Hyperprolactinemia is a hormonal disorder that can occur in both men and women. It is caused by excess levels of the hormone prolactin in the blood.
Generally, it is more common to find hyperprolactinemia as a cause of female sterility, as the excess of the hormone prolactin causes alterations in the menstrual cycle and anovulation.
The causes of this disorder are very diverse, ranging from normal pregnancy and lactation to the appearance of benign tumors in the pituitary gland. However, these are ot the only reasons why an excessive increase in blood prolactin levels may occur.
Provided below is an index with the 10 points we are going to expand on in this article.
- 1.
- 2.
- 3.
- 4.
- 5.
- 5.1.
- 6.
- 6.1.
- 6.2.
- 6.3.
- 6.4.
- 6.5.
- 7.
- 8.
- 9.
- 10.
Prolactin hormone
Prolactin (PRL) is a hormone secreted by the pituitary gland, a gland at the base of the brain. Its main function is to stimulate the production of colostrum and breast milk in the mammary glands after childbirth.
Prolactin is also involved in the synthesis of progesterone during the luteal phase of the menstrual cycle.
Although the level of the hormone prolactin usually increases during pregnancy and lactation, it is normal for an adult woman to have values between 0 and 20 ng/ml.
Hyperprolactiemia is a pathology characterized by an increase in the hormone prolactin in the blood, with a concentration higher than 30 ng/ml.
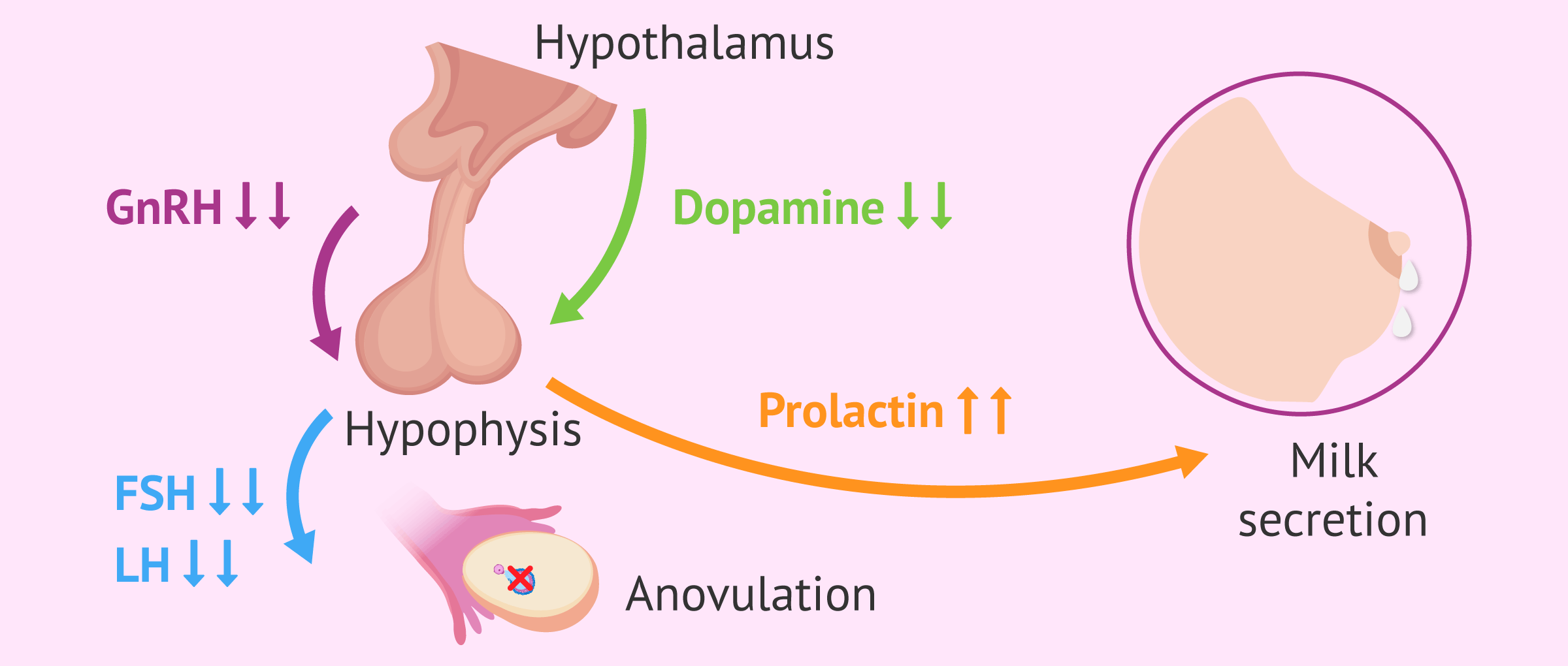
Abnormal blood prolactin levels can alter the menstrual cycle, produce anovulation and, consequently, infertility.
In particular, excess prolactin inhibits the secretion of GnRH (gonadotropin-releasing hormone), which in turn affects the production of FSH and LH hormones, responsible for follicular development and ovulation.
It is also common for women with polycystic ovary syndrome (PCOS) to have hyperprolactinemia due to increased estrogen production.
Causes of hyperprolactinemia
As we have already mentioned, pregnancy is the main cause of hyperprolactinemia in women. During gestation, the prolactin level may increase to 300 ng/ml.
The same is true during breastfeeding, in which the baby stimulates the nipple when sucking milk causing continuous blockage in dopamine secretion. As a consequence, the decrease in dopamine causes more prolactin to be secreted, as both hormones are regulated by a negative feedback system.
However, these are normal physiological situations in a woman's life in which the increase in blood prolactin is transient, just as it occurs during deep sleep, physical exercise, or orgasm. Once lactation is over, prolactin will return to normal levels and the menstrual cycle will re-establish itself.
Also, hyperprolactinemia can have some pathological causes, such as the following:
- Hypothyroidism
- Pituitary adenomas (prolactinomas)
- Chronic renal failure
- Polycystic ovary syndrome (PCOS)
- Hyperandrogenism
- Anorexia nervosa
- Stress and anxiety
- Multiple Sclerosis
- Cancer and pituitary tumors

There is also a type of iatrogenic hyperprolactinemia, caused by external factors such as neuroleptic drugs, antidepressants, anxiolytics, tranquilizers, opioids (morphine derivatives), and so on. All these drugs decrease the action and synthesis of dopamine.
Finally, oral contraceptive pills with estrogens may also produce a moderate increase in circulating prolactin in the blood.
Signs and symptoms
Everyone is different and not everyone will have the same symptoms when they have high levels of prolactin in their blood. The following are the most important signs and symptoms of hyperprolactinemia:
- Galactorrhea: secretion of milk by the mammary glands. It occurs in 30% of cases.
- Primary or secondary amenorrhea: disappearance of menstruation.
- Headaches and visual field alterations. These symptoms are caused by tumors.
- Hirsutism, if the woman has PCOS and/or hyperandrogenism.
- Osteroporosis, especially in cases of hypogonadism.
- Decreased libido and dry vagina.
- Infertility, mainly due to chronic anovulation.

It is not necessary for a woman to have all of these symptoms at once to make a diagnosis of hyperprolactinemia. Sometimes only the most common ones take place.
Furthermore, symptoms in men suffering from hyperprolactinemia include decreased sexual desire, infertility, visual disturbances, galactorrhea and even osteoporosis and decreased muscle mass.
Assisted procreation, as any other medical treatment, requires that you rely on the professionalism of the doctors and staff of the clinic you choose. Obviously, each clinic is different. Get now your Fertility Report, which will select several clinics for you out of the pool of clinics that meet our strict quality criteria. Moreover, it will offer you a comparison between the fees and conditions each clinic offers in order for you to make a well informed choice.
Diagnosis
The first diagnostic test that should be done in any patient with suspected hyperprolactinemia is to meaure bloodprolactin levels.
To do this, a blood test must be done between the third and fifth day of the menstrual cycle, when the ovaries are at rest and hormones at basal levels.
As indicated above, blood prolactin levels greater than 30 ng/ml indicate hyperprolactinemia disorder. If a prolactin result between 20 and 40 ng/ml is obtained, the analysis will be repeated to confirm the diagnosis.

In addition, it is important to review the medical history of the patient to determine the cause of this hormonal disturbance. Firstly, pregnancy has to be ruled out, and it must be taken into account whether the patient takes oral contraceptives, anxiolytic drugs, antidepressants, etc.
Finally, it is also important to rule out the presence of any pituitary tumor using computed tomography (CT) or magnetic resonance imaging (MRI), especially if hyperprolactinemia is not associated with hypothyroidism.
A blood prolactin value greater than 200 ng/ml in a non-pregnant woman may indicate a pituitary tumor.
If the cause of the high prolactin is not found after all tests have been performed, the patient will be told that she suffers from idiopathic hyperprolactinemia.
Treatment
Before starting treatment to lower the level of prolactin in the blood, we need to know the exact cause of this hormonal disorder.
In the case of drugs that are causing hyperprolactinemia, it will be enough to stop taking these substances to restore normal prolactin levels.
If high prolactin is the result of hypogonadism, the endocrinologist may indicate thyroid hormone replacement therapy.
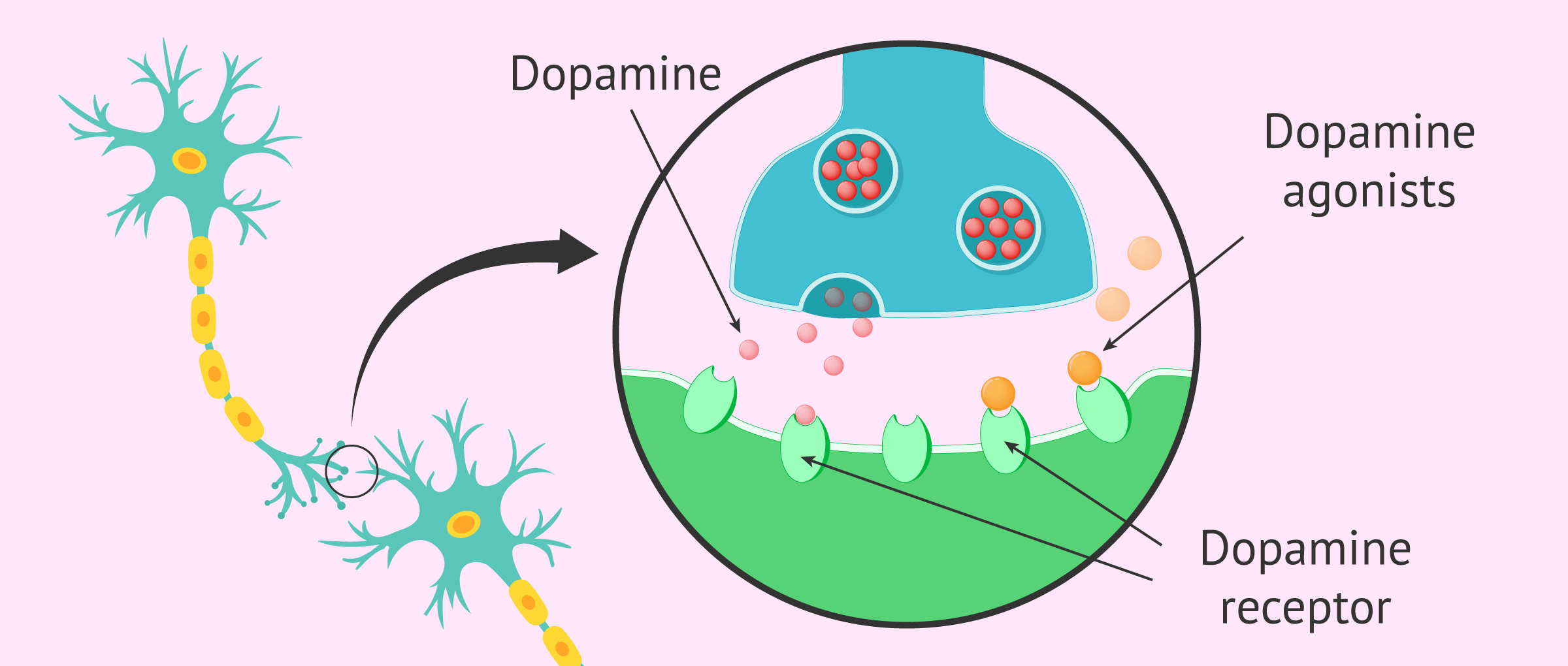
In other situations, such as pituitary adenomas or prolactinomas, the treatment of hyperprolactinemia is based on the administration of dopamine agonist drugs, such as cabergoline or bromocriptine. These substances act like dopamine, inhibiting the production of prolactin in the pituitary gland.
Generally, this type of treatment is the most widely used in order to restore prolactin levels soon and restore fertility, especially in young patients who want to get pregnant. However, a woman can spend months or even years on these medications.
If drug treatments do not work, or if large prolactinomas are found, surgery or radiation therapy may be needed to remove the tumor. The latter is less used because it takes a very long treatment for prolactin levels to return to normal.
Hyperprolactinemia and infertility
When the cause of hyperprolactinemina is clear, the best thing to do is to treat the cause in order to get the hormone levels in the blood normalized. In addition, as prolactin levels return to normal, FSH and LH hormone levels will also be regulated. This will restore the woman's ovarian function and reproductive capacity.
However, if the cause of the increased prolactin levels in women is unknown, it will be difficult to establish a specific and personalized treatment.

In these cases, those women diagnosed with hyperprolactinemia and that it is not possible to solve, may have to turn to assisted reproduction techniques to achieve pregnancy.
FAQs from users
Can I get pregnant with high prolactin?
Once the cause of hyperprolactinemia has been determined, prolactin (PRL) is normalised. With proper management, most women can become pregnant.
Bromocriptine and cabergoline are drugs used for treatment and are not teratogenic.
In the case of macroadenomas near the optic chiasma and which do not present a significant reduction in tumor volume with dopamine agonists, the best pre-pregnancy therapeutic option is transsphenoidal surgery.
Read more
Do men also suffer from hyperprolactinemia?
Yes, although it's less common. In this case, a man is considered to have hyperprolactinemia when his blood prolactin hormone level is above 20 ng/ml.
The main clinical manifestations of hyperprolactinemia in men are erectile dysfunction, decreased libido, gynecomastia (an increase in breast tissue) and infertility.
Does Hyperprolactinemia make you gain weight?
That might happen. This is because prolactin hormone irregularities may influence other metabolic pathways related to weight gain.
Can hyperprolactinemia be cured?
This depends on the exact cause that is causing the prolactin hormone surge.
When excess prolactin is due to physiological causes such as pregnancy or breastfeeding, normal levels of this hormone will be restored as soon as the mother stops breastfeeding and recovers her regular menstrual cycles.
If there is a pathological cause, the woman may have to live for long periods of time with hyperprolactinemia. However, dopamine antagonist drugs can help to achieve normal prolactin levels in these cases.
Can stress be a cause of hyperprolactinemia?
Yes, stressful situations can lead to an increase in prolactin levels in the blood. If a woman suffers prolonged stress over time, her ovulation will be affected, leading to fertility problems.
Recommended reading
Apart from prolactin, there are other hormones involved in the female reproductive system that can cause infertility. For more information related to this topic, you can access this article: Female hormone analysis: what should normal hormone levels be?
If you want to know more about breastfeeding and its effect on the menstrual cycle during it, we recommend reading the following post: Feeding your newborn baby - breastfeeding or formula feeding?
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Cristina Laguna Benetti-Pinto, Andrea Prestes Nácul, Ana Carolina Japur Rosa E Silva, Gustavo Arantes Rosa Maciel, Vania Dos Santos Nunes Nogueira, Paula Condé Lamparelli Elias, Manoel Martins, Leandro Kasuki, Heraldo Mendes Garmes, Andrea Glezer. Hyperprolactinemia in women: treatment. Rev Bras Ginecol Obstet. 2024 Apr 25:46:e-FPS05. doi: 10.61622/rbgo/2024FPS05. eCollection 2024 (View)
Freeman ME, Kanyicska B, Lerant A, Nagy G. Prolactin: structure, function, and regulation of secretion. Physiol. Rev. 2000;80:1523-1631 (View)
Grattan DR. Behavioural significance of prolactin signalling in the central nervous system during pregnancy and lactation. Reproduction. 2002;123:497-506 (View)
Melgar V, Espinosa E, Sosa E, Rangel MJ, Cuenca D, Ramírez C, Mercado M. Current diagnosis and treatment of hyperprolactinemia. Rev Med Inst Mex Seguro Soc. 2016 Jan-Feb;54(1):111-21.
Melmed S, Casanueva FF, Hoffman AR, Kleinberg DL, Montori VM, Schlechte JA, Wass JA; Endocrine Society. Diagnosis and treatment of hyperprolactinemia: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2011;96(2):273-288 (View)
FAQs from users: 'Can I get pregnant with high prolactin?', 'Do men also suffer from hyperprolactinemia?', 'Does Hyperprolactinemia make you gain weight?', 'Can hyperprolactinemia be cured?' and 'Can stress be a cause of hyperprolactinemia?'.
Authors and contributors




More information about Michelle Lorraine Embleton

Hey there. A few months ago I started to get milk leaking from my breasts and I am not pregnant. Could this be due to high prolactin levels? Thanks
Hello FionaLord
Galactorrhea, the term used for a milky discharge from the nipple that isn´t due to breastfeeding, is a fairly common symptom of hyperprolactinemia.
You should really consult an endocrinologist to have a hormone analysis and find out your the prolactin value. If your levels are too high and it is deemed necessary, the doctor will prescribe a treatment to restore the hormone values.
I hope I have helped you.
As with other issues that cause infertility, the important thing is to be able to uncover them as soon as possible in order to address the treatment that will lead to the restoration of fertility.
Hi, I had a miscarriage 1 month ago. I had an ultrasound and I have a cyst and left ovary with polycysts. They sent me to do a gynecological and hormonal profile, I only have high Prolactin. What’s the reason? I haven’t had my period yet.