Sertoli syndrome is also known as Sertoli-cell-only (SCO) syndrome, germ cell aplasia or Del Castillo syndrome. It describes a disorder in which no germ cells are found in the seminiferous tubules and only Sertoli cells are present.
Men diagnosed with this syndrome do not produce spermatozoa, so they will present azoospermia, that is, the absence of spermatozoa in the ejaculate.
Therefore, patients with Sertoli syndrome have obvious difficulties in becoming parents naturally. This is why they need assisted reproduction techniques, on many occasions, resorting to a sperm donor.
Provided below is an index with the 7 points we are going to expand on in this article.
What are Sertoli cells?
Sertoli cells are cells present in the testicular seminiferous tubules. They line them and have a supportive function. Hence, Sertoli cells play an important role in the nutrition of germ cells and for spermatogenesis to occur properly. Spermatogenesis is the name given to the production of spermatozoa in the seminiferous tubules.
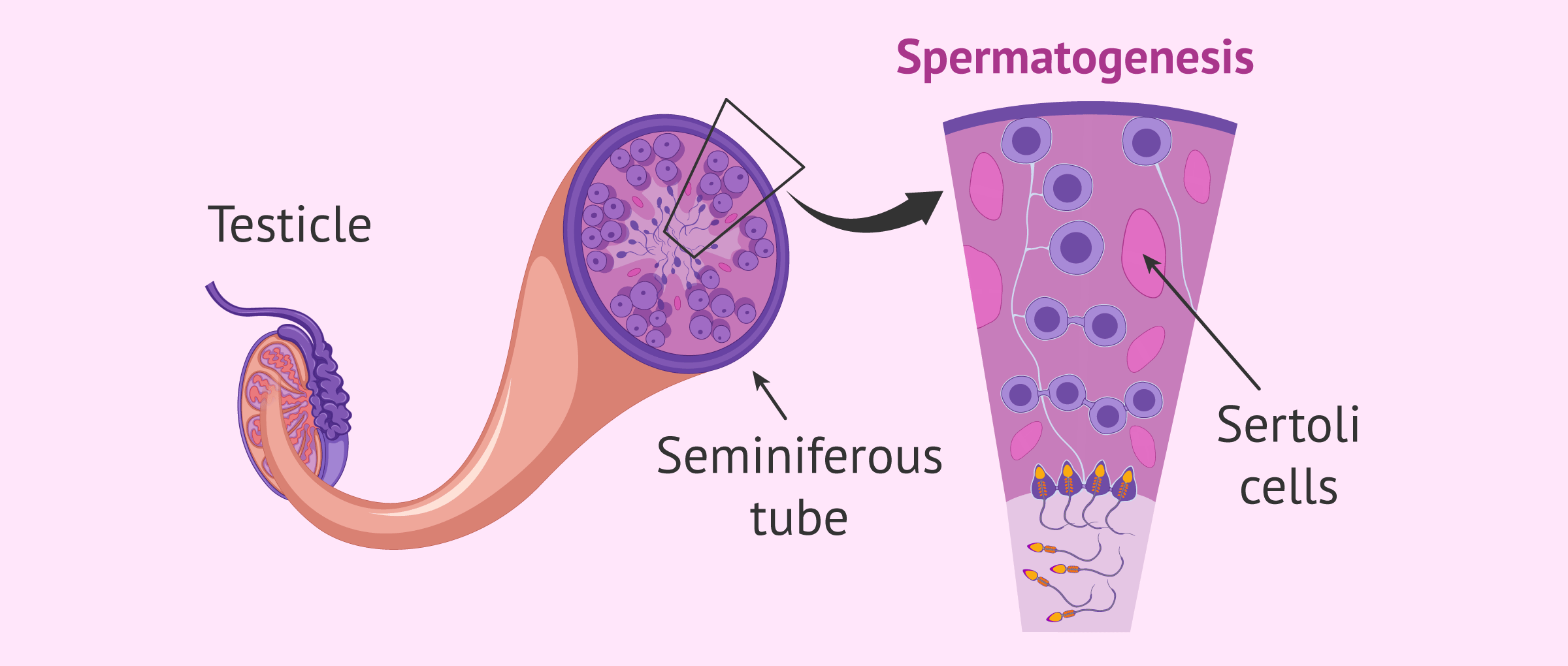
Therefore, under normal conditions, Sertoli cells coexist with germ cells in the seminiferous tubules.
Sertoli's syndrome
Patients affected by Sertoli syndrome only have Sertoli cells in the seminiferous tubules, and an absence of germ cells.
Usually, the physical examination of these males is normal, with normal secondary sexual characteristics (although the testicles may be smaller). Thus, germ cell aplasia is typically diagnosed when these patients attend a consultation for infertility problems.
If the seminogram shows a result of azoospermia, the diagnosis of Sertoli syndrome would be made by testicular biopsy and analysis of the tissue obtained.
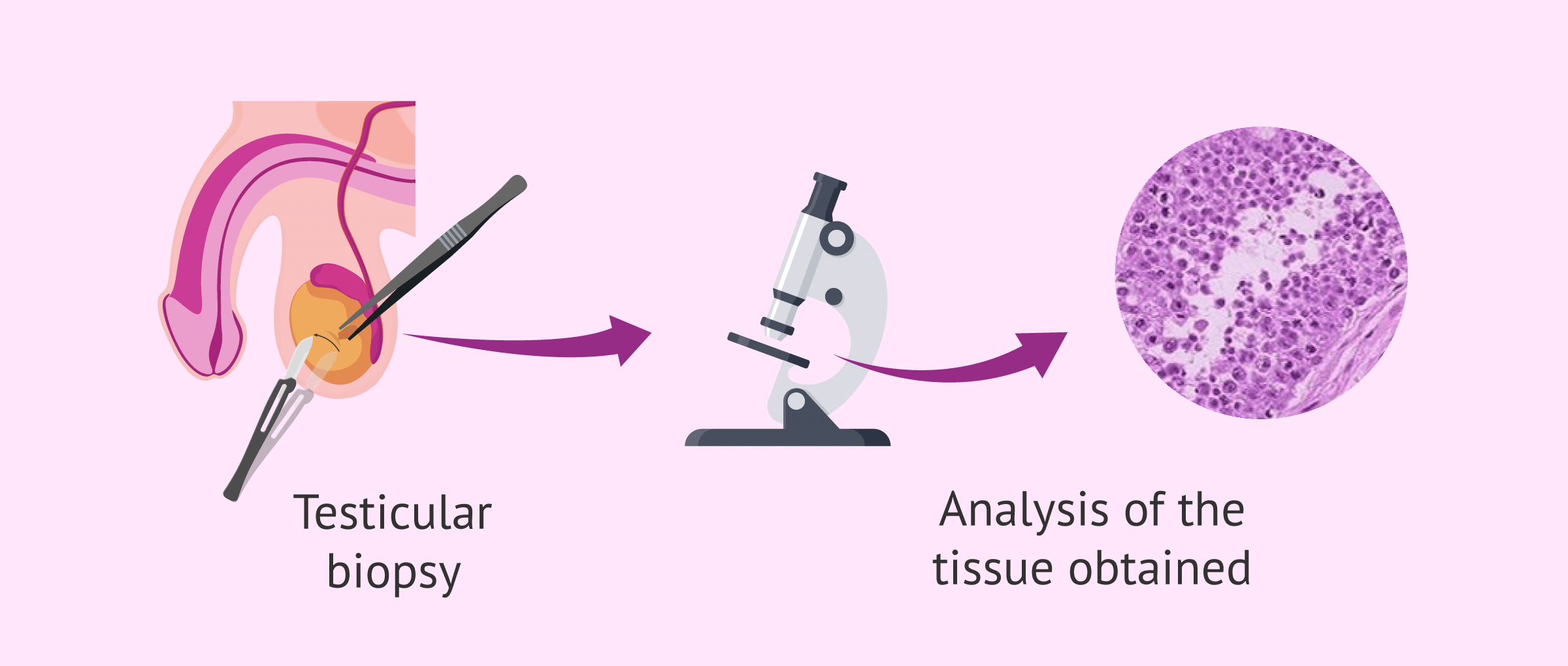
Among the clinical findings, many of the males affected with Sertoli syndrome may have a normal karyotype. Luteinizing hormone (LH) and testosterone levels are generally normal in these patients, while follicle-stimulating hormone (FSH) would be elevated.
Causes
One of the proposed causes of Sertoli syndrome is that the primordial germ cells did not successfully migrate to the primitive testis. In addition, genetic alterations, such as microdeletions of the Y chromosome, have been described as a possible cause. Sertoli syndrome has also been associated with Klinefelter syndrome.
However, the exact reasons for germ cell aplasia are often unknown.
In addition, there are other possible acquired causes associated with Sertoli syndrome. These include oncological treatments and viral infections.
Treatment
Unfortunately, there is no specific treatment for germ cell aplasia. For this reason, men diagnosed with Sertoli cell-only syndrome who wish to become fathers must resort to assisted reproduction.
These patients will not have sperm production and, therefore, it will not be possible to obtain spermatozoa in the ejaculate or in the testicles by biopsy. Because of this, patients with Sertoli syndrome cannot be biological parents.
Despite this, these patients can resort to sperm donation or adoption to have children.
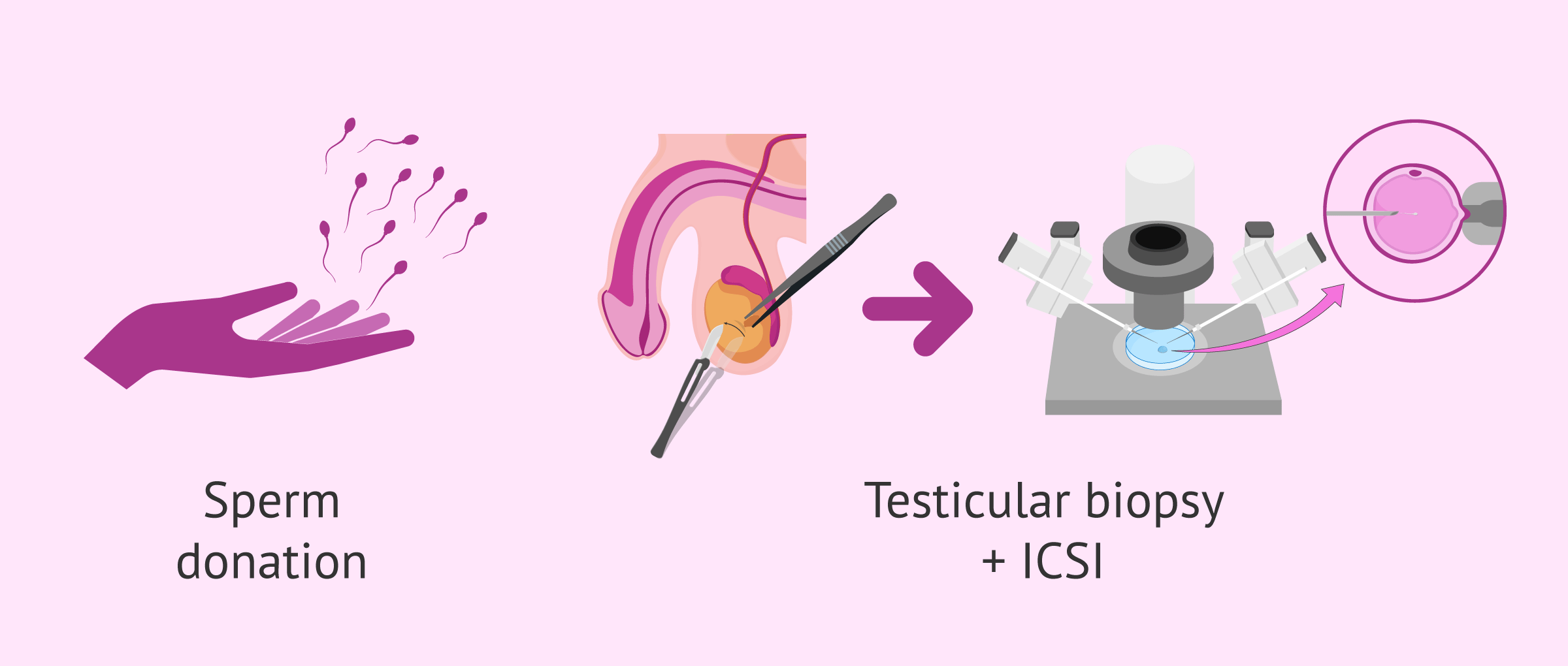
However, in some cases, some seminiferous tubules may be able to manage a small amount of spermatogenesis. This would make it possible to recover some sperm by testicular biopsy for later use in intracytoplasmic sperm injection (ICSI), which would allow them to become biological fathers.
In this case, it is essential to perform the necessary genetic tests and to offer genetic counseling to future parents, due to the risk that the baby may inherit some alteration.
Assisted procreation, as any other medical treatment, requires that you rely on the professionalism of the doctors and staff of the clinic you choose. Obviously, each clinic is different. Get now your Fertility Report, which will select several clinics for you out of the pool of clinics that meet our strict quality criteria. Moreover, it will offer you a comparison between the fees and conditions each clinic offers in order for you to make a well informed choice.
FAQs from users
What may be the cause of Sertoli syndrome?
Sertoli syndrome (germinal aplasia) consists of a testicular alteration characterized by not finding spermatogonia or spermatozoa (germ cells) at the level of the seminiferous tubule, only Sertoli cells (those whose mission is to provide structural and metabolic support to germ cells or future sperm cells). It is a cause of permanent and irreversible sterility. Since there are no spermatozoa in the testicle, it is not possible to resort to any assisted reproduction technique with the patient's own sperm, thus requiring donor sperm.
Among the fundamental causes of germinal aplasia (Sertoli syndrome), there are congenital or acquired causes: poor testicular descent, radiation, cytostatic drugs.
Can I be a father if I have Sertoli syndrome?
Sertoli syndrome patients have to resort to assisted reproductive techniques in order to become fathers and, in most cases, donor sperm must be used (so they will not be biological fathers).
However, in some men with Sertoli syndrome it is possible to obtain spermatozoa by testicular biopsy if a focus of spermatogenesis is preserved. These sperm can then be used to fertilize the eggs by intracytoplasmic sperm injection (ICSI) and thus attempt to achieve gestation.
Recommended reading
If you want to learn more about spermatogenesis, you can visit the following link: How spermatozoa are formed - Phases of spermatogenesis.
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Anniballo R, Ubaldi F, Cobellis L, Sorrentino M, Rienzi L, Greco E, Tesarik J. Criteria predicting the absence of spermatozoa in the Sertoli cell-only syndrome can be used to improve success rates of sperm retrieval. Hum Reprod. 2000 Nov;15(11):2269-77.
Behre HM, Bergmann M, Simoni M, Tüttelmann F. Primary Testicular Failure. 2015 Aug 30. In: Feingold KR, Anawalt B, Boyce A, Chrousos G, de Herder WW, Dungan K, Grossman A, Hershman JM, Hofland J, Kaltsas G, Koch C, Kopp P, Korbonits M, McLachlan R, Morley JE, New M, Purnell J, Singer F, Stratakis CA, Trence DL, Wilson DP, editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000–.
Foresta C, Ferlin A, Garolla A, Moro E, Pistorello M, Barbaux S, Rossato M. High frequency of well-defined Y-chromosome deletions in idiopathic Sertoli cell-only syndrome. Hum Reprod. 1998 Feb;13(2):302-7.
Franco G, Scarselli F, Casciani V, De Nunzio C, Dente D, Leonardo C, Greco PF, Greco A, Minasi MG, Greco E. A novel stepwise micro-TESE approach in non obstructive azoospermia. BMC Urol. 2016 May 12;16(1):20.
Ghanami Gashti N, Sadighi Gilani MA, Abbasi M. Sertoli cell-only syndrome: etiology and clinical management. J Assist Reprod Genet. 2021 Mar;38(3):559-572.
Gul U, Turunc T, Haydardedeoglu B, Yaycioglu O, Kuzgunbay B, Ozkardes H. Sperm retrieval and live birth rates in presumed Sertoli-cell-only syndrome in testis biopsy: a single centre experience. Andrology. 2013 Jan;1(1):47-51.
Ramphul K, Mejias SG. Sertoli-Cell-Only Syndrome. 2020 Sep 19. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan–.
Stouffs K, Gheldof A, Tournaye H, Vandermaelen D, Bonduelle M, Lissens W, Seneca S. Sertoli Cell-Only Syndrome: Behind the Genetic Scenes. Biomed Res Int. 2016;2016:6191307.
Yang Y, Ma MY, Xiao CY, Li L, Li SW, Zhang SZ. Massive deletion in AZFb/b+c and azoospermia with Sertoli cell only and/or maturation arrest. Int J Androl. 2008 Dec;31(6):573-8.
FAQs from users: 'What may be the cause of Sertoli syndrome?' and 'Can I be a father if I have Sertoli syndrome?'.
Authors and contributors



More information about Cristina Algarra Goosman

More information about Michelle Lorraine Embleton

Do you know what causes this syndrome? Is there any way to avoid it?
Hello Luisb,
The causes of this syndrome are not established, it is certain that there are some associated genetic alterations and some external factors that influence the presence of the syndrome such as radiation from cancer treatments.
I hope I have solved your doubt,
Best regards
Hi, my husband has Sertoli syndrome and I would like to know if it is impossible for him to be the genetic father of our children. If there was any possibility or something we can do…..
Hello Alexdr,
There are times when it is possible for a man with Sertoli Syndrome to have children. This will depend on sperm production.
The ICSI technique allows the fertilization of sperm, this will be extracted by a testicular biopsy of some morphologically and genetically correct sperm.
However, there are some couples who cannot obtain spermatozoa and therefore must resort to sperm donation.
I hope I have helped you,
Best regards