Morris syndrome, also known as Androgen Insensitivity Syndrome (AIS) or testicular feminisation syndrome, is a genetic alteration that affects an individual's sexual development.
Specifically, the person is born with a male genetic sex (XY), but his development and physical appearance is female. For this reason, Morris syndrome is also said to be a type of male pseudohermaphroditism.
People with AIS have female sexual characteristics and are therefore considered to be women. However, they do not have a uterus or ovaries, and they discover that they suffer from this genetic alteration due to the absence of menstruation when they reach puberty. As a consequence of this, these women will also be sterile.
Provided below is an index with the 9 points we are going to expand on in this article.
- 1.
- 2.
- 3.
- 4.
- 5.
- 5.1.
- 5.2.
- 5.3.
- 5.4.
- 5.5.
- 6.
- 7.
- 8.
- 9.
Causes
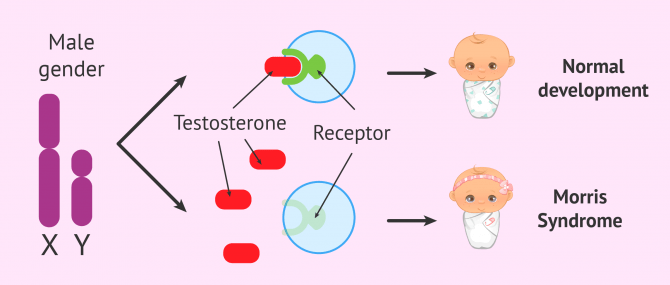
Morris syndrome is caused by a genetic mutation located on the X sex chromosome that affects the AR (androgen receptor) gene.
What happens is that there is no formation of androgen receptor proteins and, as a result, these male sex hormones cannot perform their function. The person is said to be resistant to androgens.
Androgens, and specifically the hormone testosterna, are responsible for sexual development in males. They intervene in the formation and descent of the testes, growth of the penis, appearance of hair, spermatogenesis, etc.
Women with Morris syndrome have similar blood testosterone levels to men. However, their body is not able to absorb it and, as a consequence, there is a feminine sexual development.
The genetic alteration that gives rise to AIS has two different origins:
- Inherited from mother
- is what happens in two-thirds of all cases. The mother carries the mutated gene on one of her X chromosomes, but does not have the disease because of its recessive nature. However, her children with XY genotype with only one copy of the altered gene will be affected.
- Spontaneous mutation in the ovum
- the alteration appears de novo at the time of ovum formation or during the early stages of embryo development.
Types of AIS
The severity of androgen insensitivity syndrome depends on the level of androgen receptor deficiency. Depending on the degree of insensitivity, the following types will exist:
- Incomplete AIS
- different levels of male and female traits may appear, e.g. undescended testes, clitoromegaly or micropenis, partial closure of the vagina, etc.
- Complete AIS
- corresponds to Morris syndrome itself. The external genitalia are female, as resistance to androgens is complete.
Complete AIS can also be called complete testicular feminization because it prevents the development of the penis and other male body organs.
Morris syndrome can occur in one in 20,000 to 64,000 male newborns. This prevalence could be even higher if undiagnosed cases are counted.
Features of the complete AIS
People with genotype 46,XY who suffer from Morris syndrome have an apparently feminine sexual development, but with some peculiarities.
The resistance of the fetus to the action of androgens during embryogenesis prevents the complete formation of the male reproductive system. However, there are testicles because their formation depends on the SRY gene present in the Y chromosome.
On the other hand, the external genitals develop as if the male hormones did not exist, with an aspect equal or very similar to those of a woman: vagina, vulva, breasts...
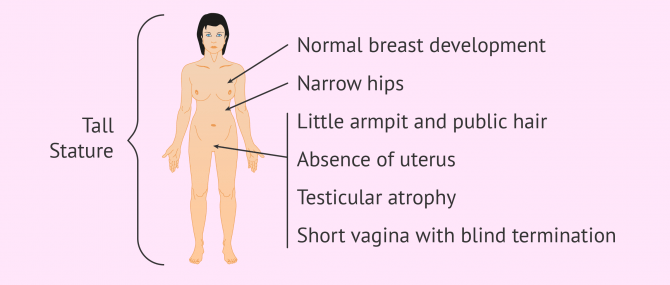
In general, no symptom of AIS is suspected during these girls' childhood. However, once puberty is reached, the lack of menarche (first period) makes one suspect that something is not right. Other characteristics and physical features of Morris syndrome include the following:
- Little armpit and pubic hair.
- The labia majora and labia minora of the female genitals may be smaller.
- Short vagina with blind termination.
- Absence of uterus, fallopian tubes and ovaries.
- Undescended atrophied testicles, in the groin region, abdomen, or labia majora.
- Normal breast development
- Narrow hips and tall stature.
- Decreased bone density.
Treatment
Nowadays, there is no effective treatment to correct the deficit of androgen receptors and that the male gender can express itself.
However, there are some interventions that can help these people lead as normal a life as possible. These are discussed below:
- Dilation of the vagina
- in the case of a very small vagina, it is possible to use vaginal dilators once the woman has reached puberty, in order to be able to have sex without pain.
- Vaginal plastic surgery
- in case of a very small vagina and cannot use dilators.
- Gonadectomy
- removal of undescended testicles to prevent the development of malignant tumors such as gonadoblastoma. It should be noted that this surgery cannot be performed until the girl finishes developing and goes through puberty.
- Calcium and vitamin D supplements
- to treat the lack of bone density in these patients. Exercise is also recommended.
- Psychological assistance
- in patients who may be greatly affected by the diagnosis and suffer dissatisfaction with their own body. Also to accept the fact that the woman will not be able to have a biological child due to sterility.

FAQs from users
What is the sexual identity of a person with Morris syndrome?
Although these people have a typical male genotype, with X and Y sex chromosomes, they are physically women and have been raised and identified as such since birth.
Normally, female identity persists in these people after diagnosis and for the rest of their lives. However, it can also happen that there is a change of identity and that the person is identified as a man.
How is Morris syndrome diagnosed?
The easiest way to confirm that a woman suffers from this type of pseudohermaphroditism is through a blood test and the study of the karyotype to see the chromosomes. On the other hand, by means of a hormonal analysis a high level of androgens, typical of the male sex, will also be observed.
What is a gonadoblastoma?
A gonadoblastoma is a very rare type of tumor, formed by a combination of germinal cells and sex-estromous cords, which is found exclusively in patients with some gonadal dysgenesis, as is the case of Morris syndrome.
To prevent the development of this type of tumour in women with AIS who have atrophied testicles, it is advisable to remove them as soon as possible after puberty.
Atrophied testicles may be noted by palpation in the groin or lower abdomen, and may also result in inguinal hernias.
Can people with Morris syndrome have children?
Since they do not have a uterus or ovaries, these women cannot have a pregnancy or a biological child. Their reproductive options to become mothers will be adoption or surrogacy with egg donation.
If you are interested in more information about surrogacy, we recommend you visit the following post: What Is Surrogacy? – Definition & Types.
Which celebrities have been associated with Morris syndrome?
Throughout history, there have been several legends that claim that some historical characters suffered from Morris syndrome, as are the cases of Joan of Arc or Queen Elizabeth I of England.
Also today, there are still unconfirmed rumors of some famous women with Morris syndrome, such as the spanish presenter Anne Igartiburu, or Hollywood actresses Nicole Kidman and Charlize Theron.
Suggested for you
Morris syndrome is an inherited X-linked disorder and could therefore be avoided by preimplantation genetic diagnosis (PGD) of embryos during assisted reproductive treatment. If you want to know what it is, we invite you to read the following post: What Is PGD or Preimplantation Genetic Diagnosis?
On the other hand, if you want to consult some of the diagnostic tests that can be done on these women, you can continue reading here: Female Fertility Tests – How Do You Know if You Can’t Get Pregnant?
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Author


Find the latest news on assisted reproduction in our channels.
