Assisted Reproductive Technology (ART), also referred to as assisted reproduction or assisted conception, can be defined as the set of techniques and medical treatments that allow individuals and couples to start a family when it cannot be achieved naturally due to infertility problems.
Nowadays, between 12% to 18% of couples willing to create a family suffer from infertility, with 50% of the cases due to male factor infertility, and the remaining 50% caused by female infertility. It can also occur that both members of the couple are childless.
There exist another group that has no alternative but to turn to fertility treatment to have babies: single males and females, as well as same-sex couples.
Currently, the main fertility treatments available for these patients to fulfill their dreams are, on the one hand, intrauterine insemination (IUI) and in vitro fertilization (IVF), which can be combined with other options such as third-party reproduction, also known as donor-assisted reproduction, or PGD (Preimplantation Genetic Diagnosis).
Provided below is an index with the 11 points we are going to expand on in this article.
- 1.
- 2.
- 3.
- 4.
- 4.1.
- 4.2.
- 4.3.
- 4.4.
- 5.
- 6.
- 7.
- 7.1.
- 7.2.
- 7.3.
- 7.4.
- 7.5.
- 7.6.
- 7.7.
- 7.8.
- 8.
- 9.
- 10.
- 11.
What is assisted reproduction?
The concept of assisted reproduction can be defined as the set of techniques and treatments that replace the natural process of reproduction with the aim of facilitating pregnancy.
Depending on the cause or origin of infertility, assisted reproduction professionals (gynecologists and embryologists) may intervene to a greater or lesser degree in the functioning of the male and female reproductive systems to help achieve pregnancy.
In general, it is possible to act in any of the parts of the reproductive process, but the most important are the following:
- Development of ovarian follicles
- Ovulation
- Transportation of human gametes: egg and sperm cells
- Fertilization: when sperm meets the egg

Assisted reproduction aims to safeguard each of the barriers that may exist naturally. To this end, professionals have the help of hormonal medication and techniques, more or less complex, such as artificial insemination (AI), intracytoplasmic sperm injection (ICSI), embryo culture, etc.
In addition, assisted reproduction has made great advances and, nowadays, it is possible to have donor gametes in the event of not being able to have biological children due to the risk of transmitting diseases or not having one's own gametes.
History of assisted reproduction
To overcome the barriers that can be found naturally in any of the processes listed above, we use fertility medications in combination with different methods, such as IUI and IVF. Moreover, there exists another method that provides even higher success rates: Intracytoplasmic Sperm Injection (ICSI).
Until the end of the 20th century, people with fertility problems had to resign themselves or resort to adoption if they wanted to start a family.
In 1978, all this changed with the birth of Louise Brown, the first "test-tube baby". Infertile people saw assisted reproduction as the solution to their problems in achieving pregnancy.
Louise Brown has been a natural mother, which has demonstrated that the use of assisted reproductive techniques does not imply the birth of infertile children.
The technique that allowed this first birth was IVF. An egg was removed from the patient and the union with the sperm was performed in a dish in the laboratory. The fertilized egg was divided up to eight cells and re-implanted in the mother.
The success of this first IVF opened the door to the whole range of techniques we know today as assisted reproduction.
In the beginning, fertility treatments did not offer high success rates. However, the different techniques have been perfected over the years, specialized professionals have been trained in this field, and more and more children are being born all over the world thanks to reproductive medicine.
Indications
To consider that a couple has fertility problems, they must spend one year having unprotected sexual intercourse without achieving pregnancy (6 months if the woman is older than 35 years). However, if it is known that there is an infertility problem, such as uterine malformations or genetic alterations, it does not make sense to wait this time.
In any of these cases, the couple should go to an assisted reproduction center to carry out a fertility study and find out the possible causes of their infertility.
In a very general way, the fertility alterations in men and women that prevent or hinder them from having a child naturally are the following:
- Male infertility
- poor seminal quality, absence of sperm, genetic alterations in sperm, etc.
- Female infertility
- alterations in the menstrual cycle, decreased quantity and / or quality of eggs, problems affecting embryo implantation, etc.

In addition, if there is any hereditary disease in the family that may result in the birth of a sick child, it is recommended not to attempt a natural pregnancy and to go to a clinic for a genetic study.
Nevertheless, single women and lesbian couples will also need to resort to assisted reproduction in order to become mothers. To do so, these women will have to undergo sperm donation treatment.
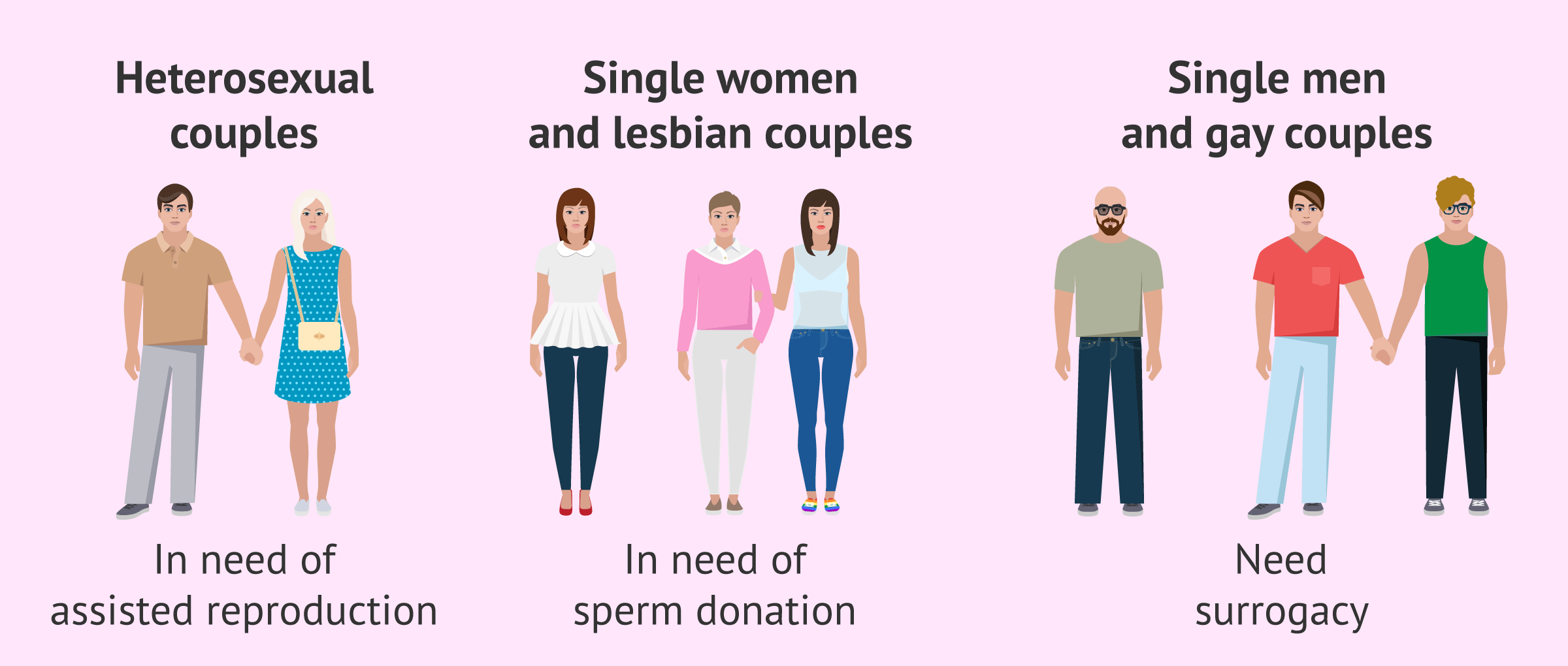
As for single men and gay couples, their only option to have children is surrogacy.
Assisted reproduction techniques
Assisted reproductive techniques in humans arise with the main objective of achieving a pregnancy that results in a healthy newborn.
Advances in science and new technologies allow the number of assisted reproductive techniques to be continuously increasing and, at the same time, the protocols and methods of the existing ones to be improved.
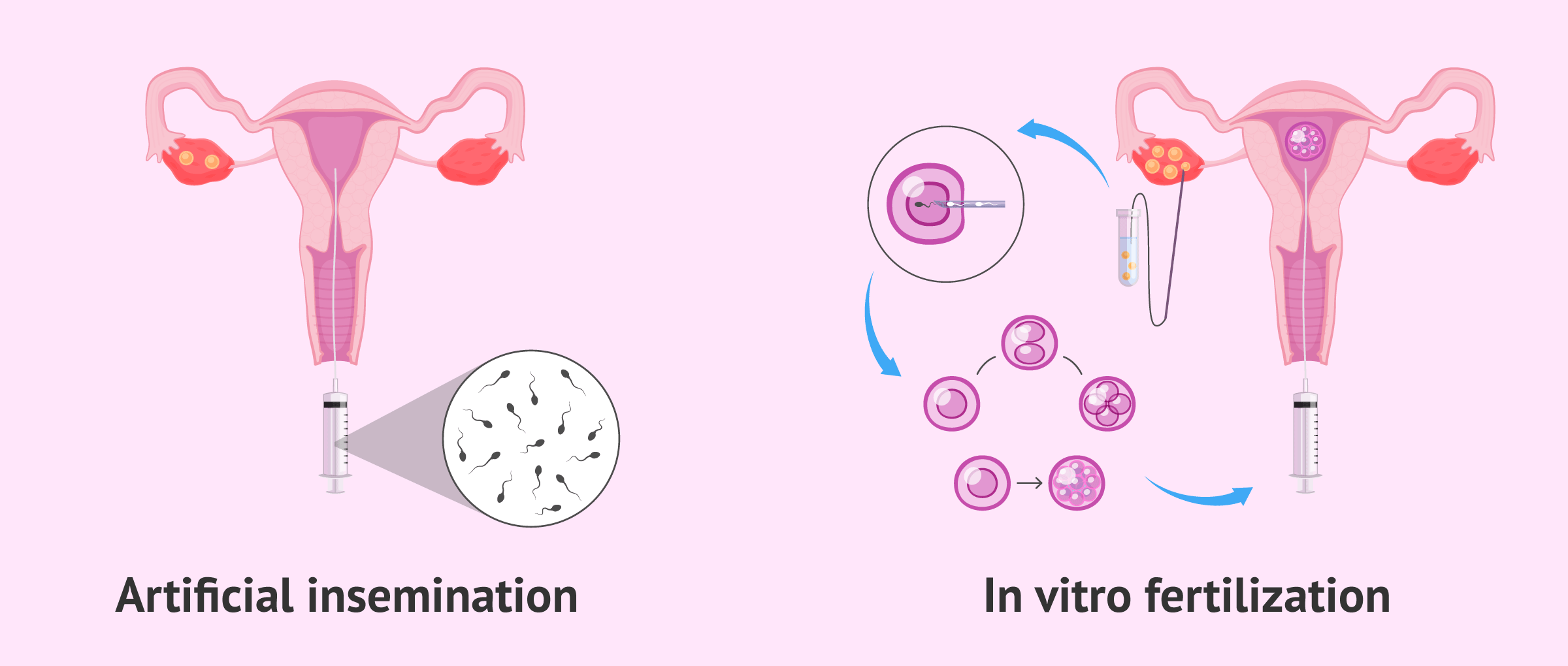
Artificial insemination (AI) and in vitro fertilization (IVF) are the most commonly used assisted reproductive techniques, each with its advantages and disadvantages. The choice of one technique or the other will depend basically on the type of infertility and medical recommendation.
In the first place, the simplest and least invasive method will always be tried. If there is a serious cause of infertility or if pregnancy is not achieved after several attempts, the specialist doctor will recommend a more complex reproductive technique.
Below we will explain the most important assisted reproductive techniques from the least to the most complex.
Inseminación artificial (IA)
It is the fertility treatment involving the lowest complexity and the most similar one to natural conception. It involves the insertion of sperm directly into the female reproductive system, usually in the womb, to ease make it easier for the sperm to reach the egg in the Fallopian tube, as it happens when pregnancy is achieved naturally.
Intrauterine insemination (IUI) can be done using the husband's sperm (AIH) or donor sperm (AID), which means that both opposite-sex and same-sex couples, as well as single females, can benefit from this fertility treatment.
This reproductive method requires a low degree of complexity, and involves three basic steps:
- Ovarian stimulation to trigger follicle growth, and ovulation induction
- Preparing the semen sample in the lab
- Inserting the sample with a catheter to inseminate the patient

AI can be performed either with the partner's sperm (AIH) or with donor sperm (AID). Therefore, this method can be used by heterosexual couples, as well as single women or lesbians.
To learn more about IUI, see also: Artificial insemination (AI): process, cost and types.
In Vitro Fertilization (IVF)
IVF is a method of assisted reproduction that consists of joining egg and sperm in the laboratory to create an embryo, which is then transferred to the woman's uterus. Unlike AI, IVF is a highly complex technique.
In general, the IVF procedure is as follows:
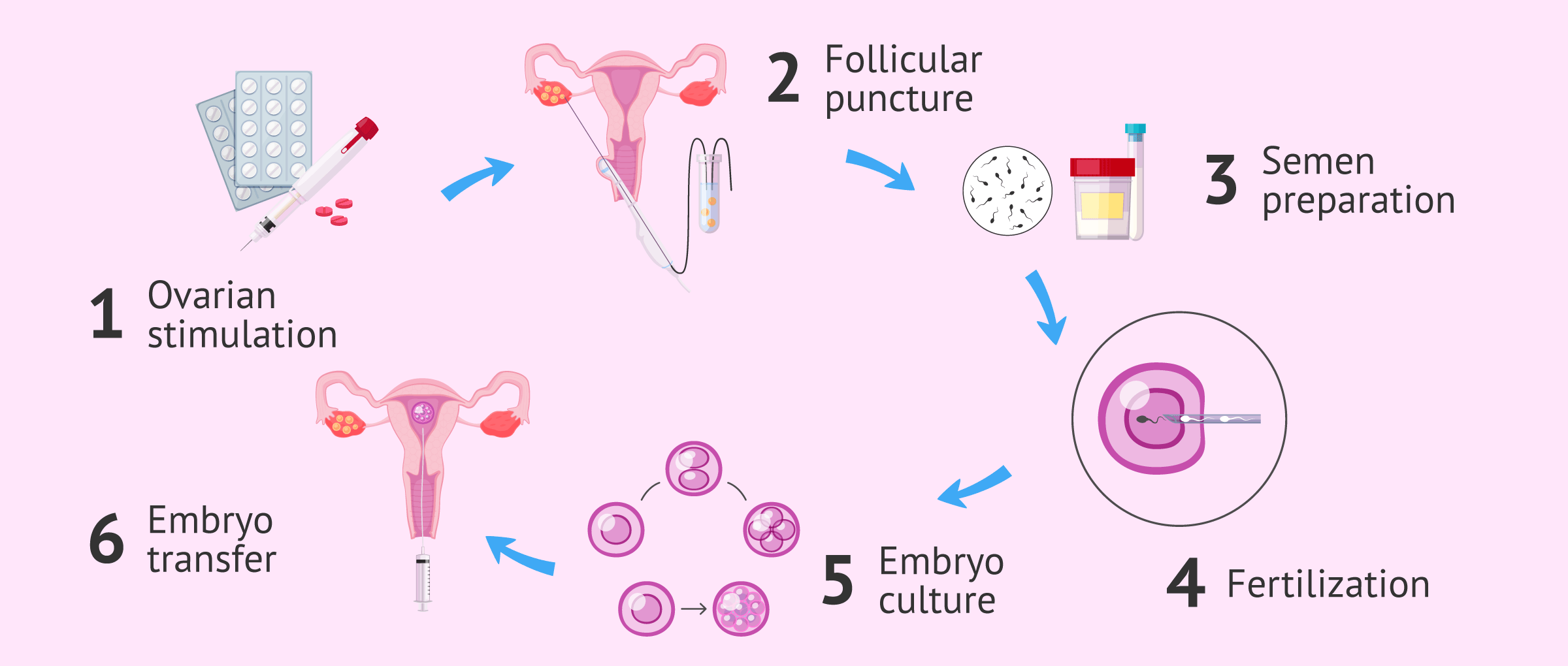
In both cases, the IVF procedure involves the following steps:
- Controlled ovarian stimulation (COS) so that multiple eggs mature in a single cycle
- Follicle puncture (ovum-pick up) to collect the eggs produced from the ovary
- Preparation of the semen sample at the laboratory
- Fertilization in the laboratory (by means of classical IVF or ICSI)
- Embryo culture and development
- Embryo transfer into the patient's womb
There are two types of IVF, depending on the method used for fertilization:
- Conventional IVF
- the egg is brought into contact with the sperm in a culture dish, so that fertilization takes place on its own.
- ICSI
- a sperm is selected and introduced into the ovule by microinjection, so fertilization is forced.
The semen used in IVF can be both semen from the partner and from a donor. The same happens with the eggs: if the woman cannot use her own, donor eggs can be used in the treatment known as egg donation .
For lesbian couples, there is a special type of IVF known as the Reciprocal IVF . This technique consists of using the ovules of one of the women of the couple, while the transfer of the embryos obtained will be made to the other woman. Thus, both participate in the process, providing the genetic material (the eggs) or carrying out the pregnancy.
Learn more about the IVF process, its success rates, and more in the following post: What is in vitro fertilization (IVF)?
Preimplantation Genetic Diagnosis (PGD)
ART also allows embryos to be genetically tested during IVF treatment. It is the preimplantation genetic diagnosis (PGT), currently known as preimplantation genetic test (PGT).
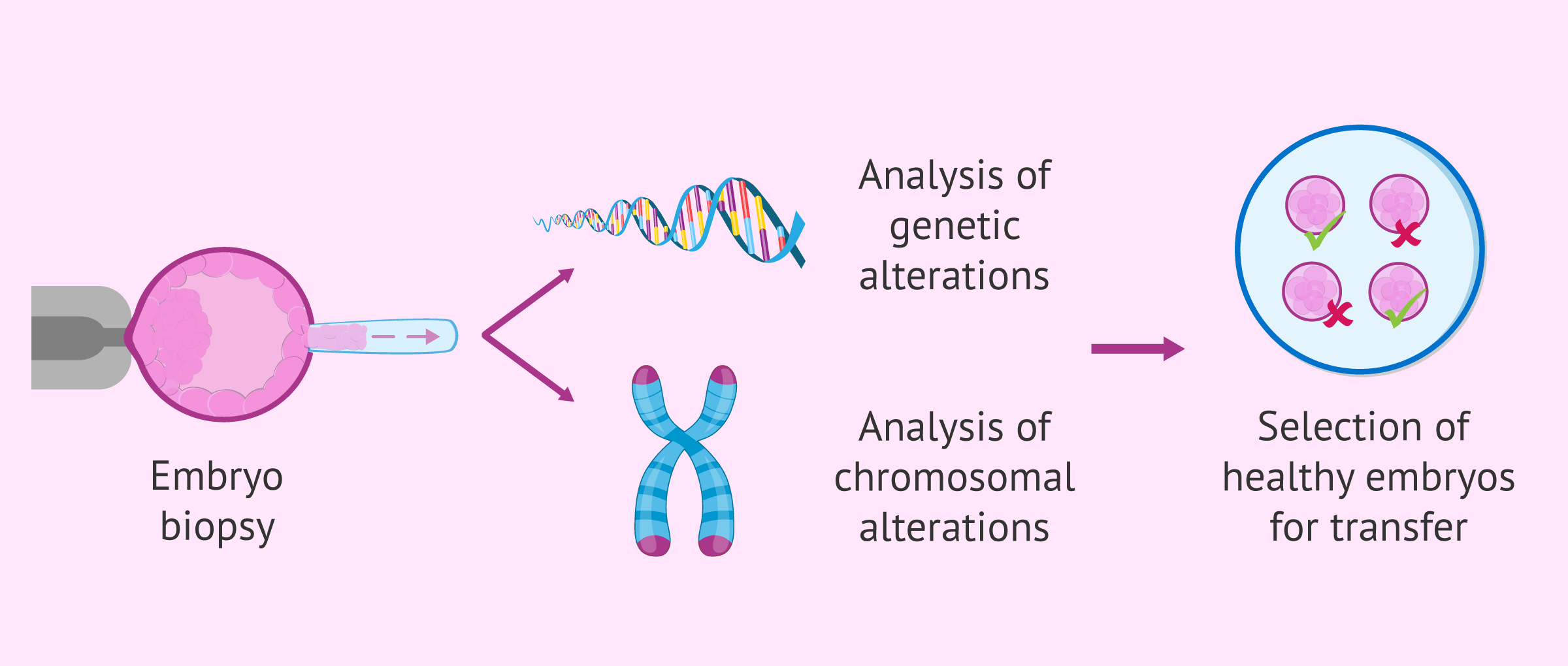
To do this, one or more cells are removed from the embryo, through a procedure known as an embryo biopsy. Later, it is analyzed if they present any chromosomal alteration or genetic mutation.
Finally, only genetically healthy embryos are selected for transfer to the woman's uterus. Those embryos that present any abnormality are discarded.
Get more info about this advanced technique by visiting this post: What is PGD or Preimplantation Genetic Diagnosis?
Surrogacy
Surrogacy or surrogate motherhood, commonly referred to as womb for rent or womb to rent, is another infertility treatment that involves a woman (the gestational carrier or surrogate), who carries someone else's child.
This fertility option is recommended for the following family types:
- Opposite-sex couples who cannot have a child naturally as a consequence of uterine problems, or after several failed IVF attempts.
- Lesbian couples and single females who cannot carry a pregnancy to term for the same reasons.
- Gay couples (man and man) and single males who wish to have a biological child.
This assisted reproduction technique has sparked several debates in the field of bioethics and, in fact, in Spain the law does not allow it .
We recommend that you read the following post to learn about this technique: IVF treatment abroad: costs, benefits and best countries.
Prices
The cost of infertility treatments depends mainly on the technique used, the country, and the fertility clinic chosen.
In Spain, artificial insemination can cost around €700–€1,700. This price range for artificial insemination is due to the fact that each assisted reproduction clinic sets its own prices, the services included in the package, and the origin of the sperm sample. Additionally, the cost of hormonal medication should be added, which usually represents an extra expense of €250–€600 depending on the required doses.
In contrast, the price of IVF is higher. In this case, IVF with own eggs and sperm costs around €3,500–€5,500, plus €1,000–€1,200 for hormonal medication. If it involves egg donation, the price increases to €4,500–€9,000.

It should be noted that, if you are carrying your IVF treatment in the United States, the cost might be even higher, as the healthcare system is privately funded. Moreover, fees can vary by state. So, broadly speaking, the cost of IVF can be as high as $10,000-$20,000.
The rates mentioned above can increase if additional procedures are needed, such as PGD or egg and/or sperm donation. For this reason, we strongly recommend that you ask various clinics for estimates or detailed quotes to find out what is included and what is not.
If you need to undergo IVF to become a mother, we recommend that you generate your Fertility Report now. In 3 simple steps, it will show you a list of clinics that fit your preferences and meet our strict quality criteria. Moreover, you will receive a report via email with useful tips to visit a fertility clinic for the first time.
The cost of fertility drugs is not usually included in the general quote for fertility treatments. So, you should keep in mind that you will have to add them to your budget.
Some clinics and agencies collaborate with medical insurance companies that can help you to reduce the costs associated with your treatment. In some countries such as the UK, some patients can get IVF treatment on the NHS.
Legal and social aspects
The increase in reproductive problems in society meant the need for a solution by medicine and the beginning of assisted reproduction. When the means to solve these infertility problems emerged, the legal regulation of these techniques was necessary to guarantee that they are applied in a moral and ethical way.
In Spain, Law 14/2006 on assisted human reproduction techniques has represented a great advance by allowing ART to be carried out within a legal framework.
The new methods available and the appearance of alternative family models to the traditional one have made society rethink the concept of family . This is no longer necessarily composed of a father, a mother and one or more children. Likewise, there does not have to be a genetic relationship, as occurs when a child has been adopted, the result of the donation of eggs and / or semen or the adoption of embryos.
On the other hand, especially with IVF and PGT techniques, the discussion about the beginning of human life and the moral and ethical implications of embryo manipulation has been raised. Here religious, cultural and social factors come into play.
FAQs from users
What are the objectives of assisted reproduction techniques?
The goal we aspire to is to generate a healthy gestation, with the minimum possible risks and complications, giving rise to healthy children.
Read more
What are the potential risks associated with assisted reproductive technology?
There is an increased risk of multiple births, especially with multiple-embryo transfers. This can occur with IUI if multiple eggs are produced in a single cycle as well.
To date, no study has confirmed that the use of assisted reproductive treatments increases the risk of fetal malformation, children born with diseases such as autism or other anomalies, etc. Apparently, no substantial differences with a natural pregnancy can be found.
What is assisted reproductive treatment?
Assisted reproductive treatment, officially known as Assisted Reproductive Technology (ART), refers to the set of fertility treatments that allow childless patients who are unable to have a child naturally achieve pregnancy.
What are the fertilization methods or treatments to achieve assisted childbearing?
There are two main treatments: artificial insemination and in vitro fertilization. The choice of one method or the other will depend on the fertility tests and the doctor's recommendation. Thus, it will be possible to obtain a good chance of pregnancy but using the simplest and least invasive technique possible.
How much does an artificial insemination cost? What about the price of in vitro fertilization?
An artificial insemination in the USA is around $700-$1600, while in vitro fertilization can cost $10,000-$20,000. These prices do not include the medication to stimulate the ovary and will depend on the clinic where it is done. If any additional analysis or technique is required, the price will also be higher.
Is there any fertility treatment more natural than artificial insemination?
Yes, directed intercourse or programmed intercourse, which consists of monitoring the woman's ovulatory cycle to have sexual intercourse when the doctor indicates, which will be on the days of ovulation, to increase the probability of pregnancy.
This can be done in a natural cycle, that is, in a woman's normal cycle, without applying hormones. If pregnancy is still not achieved, it can be attempted in a cycle with hormonal medication, that is, with ovarian stimulation.
How many types of assisted fertilization are there?
The assisted fertilization refers to assisted reproduction, so there are 2 main types: artificial insemination and in vitro fertilization. As we have already indicated in the article, within these techniques subtypes can be distinguished.
What is an in vitro pregnancy or in vitro method?
Both terms refer to in vitro fertilization, which is a procedure where fertilization, the union of the egg and sperm, is done in the laboratory rather than in the female reproductive tract.
Suggested readings
You can learn more about the details of each infertility treatment and the costs associated by visiting this post: Guide to infertility treatments.
Also, if you want to learn more about the concepts of infertility, sterility, and subfertility, you are invited to delve deeper into it by reading this interesting article: What is the difference between infertility, sterility and subfertility?
Finally, we have made reference here to third-party reproduction, but... do you know what does it exactly refer to and what is involved? Learn about it with our comprehensive guide: Definition, costs, and options for third-party reproduction.
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
The ESHRE Capri Workshop Group. Intrauterine insemination. Human Reproduction. 2009; 15 (3): 265 -277.
Hull MG, Glazener CM, Kelly NJ, Conway DI, Foster PA, Hinton RA, Coulson C, Lambert PA, Watt EM, Desai KM. (1985). Population study of causes, treatment, and outcome of infertility. Br Med J (Clin Res Ed); 291(6510):1693-7
Jones H. W. and Schrader C. (1988). In-Vitro Fertilization and Other Assisted Reproduction. Annals of The New York Academy of Sciences, Vol. 541, New York.
Pellicer A, Alberto Bethencourt JC, Barri P, Boada M, Bosch E, Hernández E, Matorras R, Navarro J, Peramo B, Remohí J, Riciarelli E, Ruiz A y Veiga A. Reproducción Asistida. En: Documentos de Consenso SEGO 2000:9-51.
Santamaría Solís, L. (2000). Técnicas de reproducción asistida. Aspectos bioéticos. En: Cuadernos de Bioética 2000/1ª. Asociación Española de Bioética y Ética Médica (AEBI).
Sociedad Española de Fertilidad (SEF) (febrero de 2012). Saber más sobre fertilidad y reproducción asistida. En colaboración con el Ministerio de Sanidad, Política Social e Igualdad del Gobierno de España y el Plan de Calidad para el Sistema Nacional de Salud.
WHO Laboratory Manual of Examination of Human Semen and Semen-Cervical Mucus Interaction. Cambridge: Cambridge University Press, 1999.
WHO Manual for standardized investigation and diagnosis and management of the infertile male. Cambridge: Cambridge University Press, 2000.
Zegers-Hochschild F. et al. (2010). Glosario de terminología en Técnicas de Reproducción Asistida (TRA). Versión revisada y preparada por el International Committee for Monitoring Assisted Reproductive Technology (ICMART) y la Organización Mundial de la Salud (OMS). Red Latinoamericana de Reproducción Asistida en 2010. Organización Mundial de la Salud 2010.
FAQs from users: 'What are the objectives of assisted reproduction techniques?', 'Why is assisted human reproduction an ethical issue?', 'What are the potential risks associated with assisted reproductive technology?', 'What is assisted reproductive treatment?', 'What assisted reproduction techniques take place in the lab?', 'What are the fertilization methods or treatments to achieve assisted childbearing?', 'When was intracytoplasmic sperm injection first used?', 'When is IVF recommended?', 'How much does an artificial insemination cost? What about the price of in vitro fertilization?', 'Is there any fertility treatment more natural than artificial insemination?', 'How many types of assisted fertilization are there?' and 'What is an in vitro pregnancy or in vitro method?'.
Authors and contributors








More information about Cristina Algarra Goosman

Hello, could anybody tell me if same-sex couples (lesbian) can undergo assisted reproduction? And what is the cost? How long would it take? Can we choose our baby’s sex?
Hello Marlene,
The answer is yes, lesbian couples can undergo assisted reproduction, although policies may vary from country to country.
As for sex selection, it is allowed in the following countries: United Kingdom, Australia, Canada, and the United States. Conversely, it is illegal in China and India, for example. In Spain, it is neither allowed, except in cases where there is some genetic alteration associated to gender, and as long as it is approved by a judge.
Best wishes
Hi, can I start a fertility treatment using my husband’s sperm? I’ve been told that you can only undergo fertility treatments, regardless of which one you choose, with donor sperm. I think this is senseless, isn’t it?
Hello,
This information is mistaken. In fact, the aim of fertility treatments is precisely that infertile couples are able to have children, and that’s why the husband’s sperm is used as long as it is possible. Donor sperm is used only in case the woman wishes to have a child without a male partner, or in case the man does not produce sperm or has a low sperm count.
My advice is that you visit a fertility clinic, undergo previous fertility testing and then choose the treatment that best fits your particular case.
Best wishes
Hi, I am wishing to have IVF this year in Málaga, could you inform me of the cost and process? I am from the UK. I have had one child via IVF.
Regards,
Amy
Dear Amy,
First of all, thank you for getting involved. If you want to travel to Spain to have a child via IVF, I recommend you to complete and submit our form to get estimates from different Spanish IVF clinics according to your own personal situation. You will find them after clicking the following link: Cost Calculator for Egg Donation & Treatments.
You can also visit our Clinic Directory to find different Spanish fertility clinics.
Should you need any further help, do not hesitate to ask 🙂
Best wishes
Do you have a team of specialists who are dealing with male infertility, to be precise, male with azoospermia? Is it possible to perform TESE and MicroTESE at your clinic? Thanx in advance
Hi Jelena,
We are not a clinic, this is an online magazine about infertility issues, donor conception, and assisted reproductive technology in general. If you need to visit a fertility specialist, my advice is that you take a look at our clinic directory.
Best wishes
Hi,
I got my tubes tied and I want to have a baby. I’m 33 years old, I hope you can help me or tell me if I can get help from the NHS. I look forward to your answer.
Hi Cathy
first of all the good news: depending on the type of tubal ligation you have, a tubal ligation reversal is possible and you may opt for intrauterine insemination. Alternatively, if tubal ligation reversal is not possible anymore or too complicated, doctors usually suggest undergoing in vitro fertilization. I suggest you read this post for more information: Is it possible to have a tubal ligation reversal?
Unfortunately, tubal ligation reversal is not available on the NHS. Therefore, I suggest you look for a private fertility clinic in your region which offers this technique.
For this, we have created our clinic directory, with which you can compare different fertility centers in order to choose the clinic that best fits you.
Hope this helps,
all the best.