The thyroid gland plays a very important role in female fertility, as it produces hormones that interact with the female sex hormones: estrogens and progesterone.
Therefore, thyroid hormones also play a role in regulating the menstrual cycle, follicular development and pregnancy, among other processes.
A malfunctioning thyroid gland can lead to metabolic imbalance, either because there is too much thyroid hormone (hyperthyroidism) or because too little thyroid hormone is produced (hypothyroidism). Both alterations can cause infertility, as well as lead to complications during pregnancy that could even end in abortion.
Provided below is an index with the 10 points we are going to expand on in this article.
- 1.
- 2.
- 2.1.
- 2.2.
- 3.
- 4.
- 5.
- 6.
- 6.1.
- 6.2.
- 6.3.
- 6.4.
- 6.5.
- 6.6.
- 6.7.
- 7.
- 8.
- 9.
- 10.
What is the thyroid gland for?
The thyroid is a butterfly-shaped gland located in the neck, just in front of the trachea.
Its main function is to act on all tissues of the body by regulating metabolism, through the production, storage and secretion of the following hormones:
- Thyroxine (T4)
- Triiodothyronine (T3)
Specifically, thyroid hormones regulate oxygen consumption, protein production, sensitivity to other hormones, and many other processes.
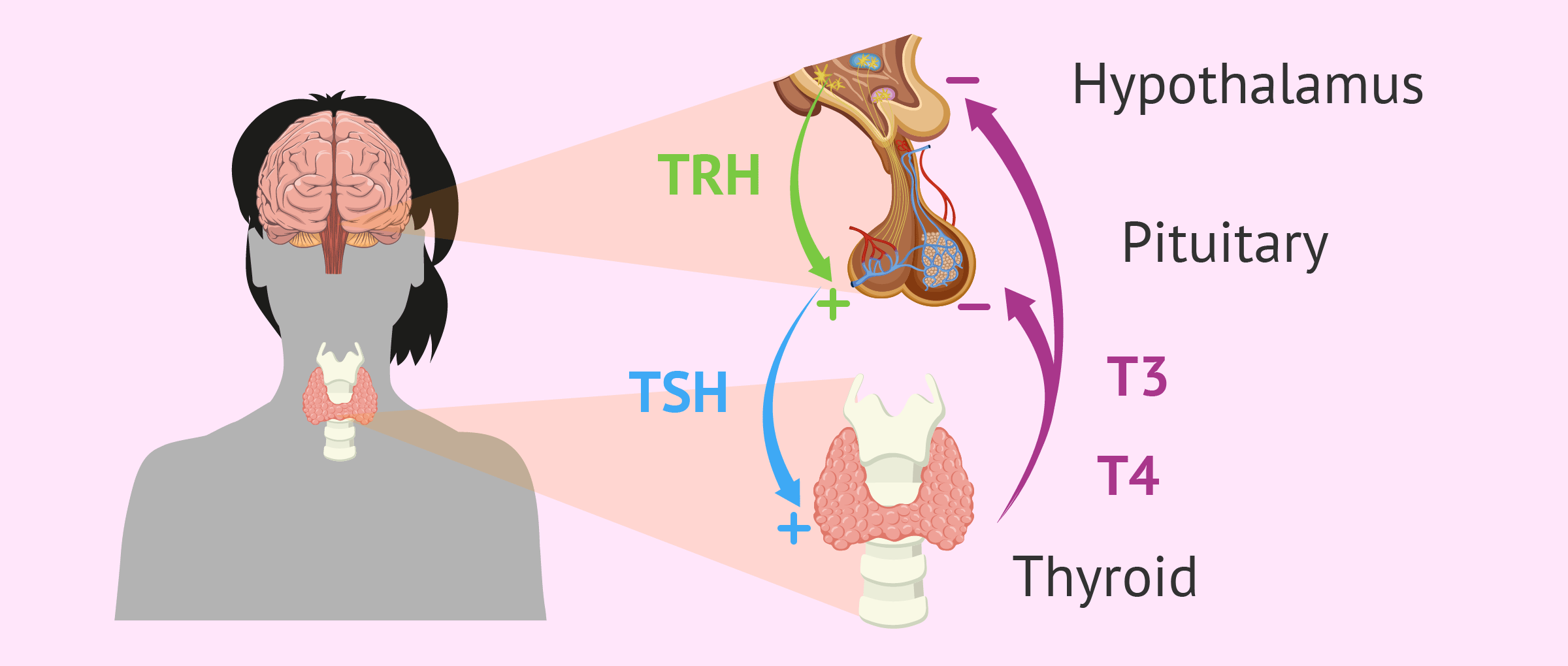
In turn, the production of thyroid hormones is regulated by TSH hormone, also called thyrotropin or thyroid-stimulating hormone, released by the pituitary gland in the brain.
Being a mother with thyroid disorders
Thyroid problems are considered an endocrine disease that affects any organ system of the body, including the reproductive system in women of childbearing age. When there is an alteration in the production of thyroid hormones, an imbalance of reproductive hormones occurs. The consequences of this are the following disorders related to women's fertility:
- Alteration of ovulation
- Irregular menstruation
- Infertility
- Risk of miscarriage

This is why thyroid hormone analysis is one of the first tests done when a woman has trouble getting pregnant. Thyroid alterations are classified into two major groups depending on the activity of the thyroid gland and the level of secreted hormones. These are discussed below:
Hyperthyroidism
It consists of the production and release of an excessive amount of thyroid hormones due to the hyperactivity of the thyroid gland. The consequence of this is an acceleration of the metabolism, with the appearance of the following symptoms:
- Increased heart rate
- Accelerated weight loss
- Excessive sweating
- Anxiety and nervousness
- Increased sensitivity to heat
- Irritability and insomnia
- Frequent bowel movements
- Trembling hands
- Muscle weakness
- Hair loss or breakage
- Irregular menstruation or total absence of menstrual cycles
The T3 and T4 hormones secreted by the thyroid in large amounts exert a feedback function on the brain and inhibit the production of TSH so that it stops stimulating the thyroid.
Hypothyroidism
In this case, the thyroid gland decreases in activity and, as a result, there is not enough production of thyroid hormones. Metabolism slows down, causing the following symptoms to appear:
- Decreased heart rate
- Weakness or fatigue
- Accelerated weight gain
- Low concentration and memory capacity
- Increased sensitivity to cold
- Muscle or joint pain
- Pale or dry skin
- Constipation
- Depression
- Hyperprolactinemia
- Irregular, lightly bleeding menstrual periods
- Anovulation

When the level of thyroid hormones decreases, the TSH released by the pituitary increases to try to maximize thyroid gland activity.
What are the causes of thyroid disorders?
There are many causes that can be responsible for the alteration of thyroid hormones. In general, malfunction of the thyroid gland itself or disorders of the hypothalamus and pituitary gland are the direct causes of these alterations.
As for hyperthyroidism, 70% of cases are caused by Graves' disease, in which antibodies are generated that stimulate thyroid growth and, as a consequence, there is an increase in the secretion of thyroid hormones. Other causes of hyperthyroidism include the following:
- Excess iodine diet
- Thyroiditis -inflammation of the thyroid
- Thyroid nodules or cysts
- Benign tumors in the pituitary gland

In relation to hypothyroidism, the most common cause is thyroiditis caused by an alteration of the immune system. This autoimmune disease is known as Hashimoto's thyroiditiswhich creates antibodies that attack the thyroid gland. Other causes of Hypothyroidism include the following:
- Surgery to remove the thyroid gland or part of it
- Radioactive therapies against cancer
- Drugs such as amiodarone and lithium
- Iodine-deficient diet
- Congenital defects

If you're interested in reading more about this topic, you can read on in the next post: Hypothyroidism
Diagnosis
First, it is important to pay attention to the signs and symptoms of hypothyroidism and hyperthyroidism in order to discuss them with the endocrinologist. It will also mesure blood pressure, weight, temperature, etc.
It is also necessary for the endocrinologist to evaluate the size of the thyroid gland by palpation of the neck to see if it is larger or smaller than normal.
Finally, a blood test to measure the level of TSH hormone is the most reliable test to diagnose thyroid problems.
The normal blood TSH value is in the range of 0.5 and 4.7 mU/ml.
Therefore, a TSH level greater than 4.7 mU/ml indicates insufficient production of thyroid hormones (hypothyroidism), while a TSH level less than 0.5 mU/ml confirms that the production of these hormones is excessive (hyperthyroidism). Occasionally, an ultrasound of the thyroid gland is recommended to rule out the presence of nodules or cysts.
Treatment
Once a dysfunction in the thyroid gland has been diagnosed, the treatment applied will depend on whether it is intended to increase or decrease its activity or hormone production:
- Hyperthyroidism
- administration of antithyroid medications to reduce the amount of T3 and T4 and relieve symptoms. In some cases, radioactive iodine is needed to destroy parts of the thyroid gland, or even surgery to remove it.
- Hypothyroidism
- administration of synthetic thyroid hormones such as levothyroxine (Eutirox). The doctor will indicate to take the drug in increasing doses until the metabolism and the correct functioning of the thyroid are stabilized.

After following the appropriate treatment, it is possible to restore the woman's ovarian cycle and have a natural pregnancy. It will also decrease the risk of miscarriage during the first trimester of gestation and associated fetal problems, as well as increase the patient's libido and mood.
If even with hormone regulation hormone levels are not balanced, it will be necessary to resort to assisted reproduction techniques to achieve pregnancy. In particular, in vitro fertilization (IVF) offers the best results.
Once the pregnancy is achieved, the woman will have to go periodically to the specialist to monitor the thyroid gland and thus keep hormone levels under control.
FAQs from users
Can I get a hysterosalpingogram if I have hyperthyroidism?
Hysterosalpingography is a gynecological imaging study that is performed with an iodinated contrast substance, so the administration of the same in patients with hyperthyroidism could complicate and aggravate this condition.
In these situations, a thorough study of thyroid function and a timely endocrinological consultation is recommended.
How is infertility treated in women with hypothyroidism?
Women who have hypothyroidism suffer from a slowdown in the production of hormones by the thyroid gland.
In these women, it is necessary, regardless of the technique used (fertilization in vitro, ovodonation), to correct with thyroid hormone (oral tablets) until a good TSH is obtained, below 2.5 (thyroid hormone) to guarantee that the implantation can be produced without problems.
This treatment will continue until pregnancy and it is important to make periodic controls with the endocrinologist to evaluate if it is necessary to increase or decrease the doses of the treatment.
How should the diet be to regulate thyroid problems?
The thyroid gland needs an adequate supply of iodine, selenium and vitamins for its proper functioning. Therefore, it will be necessary to eat a healthy and balanced diet to regulate the thyroid, based on fresh fruits and vegetables and fish rich in omega-3.
It is also very important to reduce the consumption of processed foods such as chips and soft drinks, as well as the intake of sugar.
What is subclinical hypothyroidism?
Subclinical hypothyroidism consists of a phase prior to common hypothyroidism in which the levels of T3 and T4 are still within normal, but with the TSH already elevated. This is due to the fact that the increase in TSH is sufficient to maintain the correct functioning of the thyroid gland and, therefore, the characteristic symptoms of this thyroid alteration are not yet manifested.
For this reason, it is necessary to analyze the value of TSH in blood when there are infertility problems without apparent cause.
Can I be a mother if I have hypergonadotropic hypogonadism?
The causes of hypergonadotropic hypogonadism are multiple and give rise to an alteration in ovarian function, conditioning fertility.
In general terms, we can state that the possibility of gestation will be determined by whether or not there is an ovarian follicular endowment and the integrity of the uterine factor. If both criteria are met, gestation would be possible through spontaneous gestation or Assisted Reproduction techniques (artificial insemination, in vitro fertilisation or gamete or embryo donation).
On the other hand, if there is no follicular endowment and uterine integrity is maintained, gestation through gamete or embryo donation would be possible.

It is important to underline that in cases where hypergonadotropic hypogonadism is associated with a genetic syndrome, Preimplantation Genetic Diagnosis is recommended in cases of in vitro fertilisation.
Do thyroid problems also cause male infertility?
Yes, although it is not as common as in women. Thyroid alterations influence the production and maturation of sperm, are a cause of teratozoospermia and can also cause erectile dysfunction and decreased libido.
Does hyperthyroidism affect sperm morphology?
Elevated thyroid hormone levels can affect sperm maturation and formation (spermatogenesis) and sperm quality. In addition, the concentration of available free testosterone is reduced, increasing problems with sexual intercourse, e.g. premature ejaculation.
Read more
Suggested for you
In addition to thyroid hormones, fertility tests include analysis of all the hormones that act on a woman's menstrual cycle. We recommend you read the following post for more information about this: Female Hormone Check – How Are Hormone Levels Monitored?.
If you need to do an assisted reproduction treatment such as IVF and need information, you can enter the following post to follow the reading: What Is In Vitro Fertilization (IVF)? – Process, Cost & Success Rates
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Alban Deroux, Chantal Dumestre-Perard, Camille Dunand-Faure, Laurence Bouillet, Pascale Hoffmann. Female Infertility and Serum Auto-antibodies: a Systematic Review. Clin Rev Allergy Immunol. 2017 Aug;53(1):78-86. doi: 10.1007/s12016-016-8586-z (View)
David Unuane, Brigitte Velkeniers. Impact of thyroid disease on fertility and assisted conception. Best Pract Res Clin Endocrinol Metab. 2020 Jul;34(4):101378. doi: 10.1016/j.beem.2020.101378. Epub 2020 Jan 30 (View)
David Unuane, Herman Tournaye, Brigitte Velkeniers, Kris Poppe. Endocrine disorders & female infertility. Best Pract Res Clin Endocrinol Metab. 2011 Dec;25(6):861-73. doi: 10.1016/j.beem.2011.08.001 (View)
G E Krassas, K Poppe, D Glinoer. Thyroid function and human reproductive health. Endocr Rev. 2010 Oct;31(5):702-55. doi: 10.1210/er.2009-0041. Epub 2010 Jun 23 (View)
S Medenica, O Nedeljkovic, N Radojevic, M Stojkovic, B Trbojevic, B Pajovic. Thyroid dysfunction and thyroid autoimmunity in euthyroid women in achieving fertility. Eur Rev Med Pharmacol Sci
. 2015;19(6):977-87 (View)
FAQs from users: 'Can I get a hysterosalpingogram if I have hyperthyroidism?', 'How is infertility treated in women with hypothyroidism?', 'How should the diet be to regulate thyroid problems?', 'What is subclinical hypothyroidism?', 'Can I be a mother if I have hypergonadotropic hypogonadism?', 'Do thyroid problems also cause male infertility?' and 'Does hyperthyroidism affect sperm morphology?'.
Authors and contributors







