Turner syndrome is a chromosomal alteration characterized by a complete or partial loss of one of the sex chromosomes in the female sex. As a result, the karyotype of those women is 45,XO instead of the usual karyotype 46,XX.
The symptoms of this disease vary significantly, although the majority of the women present a short stature and an alteration of the development of the sexual characteristics.
Turner syndrome is also a cause of endocrine infertility due to the ovarian failure of these women and the risk of transmitting the chromosome in their offspring.
Provided below is an index with the 10 points we are going to expand on in this article.
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 6.1.
- 6.2.
- 6.3.
- 6.4.
- 6.5.
- 7.
- 8.
- 9.
- 10.
Definition
Turner syndrome, also known as the Ullrich-Turner-Syndrome, is a genetic disorder which affects the development of the female children due to the missing X chromosome. This syndrome affects 1 in 2500 women worldwide.

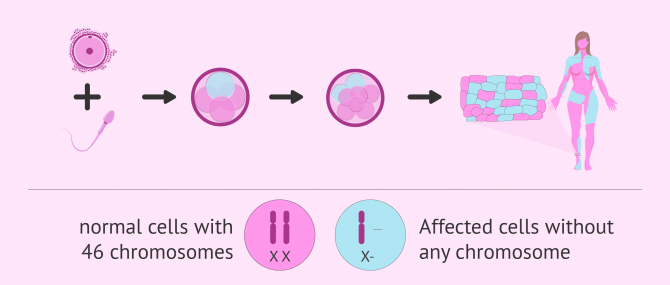
There are various degrees of severity because in some occasions, the X chromosome is not completely absent or the alteration present itself as mosaicism, which means that some of the cells of the organism are normal and others have a chromosomal alteration (46,XX/45,XO).
In these cases the affected female children may show some signs of puberty and between 2 and 5% can even be fertile.
Turner syndrome consists of the monosomy of the X chromosome, which means that only one of the sexual chromosomes is working due to the absence or incompletion of the other chromosome.
In the more favorable cases of the Turner syndrome, the symptoms are not very prominent and are not easily identified. There are women who are not diagnosed until they have their karyotype analysis done for having repeated abortions, babies with abnormalities or after a genetic study of stillborn babies.
Characteristics in women
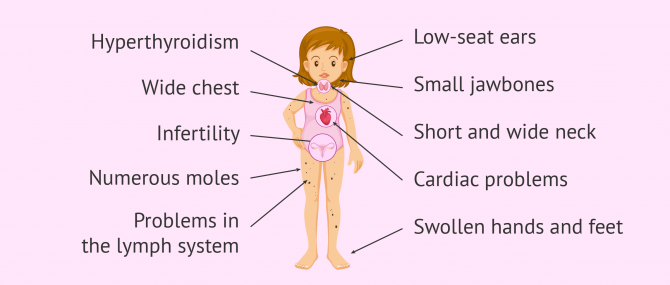
Women with Turner syndrome present a delayed or inexistent sexual development, which hinders the appearance of the secondary sexual characteristics during puberty.
Additionally, there are other common manifestations of this syndrome which we will indicate below:
- Short stature
- Short and webbed neck: wrinkled neck skin
- Low-set ear and hair
- Wide and flat chest
- Drooping eyelids and dry eyes
- Rotary arms at the elbow
- No menstruation
- Painful sexual relations due to vaginal dryness
- Swollen hands and feet in the baby stage
- Multitude of moles all over the body
- Infertility
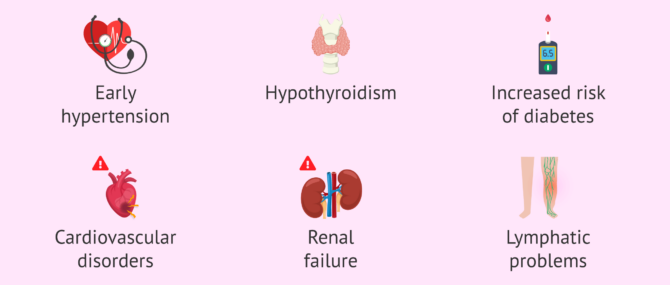
Apart from those symptoms, there can be other systemic alterations and deformations in other organs of the body:
- Early hypertension
- Hypothyroidism
- Increased risk of diabetes
- Cardiovascular alterations
- Renal insufficiency
- Problems in the lymphatic system
Finally, girls with Turner syndrome may also have psychological problems and delayed emotional maturity.
What are the causes of Turner syndrome?
The main cause of Turner syndrome is the complete or, as explained above, partial absence of an X sex chromosome. The exact mechanism that leads to this genetic alteration in embryos is unknown, but two possible theories are currently being considered:
- Meiosis
- the cause would be an alteration in the gametogenesis (formation of eggs and sperm) of the parents. This would result in gametes that do not carry the X chromosome and that, when fertilized, would result in embryos with karyotype 45,XO.
- Mitosis
- the loss of the X chromosome would not take place int he gametes but would get lost due to a failure in the first embryonary divisions after the fertilisation.
The second theory explains better the cases of Turner syndrome in mosaicism, since the divisions with the unbalanced number of chromosomes would be what leads to the presence of healthy cells and cells with monosomy in the individual.
The karyotype of the women with Mosaic Turner syndrome is 46,XX/45,XO.
The majority of researches support this second theory, the mitotic one, although they do not completely dismiss the first one.
Is there a treatment for Turner syndrome?
Because it is a chromosomal disease, there is no definitive cure for Turner syndrome.
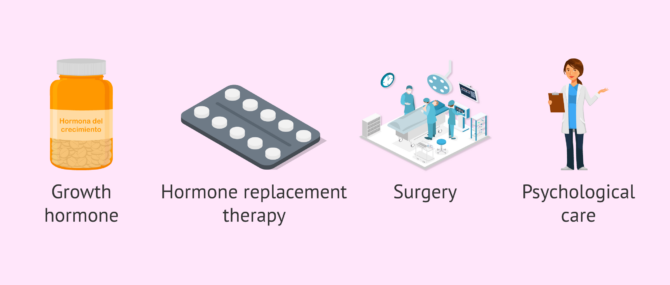
However, there are pharmacological and surgical treatments to try to correct some of the associated disorders help the woman lead as normal a life as possible. These are discussed below:
- Growth hormone
- to be able to increase the speed of growth during childhood and reach a higher height in adulthood.
- Hormone replacement therapy
- to promote sexual development and the appearance of secondary sexual characteristics: breast growth, pubic hair, etc. In addition, estrogens will help maintain the body's bone health.
- Surgery
- in case of visual, cardiac or other alterations that can be corrected.
- Psychological care
- if there are behavioural disorders in girls, difficulties in coping with the diagnosis or even when infertility is discovered in adulthood.
It is advisable for girls with Turner syndrome to visit several pediatric specialists in order to detect each of the possible disorders early and apply the most appropriate treatment: ophthalmologists, nephrologists, cardiologists, endocrinologists, and so on.
Turner syndrome and pregnancy
96% of women with Turner syndrome have fertility problems due to lack of sexual development and ovarian failure.
In addition, if a pregnancy is attained, the rate of spontaneous abortion is very high in these patients, as well as the risk of having children with malformations.
Women with Turner syndrome who become naturally pregnant are more likely to have children with Down syndrome, Turner syndrome, or other genetic alterations.

Therefore, the best option for women with Turner syndrome is to use assisted reproduction in order to become mothers. More specifically, the indicated techniques are as follows:
- IVF with PGD
- with the preimplantation genetic diagnosis it is possible to select healthy embryos, without any genetic alteration, so that a viable pregnancy can take place without the risk of fetal malformations. This treatment is indicated for patients with the Mosaic Turner syndrome who have some ovarian function.
- Ovodonation
- is the most suitable treatment and provides a higher success rate for these patients, especially for those who are not able to use their own eggs.
In general, women with Turner syndrome can carry a pregnancy to term without problems. The rate of evolutionary pregnancy is high and similar to that of other patients with assisted reproduction techniques.
Assisted procreation, as any other medical treatment, requires that you rely on the professionalism of the doctors and staff of the clinic you choose. Obviously, each clinic is different. Get now your Fertility Report, which will select several clinics for you out of the pool of clinics that meet our strict quality criteria. Moreover, it will offer you a comparison between the fees and conditions each clinic offers in order for you to make a well informed choice.
FAQs from users
Is Turner syndrome hereditary?
Turner syndrome is a chromosomal disorder characterized by the total or partial loss of one of the sex chromosomes in the female gender. Therefore, the karyotype of these women will be 45.X0 instead of the normal karyotype which is 46.XX. It is not known whether the cause may be due to meiotic problems (formation of the oocytes in the mother) or mitotic problems (division of the cells in the embryo).
This is why women with Turner syndrome are more likely to have children with Turner syndrome or other genetic disorders, because the segregation of their chromosomes occurs in an unbalanced way.
Can women with Turner syndrome get pregnant naturally?
Turner syndrome is one of the most common chromosomal abnormalities in humans, and represents an important cause of early menopause. It is caused by the total or partial loss of one of the X chromosomes (women usually have 2 X chromosomes).
The vast majority of women with Turner syndrome will be sterile due to ovarian failure. However, there is a small percentage of women (about 5%) who will be able to achieve natural gestations. It will be more likely if you have had spontaneous menstruations or if you have a mosaic Turner syndrome (when some cells have one X chromosome and two other X chromosomes).
Some adolescent women or Turner mosaics will have enough ovarian function to respond to ovarian stimulation and may vitrify oocytes to become mothers later or perform in vitro fertilization. However, the vast majority of women with this chromosomal alteration will have to resort to ovodonation.
In addition, for these women there is an increased risk of aortic dissection during pregnancy and postpartum, which will require a complete medical evaluation before seeking gestation, paying special attention to cardiovascular and renal function.
Can an advanced age cause the Turner syndrome?
Although the exact cause of Turner syndrome is unknown, advanced maternal age does pose a risk factor. As women get older, the risk of accumulating genetic alterations in their eggs and giving rise to embryos with chromosomal pathologies increases.
How is Turner syndrome diagnosed?
Turner syndrome can be diagnosed before birth if the mother has an amniocentesis. Prenatal ultrasound may also be used to diagnose due to visualization of malformations in the head or neck of the fetus.
After birth, Turner syndrome will be diagnosed by physical characteristics in girls or by delayed sexual development when they reach puberty. Finally, to confirm that you have this condition, it will be necessary to do a karyotype test to see the chromosomes.
What is the prevalence of Turner syndrome in the population?
This chromosomal alteration is one of the most common. About 1 in 2,500 girls born worldwide have Turner syndrome.
Recommended reading
In addition to Turner syndrome, there are other chromosomal diseases that are compatible with life and can be detected thanks to PGD. If you are interested in reading more about this topic, you can read on in the next post: What Genetic Diseases Can PGD Test for?
As mentioned above, the donation of eggs is the most appropriate Treatment for women who would like to become mothers. In order to obtain more information about this topic, we recommend you to enter the following post: Donor-Egg IVF Procedure for Recipients – Protocol & Cost
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Alessandra Bernadete Trovó de Marqui. Turner syndrome and genetic polymorphism: a systematic review. Rev Paul Pediatr. 2015 Jul-Sep;33(3):364-71. doi: 10.1016/j.rpped.2014.11.014 (View)
Beatriz Donato, Maria João Ferreira. Cardiovascular risk in Turner syndrome. Rev Port Cardiol (Engl Ed). 2018 Jul;37(7):607-621. doi: 10.1016/j.repc.2017.08.008 (View)
Christa Hutaff-Lee, Elizabeth Bennett, Susan Howell, Nicole Tartaglia. Clinical developmental, neuropsychological, and social-emotional features of Turner syndrome. Am J Med Genet C Semin Med Genet. 2019 Mar;181(1):126-134 (View)
Matilde Calanchini, Christina Y L Aye, Elizabeth Orchard, Kathy Baker, Tim Child, Andrea Fabbri, Lucy Mackillop, Helen E Turner. Fertility issues and pregnancy outcomes in Turner syndrome. Fertil Steril. 2020 Jul;114(1):144-154. doi: 10.1016/j.fertnstert.2020.03.002 (View)
Mette Viuff, Claus H Gravholt. Turner Syndrome and Fertility. Ann Endocrinol (Paris). 2022 Aug;83(4):244-249. doi: 10.1016/j.ando.2022.06.001. Epub 2022 Jun 18 (View)
Sang Hoon Yoon, Ga Yeon Kim, Gyu Tae Choi, Jeong Tae Do. Organ Abnormalities Caused by Turner Syndrom. Cells. 2023 May 11;12(10):1365. doi: 10.3390/cells12101365 (View)
Shelli R Kesler. Turner syndrome. Child Adolesc Psychiatr Clin N Am. 2007 Jul;16(3):709-22 (View)
Thomas Morgan. Turner syndrome: diagnosis and management. Am Fam Physician. 2007 Aug 1;76(3):405-10 (View)
Tsuyoshi Isojima, Susumu Yokoya. Growth in girls with Turner syndrome. Front Endocrinol (Lausanne). 2023 Jan 12;13:1068128 (View)
FAQs from users: 'Is Turner syndrome hereditary?', 'Can women with Turner syndrome get pregnant naturally?', 'Can an advanced age cause the Turner syndrome?', 'How is Turner syndrome diagnosed?' and 'What is the prevalence of Turner syndrome in the population?'.
Authors and contributors






More information about Michelle Lorraine Embleton
