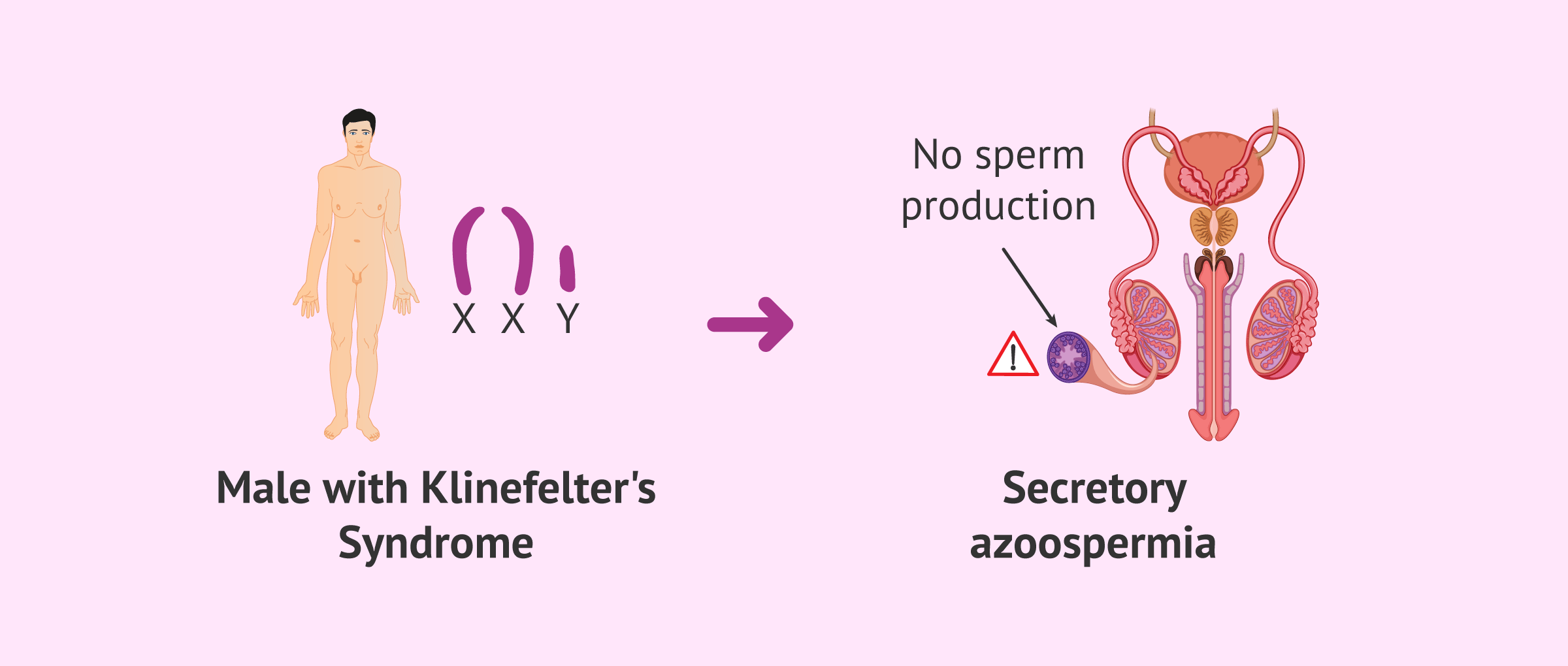
Klinefelter syndrome (KS), also known as XXY syndrome, is a genetic cause of male infertility. Children born with this genetic disease have an extra X chromosome, hence the name. Their karyotype is 47,XXY.
The effects of having an additional chromosome are abnormalities in the normal development of the body, hypogonadism, and male infertility.
However, some men affected with Klinefelter syndrome have become been able to have healthy children thanks to Assisted Reproductive Technologies (ART).
Provided below is an index with the 10 points we are going to expand on in this article.
- 1.
- 1.1.
- 2.
- 3.
- 4.
- 5.
- 5.1.
- 6.
- 6.1.
- 6.2.
- 6.3.
- 6.4.
- 6.5.
- 6.6.
- 7.
- 8.
- 9.
- 10.
What is Klinefelter syndrome?
Klinefelter or XXY syndrome is a genetic disease that causes babies to be born with an extra X chromosome. As a result, the baby has three sex chromosomes instead of 2, with male sex.
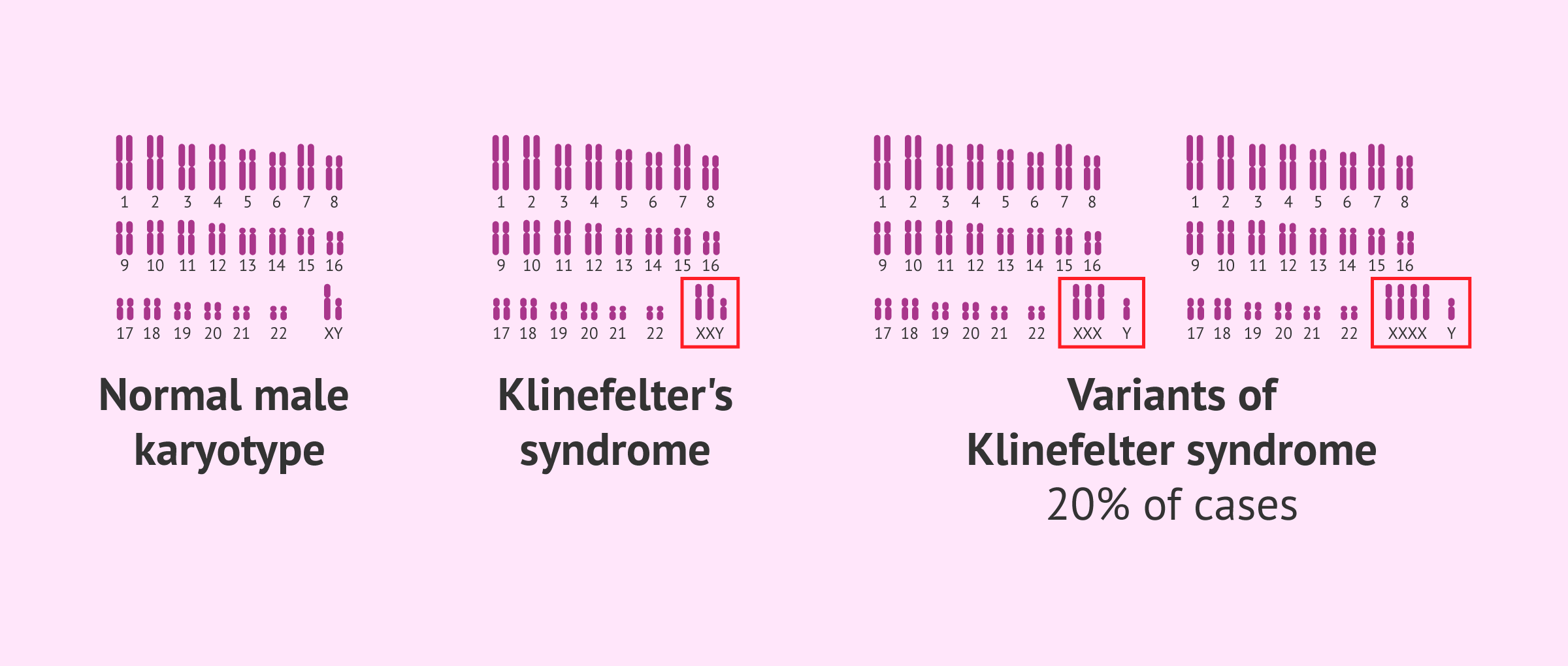
Even though the 47, XXY trisomy is the most common type, it is also possible to find males with abnormalities like 48,XXXY and 49,XXXXY in 20% of the cases approximately. It is estimated, however, that about 50% of the embryos with this chromosomal anomaly end up in miscarriage. The prevalence is 1 in every 1000 live births.
Phenotype of males
Signs and symptoms associated with children with Klinefelter syndrome start being noticeable during puberty, due to the absence of testosterone production. It is at this point when the male reproductive system and secondary male sex characteristics are supposed to develop.
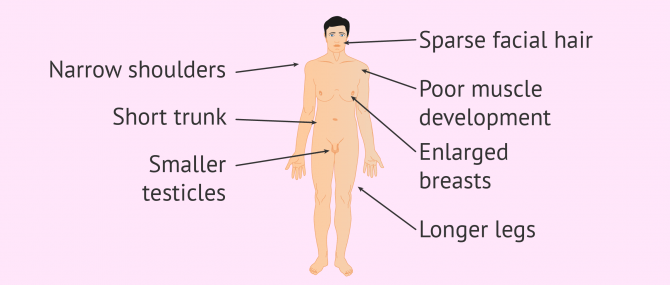
Even though the physical features may vary on a case-by-case basis, the following are the most common ones:
- Abnormal body proportions: too long legs, short trunk, shoulder equal to hip...
- Absent or sparse facial, body and sexual hair
- Poor muscle development
- Gynecomastia or enlarged male breasts
- Small or underdeveloped testes
- Other alterations of the male reproductive system: micropenis, cryptorchidism, absent vasa deferentia...
- Infertility due to azoospermia and diminished sex drive
Additionally, children affected with Klinefelter syndrome can develop psychological issues and behavioral problems. Although their IQ is generally normal, hyperactivity and attention-deficit disorder are usually associated with this chromosomal condition. Emotional disorders, depression, low self-confidence, etc. are common as well.
Causes of Klinefelter syndrome
The fact that an embryo grows with an extra X chromosome is due to an error at some point of the meiosis process during gametogenesis (egg and sperm formation) in the parents.
Meiosis is a cell division process that occurs in the egg cells of the ovaries, and the sperm cells of the testicles. The goal is to create haploid gametes, that is, to reduce the number of chromosomes in a parent diploid cell by half.
To be precise, Klinefelter syndrome can be caused by nondisjunction of a pair of chromosomes: X chromosomes do not separate during prophase of meiosis I in females.
The result is an imbalance in the total number of sex chromosomes: while some gametes will contain two sex chromosomes, other won't have any.
Depending on whether nondisjunction is associated with the father or the mother, we can distinguish two different case scenarios:
- Errors during oogenesis
- The eggs produced contain two X chromosomes instead of a single one.
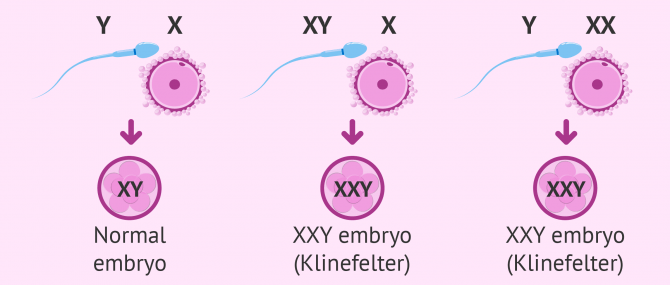
- Errors during spermatogenesis
- The sperms produced contain a X chromosome and a Y chromosome, instead of a single X or Y chromosome.
When fertilization occurs between an affected and a healthy chromosome, the result is a triploid embryo (47, XXY).
It should be noted, however, that Klinefelter syndrome is more often associated with errors during oogenesis than spermatogenesis.
Less frequently, this chromosomal condition may appear during the earliest embryo cleavage, right after fertilization. In this case, they are called mosaic embryos.
Mosaicism occurs when two cell populations with different genotypes are present within the same embryo. In other words, half are chromosomally healthy, and the other half has the XXY trisomy.
How is Klinefelter syndrome diagnosed?
In most cases, Klinefelter syndrome is diagnosed when the boy is a teenager, due to obvious phenotype and psychological traits.
When these signs and symptoms are not so noticeable, males find out about this chromosomal condition when they start trying to conceive and realize that they have azoospermia.
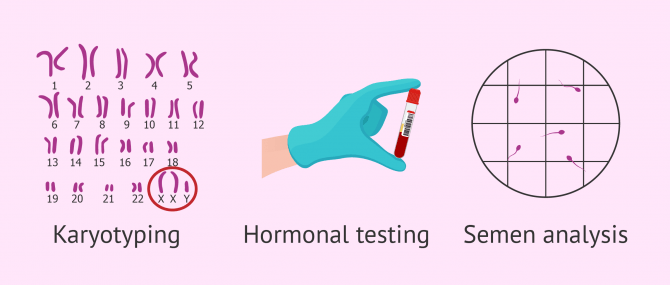
It is at this point when they visit a fertility specialist and undergo the following tests in order to determine whether they suffer from KS or not:
- Karyotype testing
- Study of the number of chromosomes to detect the presence of an extra X chromosome.
- Hormonal testing
- To detect potential alterations in sex hormones, such as too increases levels of FSH, and diminished levels of testosterone.
- Semen analysis report
- Zero sperm count due to azoospermia.
If not detected at this stage, Klinefelter syndrome may be detected during pregnancy after doing an amniocentesis or amnio test, or a chorionic biopsy.
KS and fertility
Klinefelter syndrome is the most common cause of non-obstructive or secretory azoospermia in males. Having zero sperm count in the ejaculate is due to problems during spermatogenesis in the testicles.
In spite of that, sometimes males affected by KS present a few sperms in the ejaculate, which could translate into an opportunity to have biological children. Unfortunately, these sperms may be aneuploid and the risk of passing the disease to offspring would be considerably high.
Also, the presence of this trisomy in embryos may be a cause of recurrent miscarriage as well. In certain cases, mosaicism has been found to be the cause of repeated miscarriages.
Based on the number of affected cells by KS, the chances of producing abnormal sperm cells, and subsequently causing miscarriage or the birth of an ill child, will be higher or lower.
Treatment
Given that the Klinefelter syndrome is a genetic disease, actually there is no effective treatment to cure it.
However, opting for a hormone replacement therapy with testosterone can help improve the physical symptoms associated with reduced levels of this hormone. For instance, to trigger hair growth, build body mass, improve libido, etc.
Fertility treatment options
As for the treatment options to have a child, men affected by KS have no alternative but to become parents through a fertility treatment.
Firstly, to try to find viable sperm cells in cases of azoospermia causes by KS, and secondly, to prevent that this chromosomal condition is inherited by offspring.
So, in short, there exist various fertility treatment options for these patients:
- Testicular biopsy & ICSI
- When the sperm count is zero, performing a testicular biopsy to retrieve and use them for an ICSI cycle is an option.
- Preimplantation Genetic Diagnosis (PGD)
- The goal is to evaluate the embryos genetically in order to dismiss those with chromosomal abnormalities and use the healthy ones for the transfer.
- Artificial insemination by donor (AID)
- In case no sperms are found or the patient doesn't want to run the risk of passing the disease to offspring, using donor sperm for IUI is an option.
If you need to undergo IVF to become a mother, we recommend that you generate your Fertility Report now. In 3 simple steps, it will show you a list of clinics that fit your preferences and meet our strict quality criteria. Moreover, you will receive a report via email with useful tips to visit a fertility clinic for the first time.
You may also enjoy some further information reading this: Using a Sperm Donor to Get Pregnant.
FAQs from users
Is pregnancy possible with Klinefelter syndrome?
This syndrome is characterized by a chromosomal abnormality in males in which there is an extra X chromosome. Normally, when we study the chromosomes in a man, we find 46, XY, but in these cases affected by Klinefelter syndrome, we find 47, XXY.
The physical consequences can be multiple, and if analytical studies are carried out, hormonal failure and sterility due to alteration in sperm production at the level of the testicles can be found.
Each case must be assessed individually. In some cases, sperm can be extracted directly from the testicles through a testicular biopsy. If this is the case, then an IVF treatment with microinjection of one spermatozoon into each egg (ICSI) must be performed, with the possibility of a genetic study of the embryos to check chromosomal normality.
Is Klinefelter syndrome a genetic disease?
Klinefelter syndrome or 47,XXY is a genetic abnormality that occurs as a consequence of an incorrect division of homologous chromosomes during meiosis, which give raise to the gametes of one of the parents. It can also occur during the first divisions of the zygote.
Males affected by it suffer from hypogonadotropic hypogonadism, gynecomastia, learning disabilities, and infertility. It is the most common genetic disease in males. Some men, however, do not have symptoms, and they don't know that they have this condition until they are adults and have infertility issues.
What is the lifespan of men with Klinefelter syndrome?
Lifespan of males affected by KS is almost the same as the rest of the population, with perhaps a difference of 2 to 3 years.
Males with Klinefelter syndrome can have a normal lifestyle, although they have a higher chance of suffering from other health problems, such as diabetes type 2, breast cancer, and autoimmune diseases such as lupus.
Does Klinefelter syndrome cause oligospermia?
Yes, in males with these genetic alteration, testicular development occurs at an slower growth rate than normal when they reach puberty. This causes an insufficient testosterone level and amount of sperm to be synthesized.
Is Klinefelter syndrome associated with homosexuality?
No, various studies have shown that there is no association between Klinefelter syndrome and homosexuality.
Can Klinefelter develop in females?
Babies born with genotype 47,XXY are born males, that is, they have the typical physical features of males, with a penis and testicles. This is due to the presence of the Y chromosome.
Suggested for you
Azoospermia is the main cause of infertility in males affected by KS. To learn more about this sperm disorder, read: What Is Azoospermia?
If you are interested in learning about the most common causes of male infertility nowadays, check this out: What Causes Male Infertility? – Symptoms, Treatment & Statistics.
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Daniel J Wattendorf, Maximilian Muenke. Klinefelter syndrome. Am Fam Physician. 2005 Dec 1;72(11):2259-62 (View)
Gary Butler, Umasuthan Srirangalingam, Jennie Faithfull, Philippa Sangster, Senthil Senniappan, Rod Mitchell. Klinefelter syndrome: going beyond the diagnosis. Arch Dis Child. 2023 Mar;108(3):166-171. doi: 10.1136/archdischild-2020-320831 (View)
M Bonomi, V Rochira, D Pasquali, G Balercia, E A Jannini, A Ferlin; Klinefelter ItaliaN Group (KING). Klinefelter syndrome (KS): genetics, clinical phenotype and hypogonadism. J Endocrinol Invest. 2017 Feb;40(2):123-134. doi: 10.1007/s40618-016-0541-6 (View)
Mercé Artigas López. SINDROME de KLINEFELTER (View)
Nicole Tartaglia, Natalie Ayari, Susan Howell, Cheryl D'Epagnier, Philip Zeitler. 48,XXYY, 48,XXXY and 49,XXXXY syndromes: not just variants of Klinefelter syndrome. Acta Paediatr. 2011 Jun;100(6):851-60. doi: 10.1111/j.1651-2227.2011.02235.x (View)
Priyanka Bearelly, Robert Oates. Recent advances in managing and understanding Klinefelter syndrome. F1000Res. 2019 Jan 28:8:F1000 Faculty Rev-112. doi: 10.12688/f1000research.16747.1 (View)
Rosália Sá, Luís Ferraz, Alberto Barros, Mário Sousa. The Klinefelter Syndrome and Testicular Sperm Retrieval Outcomes. Genes (Basel). 2023 Mar 4;14(3):647. doi: 10.3390/genes14030647 (View)
Wei Chen, Ming Zhu Bai, Yixia Yang, Di Sun, Sufang Wu, Jian Sun, Yu Wu, Youji Feng, Youheng Wei, Zijiang Chen, Zhenbo Zhang. ART strategies in Klinefelter syndrome. J Assist Reprod Genet. 2020 Sep;37(9):2053-2079. doi: 10.1007/s10815-020-01818-2 (View)
FAQs from users: 'Is pregnancy possible with Klinefelter syndrome?', 'Is Klinefelter syndrome a genetic disease?', 'What is the lifespan of men with Klinefelter syndrome?', 'Does Klinefelter syndrome cause oligospermia?', 'Is Klinefelter syndrome associated with homosexuality?' and 'Can Klinefelter develop in females?'.
Authors and contributors




