A semen analysis or sperm test, also known as seminogram, semenogram or spermogram, is a diagnostic test which purpose is to evaluate the quality of sperm. Thanks to it, the specialist can assess various macroscopic parameters, including the pH and volume of the semen, as well as microscopic, like the sperm morphology, sperm motility, and sperm count.
The World Health Organization (WHO) has established reference values to determine what are normal results for a semen analysis report. Based on these guidelines and the results obtained, we can look for the presence of abnormalities that may lead to male infertility, and anticipate what are a man's chances of achieving pregnancy.
Provided below is an index with the 9 points we are going to expand on in this article.
- 1.
- 1.1.
- 2.
- 2.1.
- 2.2.
- 3.
- 4.
- 5.
- 5.1.
- 5.2.
- 5.3.
- 5.4.
- 5.5.
- 5.6.
- 5.7.
- 5.8.
- 5.9.
- 6.
- 7.
- 8.
- 9.
Procedure to perform the spermogram
For the results obtained to be reliable, the WHO establishes that the seminogram must be performed after a period of sexual abstinence of between 2 and 7 days. This not only includes the absence of sexual intercourse, but also of masturbation.
On the other hand, to establish a diagnosis of male infertility, it may be useful to have at least two seminograms at least one month apart. In this case, the result of both tests must match.
It must be taken into account that there may be alterations in the seminogram results due to environmental or laboratory variables, not only physiological ones.
Sample collection for the spermogram
The seminal sample will be obtained by masturbation, after having washed the hands and genitals properly, and will be deposited in a sterile container. This container is usually provided by the clinic, but can also be purchased at pharmacies.
It is crucial to collect the entire ejaculate sample. Many men feel uncomfortable or nervous and this causes them to lose part of the seminal sample, especially the first fraction.
In this case, if a part of the ejaculate is lost or the contents of the bottle spill, the seminal analysis will not be representative and, therefore, will not be considered valid. For this reason, it is important to notify the laboratory staff that the sample is not complete, in order to schedule a new collection.
The ideal is to collect the seminal sample in the clinic itself, to alter its conditions as little as possible. However, many clinics offer the possibility of obtaining the semen sample at home and delivering it quickly to the laboratory, as long as no more than half an hour elapses between obtaining the sample and arriving at the clinic.
In addition, until arrival at the laboratory, adequate temperature and light conditions must be maintained. For this reason, it is recommended to keep the bottle in a pocket or in contact with the body and wrapped in aluminum foil so that it is not exposed to light.
If you need to undergo IVF to become a mother, we recommend that you generate your Fertility Report now. In 3 simple steps, it will show you a list of clinics that fit your preferences and meet our strict quality criteria. Moreover, you will receive a report via email with useful tips to visit a fertility clinic for the first time.
Normal values of the spermogram (WHO)
In 2010, the WHO published some seminal reference values, below which the semen sample is considered abnormal.
The sperm evaluation process is divided into the macroscopic and microscopic examinations. In general, the basic parameters determined by the WHO are analyzed. However, depending on the clinic or the laboratory, there may be variations in the procedure.
Macroscopic analysis
The macroscopic analysis is the first to be performed. It evaluates semen characteristics such as the following:
- Volume
- is expressed in milliliters (ml) the amount of semen expelled during ejaculation. From 1.5 ml is considered a normal seminal volume.
- Liquefaction
- occurs by letting the sample rest for about 20 minutes at room temperature and is a process by which the semen becomes less compact. In this way, the liquefaction allows the microscopic examination of the sample to be carried out correctly.

- Viscosity
- the formation of threads is analyzed. In the event that there is an extreme viscosity, the threads must be broken so that the sperm can circulate freely through the seminal fluid.
- Color
- semen, under normal conditions, has a grayish white or slightly yellowish color. If it presents another appearance, it may be indicative of infection.
- pH
- normal pH values for semen are between 7.2 and 8.0, which are considered slightly basic values. The variation in pH can indicate the presence of an infection or alterations in the production of seminal fluid.
Microscopic analysis
At a microscopic level, the most important seminal parameters that are evaluated are:
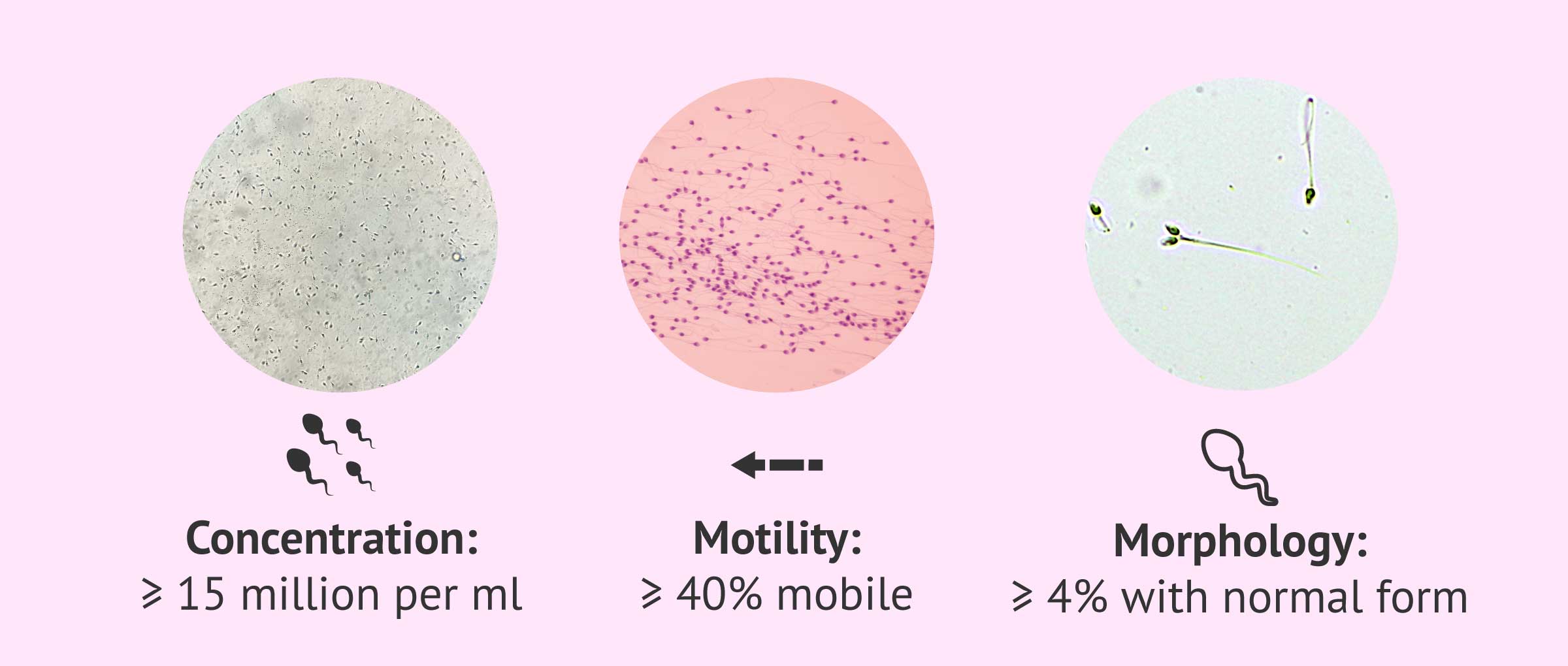
- Spermatozoa concentration
- two values are given . On the one hand, the concentration of spermatozoa per milliliter is calculated, which from 15 million/ml is considered normal. On the other hand, the total number of sperm in the ejaculate is determined, which the WHO considers normal from 39 million sperm/ejaculate.
- Motility or sperm motility
- the capacity of movement of the spermatozoa is analyzed. Generally, two values are given: the total movement (all the sperm that show movement are counted), which must reach at least 40%, and the progressive motility (the sperm that move and advance in position), whose minimum value is found at 32%. In some clinics, the type of movement is also analyzed: if it is fast, moderate, or slow.
- Vitality
- is evaluated by means of a stain test. This parameter is usually analyzed only in those cases where a large number of immotile sperm are found. In this way, it can be checked whether these sperm are alive (but immobile) or dead. The reference value for vitality is that there must be at least 58% live sperm.
- Morphology
- the shape of the head, the middle piece or neck, and the tail of the spermatozoon. The WHO qualifies as a normal seminal sample for morphology one that contains more than 4% of sperm with normal shape, that is, without abnormalities in any of its parts.
- Presence of leukocytes or epithelial cells
- it is usual that, in addition to spermatozoa, some other type of cell is found in semen, such as leukocytes or epithelial cells due to desquamation of the skin. In samples with a high presence of leukocytes, the presence of an infection is suspected.
Dr. Sergio Rogel speaks in an interview about all of the aspects evaluated during a seminogram:
Classically, during a semen analysis, macroscopic aspects of the semen sample are evaluated, such as volume, pH, consistency, color; and then the microscopic parameters are analyzed, which are the most important, including sperm count, concentration per milliliter, motility, and the normality of the semen shapes. This is typically the seminogram that everyone knows.
In addition, nowadays there are other aspects that we can look at in a semen sample, which is not really what we would call a semen analysis, but they are techniques that can be used and they would be called advanced semen analysis, such as the study of apoptosis in the sperm, DNA fragmentation, and so on.
What is the REM seminogram?
Another test that can be done as a complement to the seminogram is the motile sperm count or REM. If done, we would speak of seminogram or REM spermiogram.
The seminogram REM consists of the separation of spermatozoa based on their mobility. To obtain the motile sperm fraction, the ejaculate sample is subjected to a process called sperm capacitation.
There are several methods to train the seminal sample, although the main ones are swim-up and density gradients.

Thus, a fraction of the concentrated sample with the most motile spermatozoa is obtained. In this way, depending on the semen quality obtained, it will be possible to evaluate more efficiently the assisted reproduction technique that offers the greatest probability of success.
For example, it may happen that a basic semen analysis shows an optimal concentration and motility, but the sample does not respond well to the preparation and is not of good quality after capacitation. This will make it inadvisable to perform artificial insemination (AI) since the chances of achieving pregnancy with this technique will be low.
A semen sample is considered suitable for AI when it has a number of spermatozoa with progressive motility (a+b) higher than 3-5 million in the EMR.
How much does a semen analysis cost?
Normally, the cost range for semen analysis is $50-300, although it varies from clinic to clinic, and can be higher if it is done without insurance—more often than not, the price of out-of-pocket semen analyses is $275 approximately.
Many of the costs of fertility tests are usually covered by health insurance plans, but we recommend that you ask your health insurance provider for detailed information on what's covered and what's not.
As mentioned earlier, the total price of semen analysis testing depends on the type of exam ordered. It should be clear that not all clinics and/or labs charge the same fees, and not all may include the same parameters. For example, some clinics do not include morphology in the most basic semen analysis. This means that you have to pay an extra amount to have the morphology of your sperm analyzed as well.
If you prefer to collect the specimen at home, the cost of at-home semen analysis kits is $150 with insurance, or more than $250 without insurance, plus an average fee for shipping that varies from lab to lab.
FAQs from users
What are normal sperm values?
As for the normal values of a spermiogram or also called seminogram, the most important ones are:
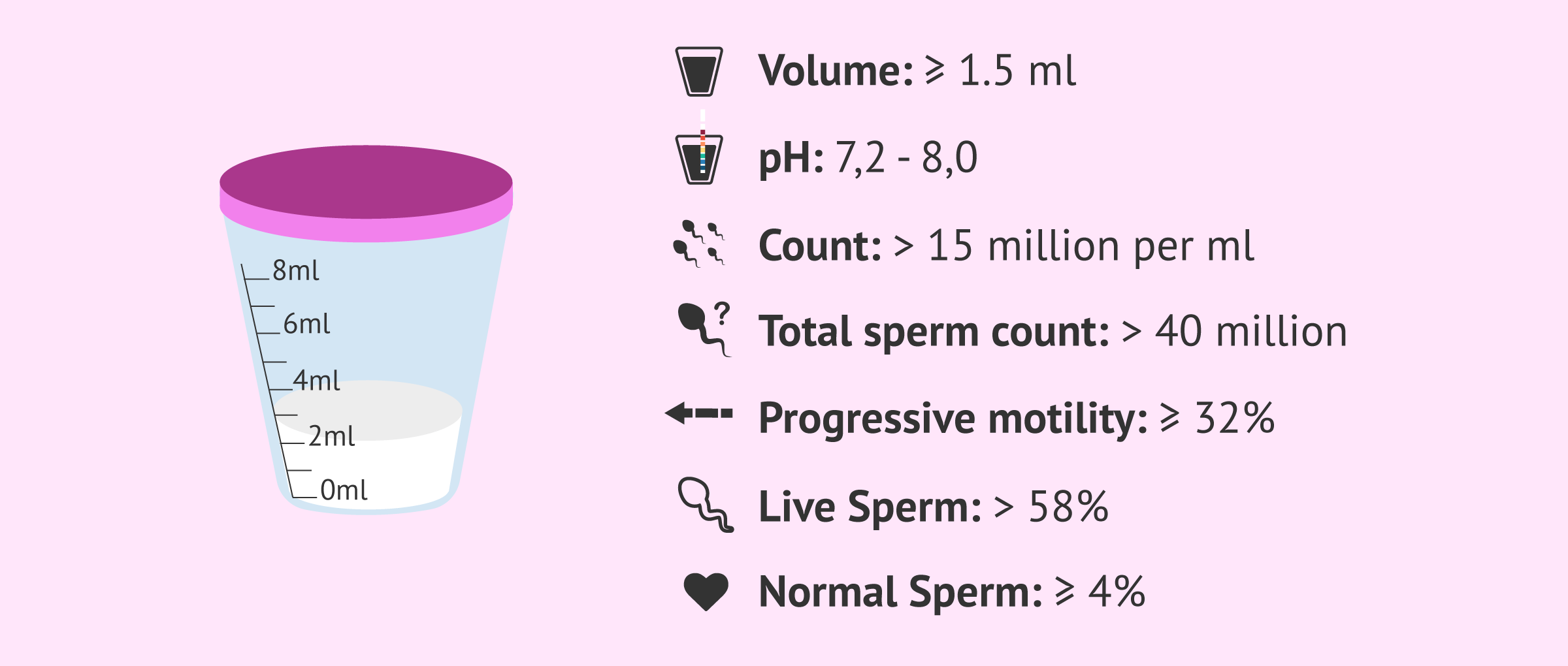
- Sample volume ≥ of 1.5 ml
- pH between 7.2 and 8.0
- Sperm concentration ≥ of 15 million/ml
- Total sperm count > 40 million
- Progressive motility (A+B) ≥ of 32%
- Living spermatozoa > of 58%
- Normal spermatozoa ≥ of 4%
- REM (sperm capacitation) > 5 million, being this the most determining parameter of the seminogram
What recommendations should be taken into account before performing a semen analysis?
Before performing a seminogram or analysis of the semen sample and to guarantee the maximum reliability of the diagnosis, the semen sample must be obtained following a series of specific indications:
- A sexual abstinence of 2-4 days. The limits are no less than 2 nor more than 4 days of abstinence.
- Sample collection in a sterile pharmacy cup.
- The way to obtain the sample is through masturbation, neither coitus interruptus nor the use of commercial condoms being valid.
- Maximum hygienic conditions in sample collection (previous handwashing).
- The semen sample must be collected completely, if part of it is spilled, it will not be valid.
- A maximum of 1 or 1.5 hours should elapse from collection to delivery to the laboratory, the delay in time may affect the mobility of the sperm.
- It is important to keep it at room temperature and avoid significant fluctuations in temperature.
- Notify if you are taking any medication or if you have had a fever in the last few days.

Can having a fever affect the result of the semen analysis?
When a male suffers a feverish period, sperm production is hampered and may even stop for a short period of time. Therefore, fever is usually associated with a decrease in sperm count and altered sperm motility and morphology.
Read more
How much does it cost to get a sperm analysis?
The general rate for a lab semen analysis in the United States of America ranges between $100 and $300, although it varies from US state to state.
In the United Kingdom, a basic semen analysis costs £130 approximately. Finally, in Canada, it costs 250 CAD on average.
Where can I get a spermogram?
The most common places for this diagnostic test are assisted reproduction clinics and clinical analysis laboratories.
It can also be performed at the Social Security if the doctor considers it necessary and indicates it.
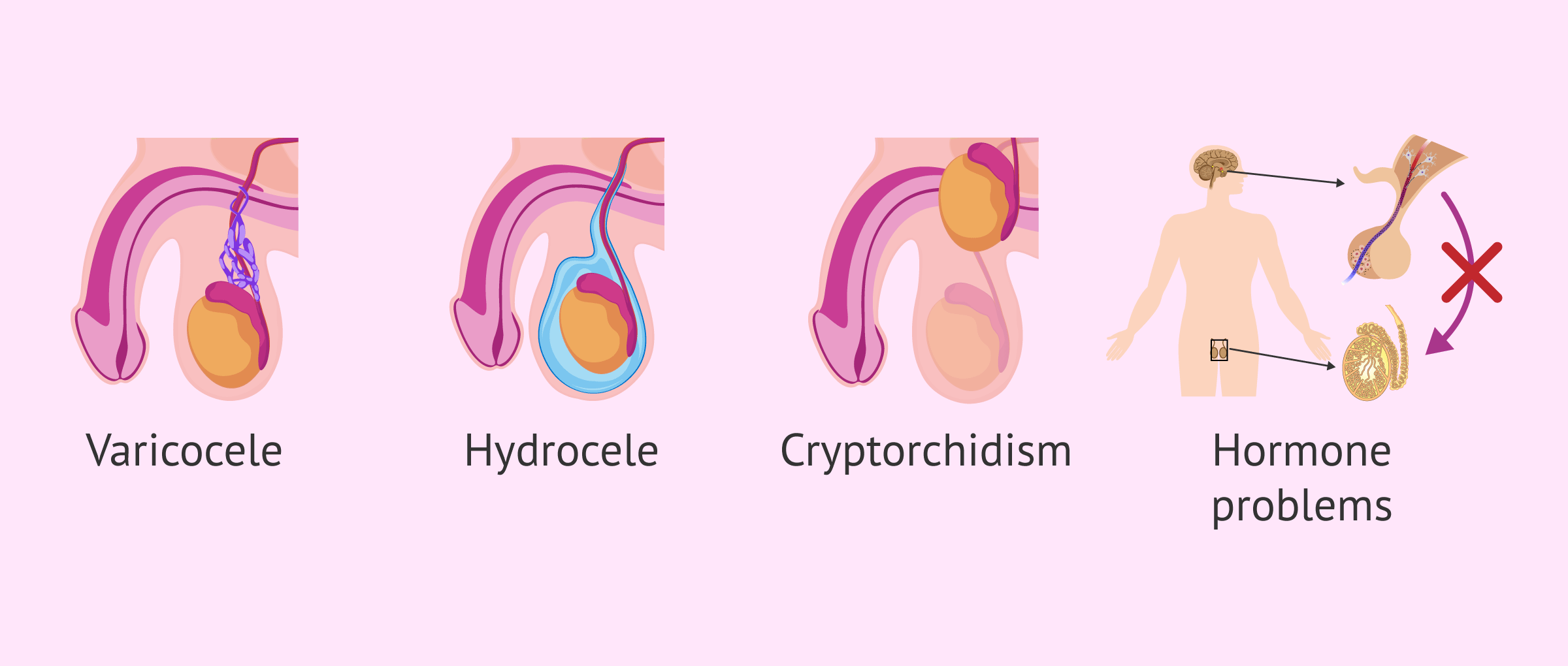
Are there diseases that cause sperm problems?
Yes, there are certain testicular diseases such as varicocele, hydrocele, cryptorchidism and some genetic diseases that can alter normal sperm production and cause infertility.
Hormonal problems such as hypogonadism, hyperprolactinemia, hyperthyroidism, hypothyroidism and diabetes also affect sperm development.
If the seminal ducts and accessory glands have any abnormalities, sperm maturation and ejaculation may be impaired.
What medications are needed for the spermiogram?
There is no medication that has to be taken for a semen analysis. However, in case any alteration is detected in the spermogram, the physician may prescribe the patient a nutritional supplement to improve the seminal quality during the following 3 months and evaluate if there is an improvement with a new semen analysis.
Does Enterococcus faecalis in semen cause infertility?
This microorganism is a gram-positive bacterium that is usually found in the male urethra and is part of the bacterial flora. However, it can sometimes ascend through the urogenital tract and trigger an infection.
Enterococcus faecalis is the most common cause of infections affecting the prostate and semen. As in any infection that affects the reproductive system, it could cause infertility, which would be resolved with antibiotic treatment. Only if the infection is acute and not treated in time can it cause permanent infertility.
How long before sperm test results?
It depends on the lab you are working with and their workload, of course. Technically, the results of a sperm test can be obtained on the same day after the collection of the sample. However, in practice, it takes about 2-3 days.
Recommended readings
After getting the results of a semen analysis, the patient is given a diagnosis. The following article explains to you how to understand it: How to Interpret the Results of a Semen Analysis.
Also, if you want to learn more about the sperm capacitation or washing procedure, you can get more info here: Instructions & How to Prepare for a Semen Analysis.
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Andrade-Rocha FT. Semen analysis in laboratory practice: an overview of routine tests. J Clin Lab Anal. 2003;17(6):247-58. (See)
Baker DJ. Semen analysis. Clin Lab Sci. 2007 Summer;20(3):172-87; quiz 188-92. (See)
Cardona Maya W. Manual de procesamiento de semen humano de la Organización Mundial de la Salud-2010 [World Health Organization manual for the processing of human semen-2010]. Actas Urol Esp. 2010 Jul;34(7):577-8. Spanish. (See)
Comhaire F, Vermeulen L. Human semen analysis. Hum Reprod Update. 1995 Jul;1(4):343-62. doi: 10.1093/humupd/1.4.343. (See)
Condorelli RA, Calogero AE, Russo GI, La Vignera S. From Spermiogram to Bio-Functional Sperm Parameters: When and Why Request Them? J Clin Med. 2020 Feb 3;9(2):406. (See)
Cooper TG, Noonan E, von Eckardstein S, Auger J, Baker HW, Behre HM, Haugen TB, Kruger T, Wang C, Mbizvo MT, Vogelsong KM. World Health Organization reference values for human semen characteristics. Hum Reprod Update. 2010 May-Jun;16(3):231-45. (See)
Esteves SC. Clinical relevance of routine semen analysis and controversies surrounding the 2010 World Health Organization criteria for semen examination. Int Braz J Urol. 2014 Jul-Aug;40(4):443-53. (See)
Franken DR, Oehninger S. Semen analysis and sperm function testing. Asian J Androl. 2012 Jan;14(1):6-13. (See)
Guzick DS, Overstreet JW, Factor-Litvak P, Brazil CK, Nakajima ST, Coutifaris C, Carson SA, Cisneros P, Steinkampf MP, Hill JA, Xu D, Vogel DL; National Cooperative Reproductive Medicine Network. Sperm morphology, motility, and concentration in fertile and infertile men. N Engl J Med. 2001 Nov 8;345(19):1388-93. (See)
Kruger TF, Menkveld R, Stander FS, Lombard CJ, Van der Merwe JP, van Zyl JA, Smith K. Sperm morphologic features as a prognostic factor in in vitro fertilization. Fertil Steril. 1986 Dec;46(6):1118-23. (See)
La Vignera S, Calogero AE, Condorelli R, Garrone F, Vicari E. Spermiogram: techniques, interpretation, and prognostic value of results. Minerva Endocrinol. 2007 Jun;32(2):115-26. (See)
Rogers BJ, Bentwood BJ, Van Campen H, Helmbrecht G, Soderdahl D, Hale RW. Sperm morphology assessment as an indicator of human fertilizing capacity. J Androl. 1983 Mar-Apr;4(2):119-25. (See)
Sociedad Española de Fertilidad (SEF). Manual de Andrología. Coordinador: Mario Brassesco. EdikaMed, S.L. (2011) ISBN: 978-84-7877. (See)
Sigman M, Baazeem A, Zini A. Semen analysis and sperm function assays: what do they mean? Semin Reprod Med. 2009 Mar;27(2):115-23. (See)
WHO laboratory manual for the examination and processing of human semen, 5th ed. Geneva: World Health Organization ; 2010. (See)
WHO laboratory manual for the examination and processing of human semen, sixth edition. Geneva: World Health Organization; 2021. (See)
FAQs from users: 'What are normal sperm values?', 'What recommendations should be taken into account before performing a semen analysis?', 'How long should you abstain before a sperm analysis?', 'Can having a fever affect the result of the semen analysis?', 'Can you do a sperm analysis at home?', 'What is the ideal motile sperm count for IUI?', 'How long should you wait for sperm test after vasectomy?', 'How much does it cost to get a sperm analysis?', 'Where can I get a spermogram?', 'Do the results of a sperm analysis improve after vasectomy reversal?', 'Are there diseases that cause sperm problems?', 'How much can a Sperm DNA Fragmentation test cost?', 'What medications are needed for the spermiogram?', 'What is WBC count in sperm analysis?', 'Does Enterococcus faecalis in semen cause infertility?', 'How long before sperm test results?', 'Do you always need a referral to get a sperm analysis?', 'Is there a sperm test to detect the gender in sperm?' and 'They found sperm in my urine test, is it normal?'.
Authors and contributors









More information about Cristina Algarra Goosman

Hi,
I suffering with Azoospermia,
In my report Impression:
SMALL AREA OF CALCIFICATION SEEN IN RIGHT TESTIS S/0? CALCIFIED GRANULOMA
Please tell me any treatement is there, Already I taken Ayurvedic treatment, But no luck,
I am not understand what I do, Please Adice.
Many Thanks,
vijju
Hello,
Your question has been already answered here: Small area of calcification seen in right testis? Calcified granuloma.
Hope this helps,
Best