: Turner Syndrome: Causes, Characteristics, and Pregnancy
Tubal factors
Tubal factors are responsible for problems in female fertility because the Fallopian tubes are essential to the reproduction process.
Therefore, any injury or obstruction in the Fallopian tubes will prevent them from performing their functions correctly causing female sterility.
Endometriosis
Endometriosis is a chronic gynecological disease that consists of the appearance and growth of endometrial tissue outside the uterus, especially in the pelvic cavity such as the ovaries, behind the uterus, in the uterine ligaments, in the bladder or in the intestine. This tissue growth may alter the function of the ovary or block the Fallopian tubes.
Endometriosis may lead to infertility in women. Specifically, about 40% of women with endometriosis have difficulties in getting pregnant.

Some symptoms of this disorder are:
- Metrorrhagia
- premenstrual bleeding or bleeding between periods.
- Dyspaurenia
- pain during or after sex.
- Hematuria
- pain and bleeding when urinating.
- Pelvic, abdominal, and lower back pain
- associated with menstruation.

If you would like to learn more about the effect of endometriosis on a woman's fertility, read on here: How does endometriosis affect a woman's fertility?
Pelvic inflammatory disease (PID)
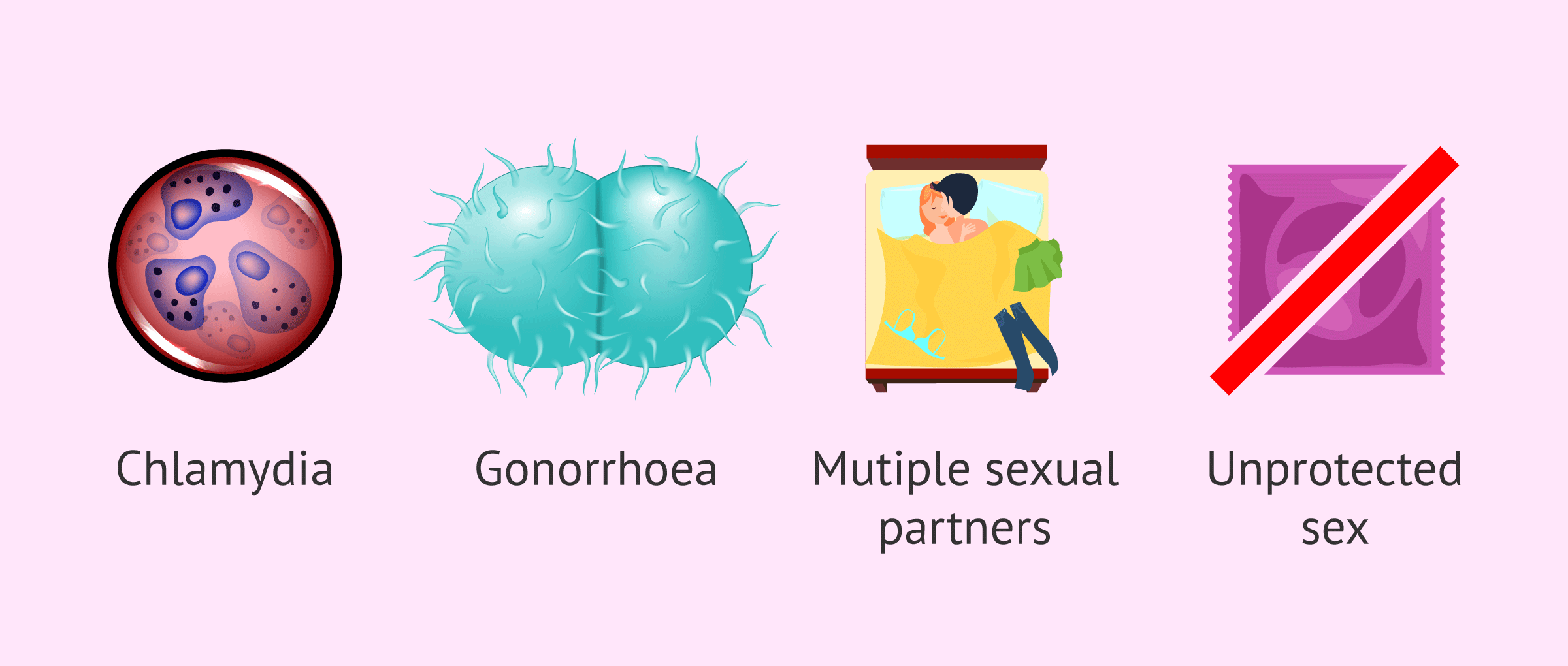
This disease is an inflammatory process caused by an infection in the uterus, ovaries, and other female reproductive organs. It causes scarring in these organs, leading to infertility, ectopic pregnancy and pelvic pain, amongst others.
In most cases, this disease is caused by the bacteria Chlamydia trachomatis and Neisseria gonorrhoeae.
Some of the risk factors are:
- Changing sexual partners.
- Vaginal douching.
- Not using birth control.
- Having a history of PID or sexually transmitted diseases.
In the following link you can read more about this tubal alteration: Pelvic inflammatory disease (PID).
Pelvic adhesions
These are bands of scar tissue that form between the organs of the pelvis (ovaries, fallopian tubes, uterus, bladder, and intestines) that can cause them to attach to each other and lose their function.
Pelvic surgeries and the resulting scars can also cause adhesions, affecting the functionality of the Fallopian tubes.

These adhesions can cause the Fallopian tubes and ovaries to stick to other nearby surfaces. As a result, their functions are impaired and fertility issues develop.
In the event that an egg is fertilized with a sperm, pelvic adhesions can also prevent the fertilized egg from reaching the uterus. This occurence increases the possibility of ectopic pregnancy, that is, that the embryo implants outside the uterus.
Salpingitis
Salpingitis is an isolated inflammation due to an infection of the Fallopian tubes.
The agents causing the infection are usually Chlamydia trachomatis, gonococcus or Mycoplasma hominis in 60% of cases, while the remaining 40% are due to bacteria that can be found in the vaginal flora.
The Vaginal flora are microorganisms that live naturallywithin the vagina without causing any damage.
This disorder may be acute and symptomatic, or chronic where it may go unnoticed.
Hydrosalpinx
Hydrosalpinx is a disorder resulting from an obstruction in the ends of the Fallopian tubes. This causes an accumulation of fluid inside them.
The problem with this disease is that the sperm cannot ascend and the egg will not be captured by the Fallopian tube, so fertilization does not take place. This makes the possibility of a natural pregnancy difficult.

Uterine factors
The uterus is an essential organ for reproduction. Thus, the uterine factor must be taken into account in female infertility, since any alteration of the uterus will have a consequence in the process of reproduction.
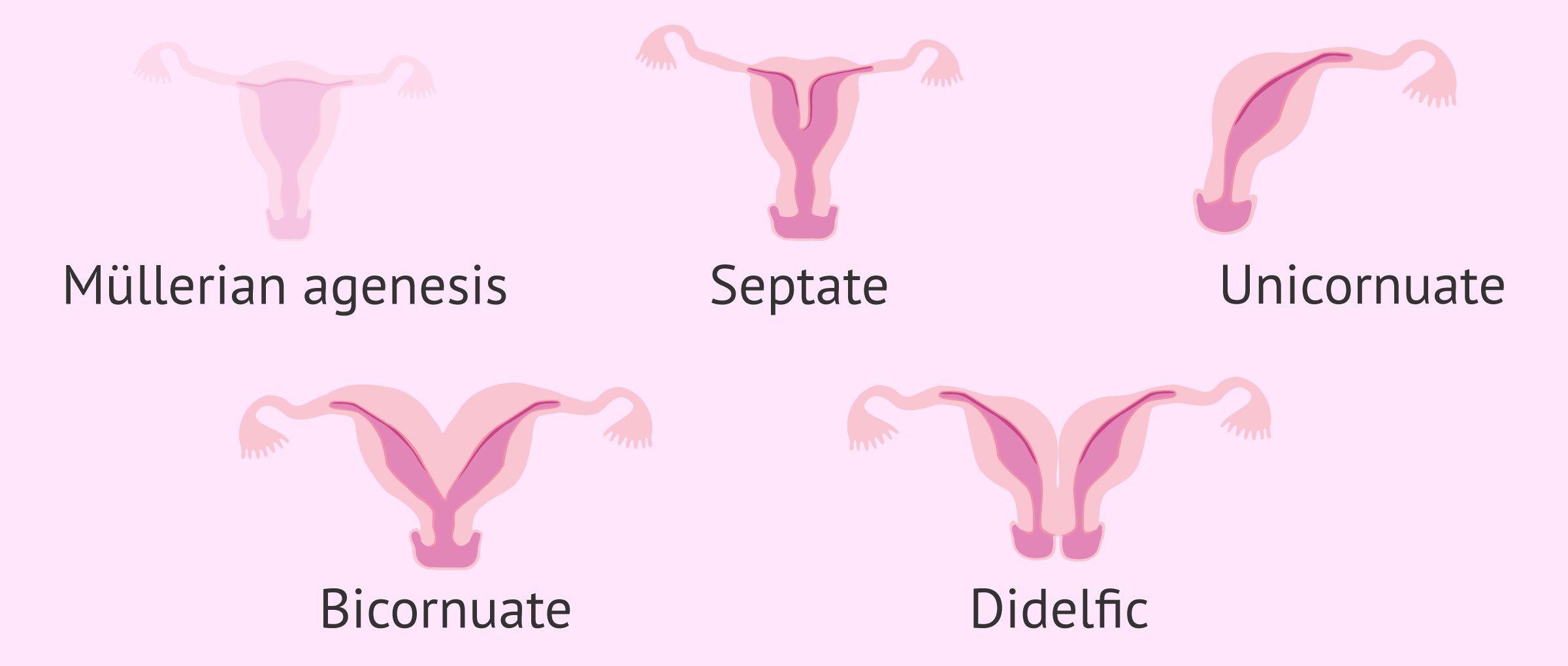
Uterine malformations
Uterine malformations are important for a woman's life because they are the origin of menstrual alterations, sterility and infertility due to abortion, miscarraige, premature birth, etc.
There are several uterine anomalies but not all of them cause infertility in women. Those that do prevent the implantation of the embryo and its growth in the uterus.
The malformations that affect fertility are the following:
- Müllerian Agenesis
- complete absence of uterus.
- Unicornuate uterus
- smaller uterus with a single Müller duct.
- Uterus didelphys
- is known as a double uterus because it has two independent uterine cavities.
- Bicornuate uterus
- as a result of an incorrect fusion of the Mullerian ducts.
- Septate uterus
- as a result of a fault in the reabsorption of the septum that divides the Mullerian ducts
Mullerian ducts are embryonic structures that appear in both sexes. In women, they give rise to the fallopian tubes and the uterus-vaginal canal; while in men, they give rise to the testicular appendix and a small cleft located in the urethra called the prostatic utricle.
If you want to know more about uterine malformations, you can read on Uterine malformations in women: may they cause infertility?
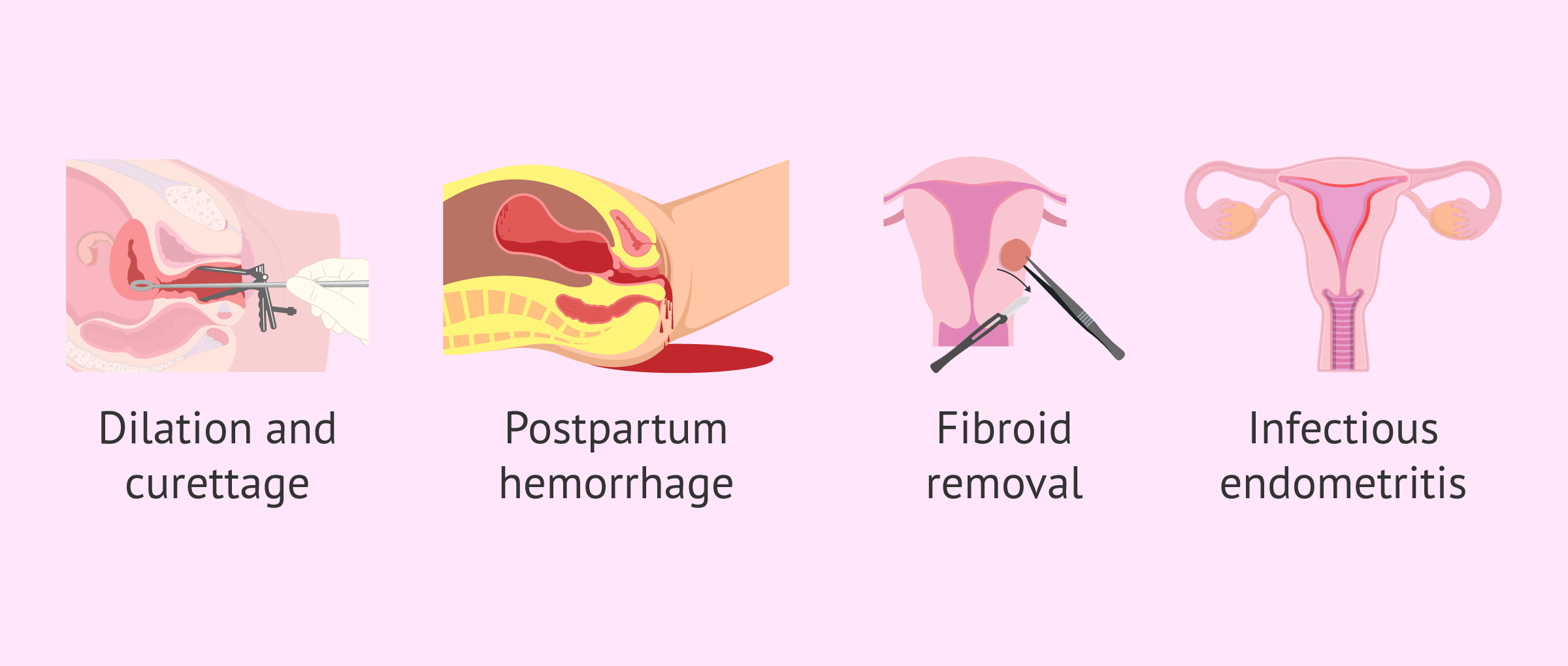
Uterine synechiae
Uterine synechiae are adhesions that occur on the uterine walls. They are also called Asherman's Syndrome or intrauterine adhesions. The prevention and treatment of this pathology is essential for fertility.
The most severe form of synechia is amenorrhea or hypomenorrhea.
Among the most frequent causes is found:
- Uterine scraping or curettage.
- Bleeding after childbirth, either by cesarean section or natural childbirth.
- Removal of a fibroid.
- Infectious endometritis.
You can read more about Asherman´s Syndrome in this article: Asherman´s Syndrome, signs, treatment and chances of pregnancy.
Tumors
Various tumors can be found in the uterus, most of which are usually benign. Among the most important are:
- Uterine fibroids
- masses of muscle tissue that are generated around the uterus. Occasionally they may appear on the cervix. Specifically, they occur in the smooth muscle tissue cells of the myometrium (the muscular layer of the uterus).
- Adenomyosis
- endometrial tissue, which lines the uterus, develops in the muscular wall of the uterus. This pathology causes a thickening of the uterus.
- Uterine polyps
- endometrial tissue that comes out of the uterine cavity. These polyps are quite sensitive to estrogen.

Other factors
In addition to all the factors mentioned, there are also others that can cause diseases resulting in female infertility. They are detailed below:
Anti-sperm antibodies
Antisperm antibodies (ASA) are the main cause of fertility problems related to immune sterility.
These antibodies can be found in the sperm itself, in seminal plasma, or even in cervical mucus.
An antibody (also called immunoglobulin) is a substance that is produced in the body and is intended to defend against foreign substances.
ASAs bind to sperm and affect their mobility. This prevents sperm from interacting with the egg, causing infertility.
Vaginismus
Vaginismus is a medical term for vaginal tightness, an involuntary contraction of the perivaginal muscles. It is a barrier to sexual intercourse because it prevents penetration or makes it very painful.
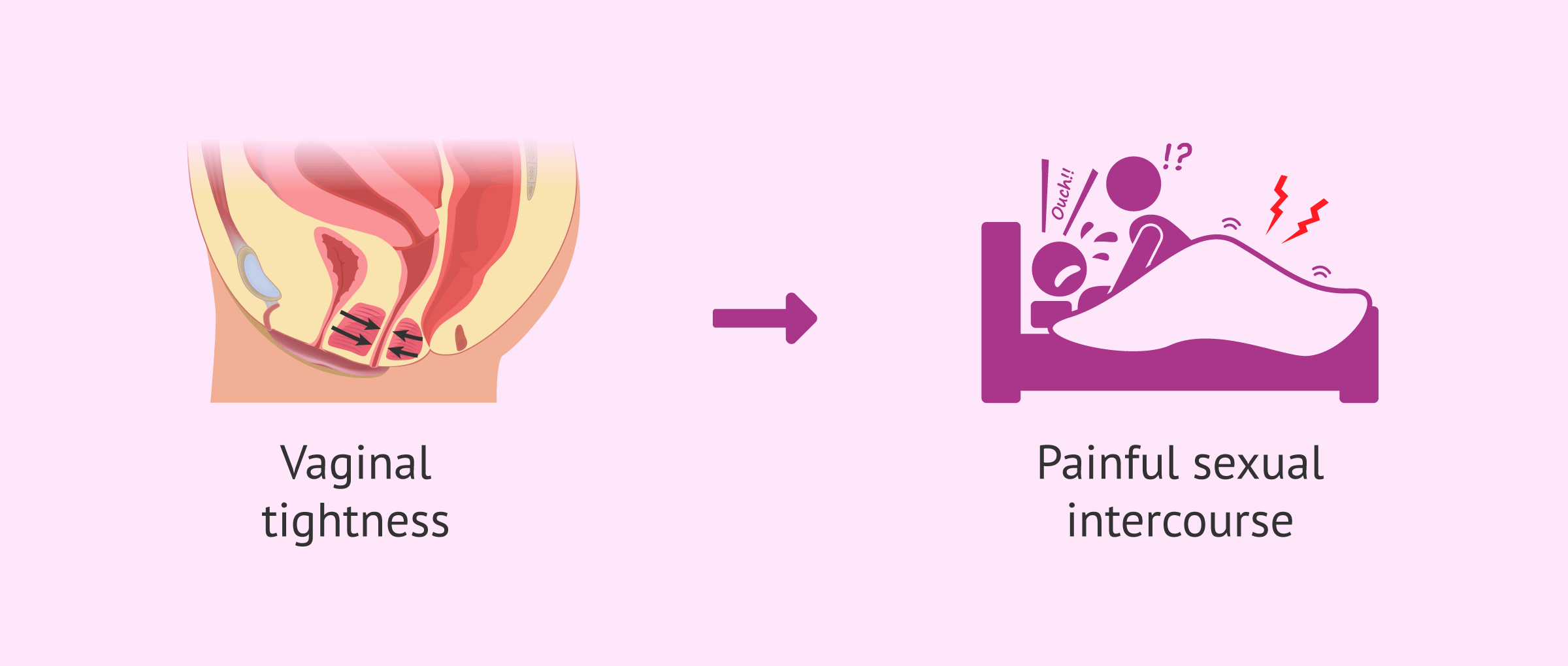
Psychological and gynecological treatment would be a solution to improve sexual life and try to achieve a natural pregnancy. Artificial insemination may also be used. However, there is no surgical or pharmacological treatment.
FAQs from users
Can chronic diseases cause female infertility?
There are multiple diseases that have repercussions in the reproductive field. Thus, chronic diseases are an important factor to take into account for couples planning pregnancy.
Among chronic diseases, the most prevalent is diabetes. As we know, it is a common disease that generates problems in carbohydrate metabolism and requires strict control. In cases of well-controlled diabetes, it does not necessarily affect fertility, unless the woman presents other complications, such as polycystic ovary disease, which affects 8-12% of women with type I diabetes. Between 20% and 40% of women with type I diabetes have menstrual irregularities.
With regard to gestation and assisted reproduction treatment, a multidisciplinary approach is essential, where endocrinologist and gynecologist are in constant communication and plan the best time for gestation, especially based on the control of blood glucose levels. It is clearly advisable to avoid transferring more than one embryo.
What is the difference between premature ovarian failure and occult ovarian insufficiency?
Ovarian insufficiency or ovarian failure is the condition suffered by young women, under 42 years, with malfunction of the ovary due to low ovarian reserve.
All women lose proper ovarian function at some point in their lives, since the ovary is endowed with follicles (which inside have eggs) that are going to decrease throughout our lives, and are not going to regenerate again.
If exhaustion comes at 48 years, it is not a problem, and menopause occurs naturally.
However, in other women, there may be ovarian depletion at a young age. If it is accompanied by alterations in the pattern of the menstruational cycles, an early ovarian failure will occur. If, on the other hand, there are no alterations in the menstrual pattern, it will be called occult ovarian failure.
Do all uterine diseases cause infertility in women?
No. The uterine diseases that cause infertility are mullerian agenesis, unicornuate uterus, bicornuate uterus, uterus didelphys or septate uterus.
What are the differences in prolactin values in case of hyperprolactemia?
The normal rate of prolactin in women is around 20 µg/l and in cases of hyperprolactinemia the rate exceeds 30 µg/l. This increase causes an inhibition of the function of GnRh, also known as Gonadotropin-releasing hormone , thus blocking the production of LH and FSH.
Does the thyroid influence a woman's reproduction ability?
Yes, of course. Thyroid function and TSH are very important for the early stages of pregnancy.
When TSH levels are lower than 5 mU/l but higher than 2.5 mU /l, it is usually associated with embryo implantation failure.
Recommended reading
We have talked about hypothyroidism as a disease that causes infertility in women. If you want more information we recommend that you access the article Hypothyroidism and pregnancy.
If you want to know more about hydrosalpinx, you can access the following link: What is hydrosalpinx - Causes, symptoms and treatment.
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Achour R, Koch M, Zgueb Y, Ouali U, Ben Hmid R. Vaginismus and pregnancy: epidemiological profile and management difficulties. Psychol Res Behav Manag. 2019 Mar 12;12:137-143. doi: 10.2147/PRBM.S186950. 2019. (View)
Brosens C, Terrasa S y Astolfi E. Vaginismo. Evid Act Pract Ambul. 2009; 12(3): 102-103 (View)
Bulun SE, Yilmaz BD, Sison C, Miyazaki K, Bernardi L, Liu S, Kohlmeier A, Yin P, Milad M, Wei J. Endometriosis. Endocr Rev. 2019 Apr 17. pii: er.2018-00242. doi: 10.1210/er.2018-00242
Dreisler E, Kjer JJ. Asherman's syndrome: current perspectives on diagnosis and management. Int J Womens Health. 2019 Mar 20;11:191-198. doi: 10.2147/IJWH.S165474 (View)
Gómez, AE. Infertilidad femenina. Actualización. Elsevier. 2011 Septiembre; 30(5):7-78
Harb HM, Ghosh J, Al-Rshoud F, Karunakaran B, Gallos ID, Coomarasamy A. Hydrosalpinx and pregnancy loss: a systematic review and meta-analysis.Reprod Biomed Online. 2019 Mar;38(3):427-441. doi: 10.1016/j.rbmo.2018.12.020. Epub 2018 Dec 25 (View)
Kovanci E, Schutt AK. Premature ovarian failure: clinical presentation and treatment. Obstet Gynecol Clin North Am. 2015;42:153-61 (View)
Laven JS. Primary Ovarian Insufficiency. Semin Reprod Med. 2016 Jul;34(4):230-4 (View)
López, V, Flores, E, Romeu, A. Estudio de la insuficiencia ovárica primaria (IOP) e insuficiencia ovárica oculta (View)
FAQs from users: 'Can chronic diseases cause female infertility?', 'What is the difference between premature ovarian failure and occult ovarian insufficiency?', 'Do all uterine diseases cause infertility in women?', 'What are the differences in prolactin values in case of hyperprolactemia?' and 'Does the thyroid influence a woman's reproduction ability?'.
Authors and contributors




More information about Michelle Lorraine Embleton

Hi
I had PID when I was younger and I was told, and have read so may times on social media, that it can cause infertlity. I took antibiotics and was given the all clear, but now I am older and we are thinking about starting a family. I am terrified that I may have fertility problems and not be able to get pregnant. How can I know?
Hi Rachel
It is normal that you are worried about how the PID you had when younger affected your fertility, and obviously you won’t know until you start trying for a baby. If you are ready to start trying to conceive (ttc) then you should go ahead and start having regular unprotected sex with your partner.
If after a year of TTC to conceive (or 6 months if you are over 35) and you haven been unable to get pregnant then it is time to consult an infertility specialist. In your case you should tell them of your PID in your medical history so they can look into the possiblity of adhesions from the infection.
You can read more information on PID in our article: What is pelvic inflammatory disease?
I hope this answer is useful and good luck with the ttc!