Beckwith Wiedemann Syndrome (BWS) is a congenital disease that appears from birth. The main characteristics of this disorder are excessive body growth, presence of omphalocele and bulging tongue, among others. In addition, BWS is highly predisposed to develop tumors during childhood.
The causes of Beckwith Wiedemann syndrome are genetic or epigenetic, related to a defect in a region of chromosome 11. In addition, most cases of BWS are spontaneous and not transmitted by their parents.
Provided below is an index with the 9 points we are going to expand on in this article.
- 1.
- 1.1.
- 2.
- 3.
- 4.
- 5.
- 5.1.
- 5.2.
- 5.3.
- 6.
- 7.
- 8.
- 9.
What is Beckwith Wiedemann Syndrome?
Beckwith Wiedemann Syndrome (BWS) is a rare genetic disease with which some babies are born and which is characterized by exaggerated growth. In addition, patients with this congenital disorder are more prone to develop tumors and malformations from birth. However, intellectual and physical development in the vast majority of people with BWS is normal.
Beckwith Wiedemann syndrome owes its name to the two doctors who described this disorder at the same time in 1960: Beckwith and Wiedemann
As for the manifestation of this syndrome, not all people with BWS have the same. Many babies suffer from macrosomia, omphalocele, etc. In addition, the breastfeeding period is a critical time for these infants, as BWS could cause low blood sugar levels.
In any case, infants diagnosed with BWS who survive the breastfeeding period have a good prognosis. Despite this, there is still a long way to go and much research remains to be done to learn more about the evolution of this disease.
Symptoms of BWS
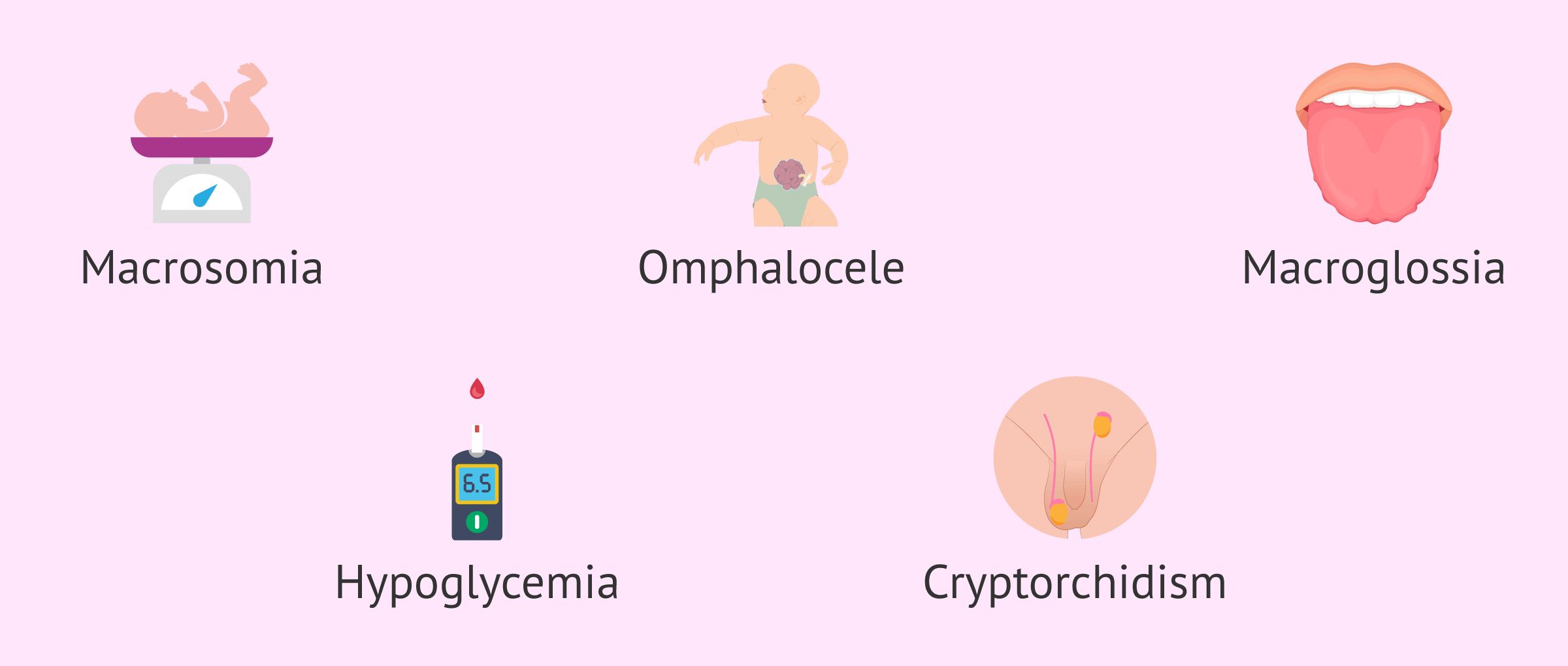
The signs and symptoms of Beckwith Wiedemann syndrome are highly variable from baby to baby, i.e. there is no set pattern of symptoms.
The most common clinical manifestations of BWS are listed below:
- High birth weight, macrosomia.
- Larger organs, visceromegaly.
- Abdominal defects, presence of umbilical hernia or omphalocele.
- Alterations in the external ear and grooves in the auricular lobe.
- Large eyes.
- Large size of tongue (macroglossia), sometimes protruded.
- Hypoglycemia, low blood sugar level
- Seizures and muscle spasms
- Cryptorchidism.
Another sign of Beckwith Wiedemann syndrome is a red birthmark appearing on the forehead or eyelids. This reddish mark is called Nevus flammeus. However, this symptom, as well as findings of polyhydramnios and prematurity during pregnancy, are less common.
Causes of Beckwith Wiedemann Syndrome
The etiology of Beckwith Wiedemann syndrome lies in a defect in gene expression. Specifically, BWS is caused by an alteration of genes located on chromosome 11.
Among the different genetic abnormalities that cause BWS are methylation errors or microdeletions in the DMR1 or DMR2 genes and maternally inherited mutations in the CDKN1C gene. In addition, certain chromosomal abnormalities, such as duplication of chromosome 11p15, translocation or inversion of maternal chromosome 11 could also induce BWS.
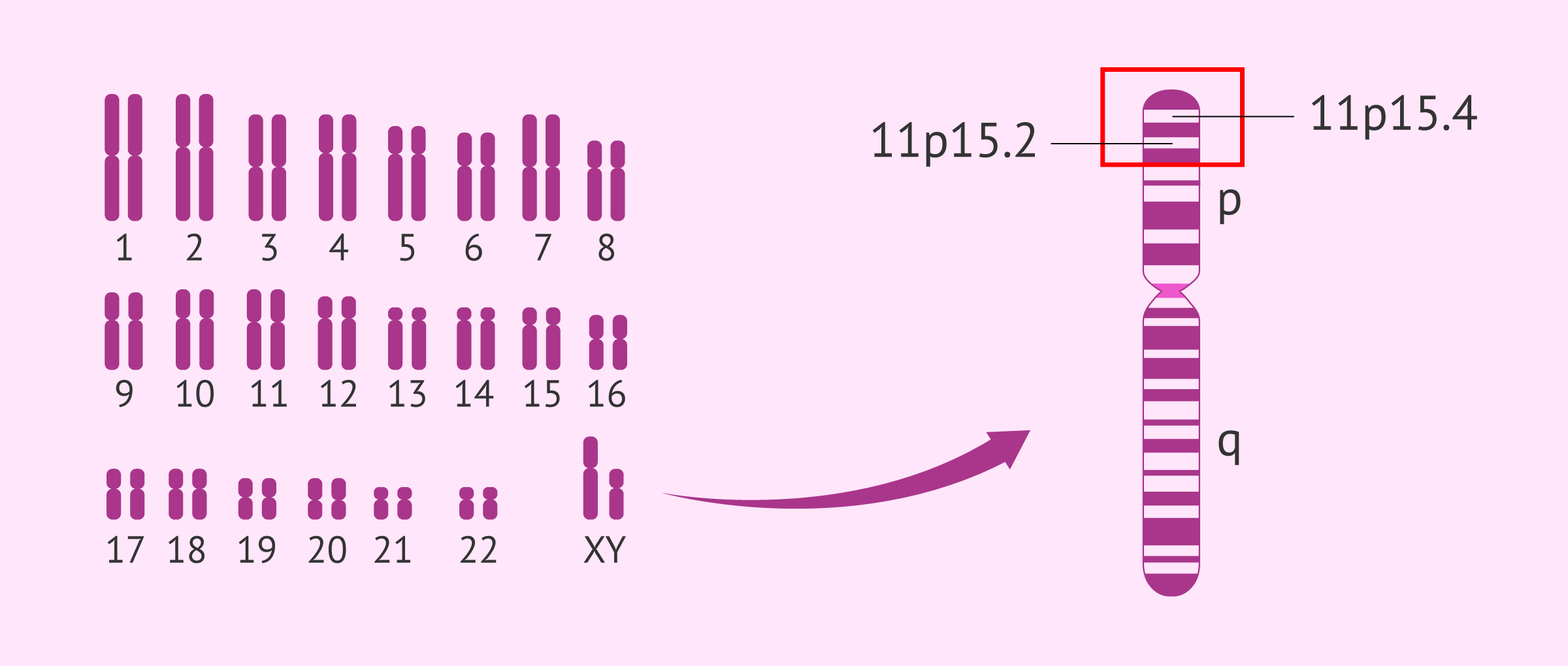
Another possible cause of Beckwith-Wiedemann syndrome could be paternal uniparental disomy of the region 15 of the short arm of chromosome 11, i.e. 11p15. This means that both copies of chromosome 11 come from the father and neither from the mother.
Approximately 85% of BWS cases occur spontaneously, but the remaining 15% are due to genetic transmission from parent to child.
How is BWS diagnosed?
Currently, there is no agreement on the clinical criteria for the diagnosis of Beckwith Wiedemann syndrome. Most specialists rely on the presence of symptoms such as omphalocele and macroglossia.
If the clinical examination leads the physician to suspect a possible case of Beckwith Wiedemann Syndrome, he/she will proceed to perform different tests for confirmation:
- Karyotyping: a blood sample will be taken from the baby to study its chromosome set. If it were indeed BWS, abnormalities in chromosome 11 would be detected.
- Molecular tests: would help to know the affected gene and the type of mutation. Most cases of BWS are caused by mutations in the CDKN1C gene.

Although these tests confirm the diagnosis of BWS, a negative molecular test result does not mean that the baby does not have BWS.
Treatment
Infants with hypoglycemia are treated through an intravenous line. In addition, during the first years of life, follow-up is necessary to prevent the development of tumors. Early diagnosis of cancer increases the survival rate of these patients.
Those children with BWS who have kidney problems or hemihypertrophy are 4 times more likely to develop a tumor, with 2 years being the average age at which most infants with BWS will develop a tumor.
On the other hand, macroglossia does not usually require surgical intervention. Only those tongues that, due to their excessive size, cause difficulty for the baby to breathe or eat will be opted for surgery.
FAQs from users
Do adults with Beckwith Wiedemann Syndrome have fertility problems?
Beckwith-Wiedemann syndrome (BWS) is a rare genetic disorder that affects the growth and development of various organs and tissues in the body. It can present with a variety of clinical features and medical conditions, but a direct association between BWS and fertility problems in adults has not been established.
It is important to note that BWS is usually diagnosed in infancy because of obvious clinical features, such as macrosomia (excessive growth at birth), enlarged internal organs, or abnormalities in organ development, such as the tongue or kidneys. Most studies and medical care focus on early diagnosis and treatment of children with BWS.
Because BWS is a disorder of growth and development, it is uncommon for fertility problems to be a major or well-established feature of this syndrome. However, each person with BWS may have a unique clinical presentation, and some may experience fertility-related health problems as a result of other medical complications associated with the syndrome.
If an adult with BWS has concerns or questions about his or her fertility, it is important to consult a physician or medical geneticist for personalized evaluation and counseling. Medical care and genetic counseling can help address specific fertility-related concerns in the context of BWS.
What is the life expectancy of children with Beckwith Wiedemann Syndrome?
Generally, Beckwith-Wiedemann Syndrome (BWS) does not affect the life expectancy and quality of life of people who suffer from it. However, a correct medical control is important, since there is a greater predisposition to develop tumors.
However, when patients reach the adolescent stage, growth becomes more normal. In addition, the risk of suffering cancer decreases with advancing age.
What complications arise from Beckwith Wiedemann Syndrome?
Beckwith Wiedemann syndrome is fully compatible with life, as it is not a fatal disease. However, this genetic disease increases the risk of developing a tumor. Therefore, this predisposition to cancer would be one of the possible consequences and complications of Beckwith Wiedemann syndrome.
Other complications derived from this disorder are anomalies in feeding or breathing, since the child has a rather large tongue. In addition, the child's spine may be laterally deviated (scoliosis) if one side of the body grows more than the other.
Suggested for you
One way to diagnose BWS before birth would be through prenatal studies. If you want to learn more about this, you can visit the following link: Invasive and non-invasive prenatal diagnostic techniques.
Another alternative to detect chromosomal alterations in embryos is through preimplantation genetic diagnosis in patients who resort to pregnancy through IVF. If you are interested in this topic, you can continue reading the following article: What genetic or chromosomal diseases can PGD detect?
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Francisco Cammarata-Scalisi, Andrea Avendaño, Frances Stock, Michele Callea, Angela Sparago, Andrea Riccio. Beckwith-Wiedemann syndrome: clinical and etiopathogenic aspects of a model genomic imprinting entity. Arch Argent Pediatr. 2018 Oct 1;116(5):368-373. doi: 10.5546/aap.2018.eng.368 (View)
Frédéric Brioude, Jennifer M Kalish, Alessandro Mussa, Alison C Foster, Jet Bliek, Giovanni Battista Ferrero, Susanne E Boonen, Trevor Cole, Robert Baker, Monica Bertoletti, Guido Cocchi, Carole Coze, Maurizio De Pellegrin, Khalid Hussain, Abdulla Ibrahim, Mark D Kilby, Malgorzata Krajewska-Walasek, Christian P Kratz, Edmund J Ladusans, Pablo Lapunzina, Yves Le Bouc, Saskia M Maas, Fiona Macdonald, Katrin Õunap, Licia Peruzzi, Sylvie Rossignol, Silvia Russo, Caroleen Shipster, Agata Skórka, Katrina Tatton-Brown, Jair Tenorio, Chiara Tortora, Karen Grønskov, Irène Netchine, Raoul C Hennekam, Dirk Prawitt, Zeynep Tümer, Thomas Eggermann, Deborah J G Mackay, Andrea Riccio, Eamonn R Maher. Expert consensus document: Clinical and molecular diagnosis, screening and management of Beckwith-Wiedemann syndrome: an international consensus statement. Nat Rev Endocrinol. 2018 Apr;14(4):229-249. doi: 10.1038/nrendo.2017.166 (View)
Hela Sassi, Yasmina Elaribi, Houweyda Jilani, Imen Rejeb, Syrine Hizem, Molka Sebai, Nadia Kasdallah, Habib Bouthour, Samia Hannachi, Jasmin Beygo, Ali Saad, Karin Buiting, Dorra H'mida Ben-Brahim, Lamia BenJemaa. Beckwith-Wiedemann syndrome: Clinical, histopathological and molecular study of two Tunisian patients and review of literature. Mol Genet Genomic Med. 2021 Oct;9(10):e1796. doi: 10.1002/mgg3.1796 (View)
Hidenobu Soejima, Satoshi Hara, Takashi Ohba, Ken Higashimoto. Placental Mesenchymal Dysplasia and Beckwith-Wiedemann Syndrome. Cancers (Basel). 2022 Nov 12;14(22):5563. doi: 10.3390/cancers14225563 (View)
Kathleen H Wang, Jonida Kupa, Kelly A Duffy, Jennifer M Kalish. Diagnosis and Management of Beckwith-Wiedemann Syndrome. Front Pediatr. 2020 Jan 21;7:562. doi: 10.3389/fped.2019.00562. eCollection 2019 (View)
Kelly A Duffy, Christopher M Cielo, Jennifer L Cohen, Christina X Gonzalez-Gandolfi, Jessica R Griff, Evan R Hathaway, Jonida Kupa, Jesse A Taylor, Kathleen H Wang, Arupa Ganguly, Matthew A Deardorff, Jennifer M Kalish. Characterization of the Beckwith-Wiedemann spectrum: Diagnosis and management. Am J Med Genet C Semin Med Genet. 2019 Dec;181(4):693-708. doi: 10.1002/ajmg.c.31740
Laura Fontana, Silvia Tabano, Silvia Maitz, Patrizia Colapietro, Emanuele Garzia, Alberto Giovanni Gerli, Silvia Maria Sirchia, Monica Miozzo. Clinical and Molecular Diagnosis of Beckwith-Wiedemann Syndrome with Single- or Multi-Locus Imprinting Disturbance. Int J Mol Sci. 2021 Mar 26;22(7):3445. doi: 10.3390/ijms22073445 (View)
Thomas Eggermann, Eamonn R Maher, Christian P Kratz, Dirk Prawitt. Molecular Basis of Beckwith-Wiedemann Syndrome Spectrum with Associated Tumors and Consequences for Clinical Practice. Cancers (Basel). 2022 Jun 23;14(13):3083. doi: 10.3390/cancers14133083 (View)
FAQs from users: 'Do adults with Beckwith Wiedemann Syndrome have fertility problems?', 'What is the life expectancy of children with Beckwith Wiedemann Syndrome?' and 'What complications arise from Beckwith Wiedemann Syndrome?'.
Authors and contributors


Find the latest news on assisted reproduction in our channels.
