Hormonal alterations in women are one of the main causes of female sterility.
This is what is known as infertility of endocrine origin or ovarian factor, since what is ultimately affected in the woman's body is the functioning of the ovaries.
In general, this type of sterility includes all alterations of the hypothalamus-hypophysis-ovarian axis that imply a hormonal imbalance and, therefore, an alteration of the menstrual cycle.
Provided below is an index with the 12 points we are going to expand on in this article.
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 8.1.
- 8.2.
- 8.3.
- 9.
- 10.
- 11.
- 12.
Anovulation
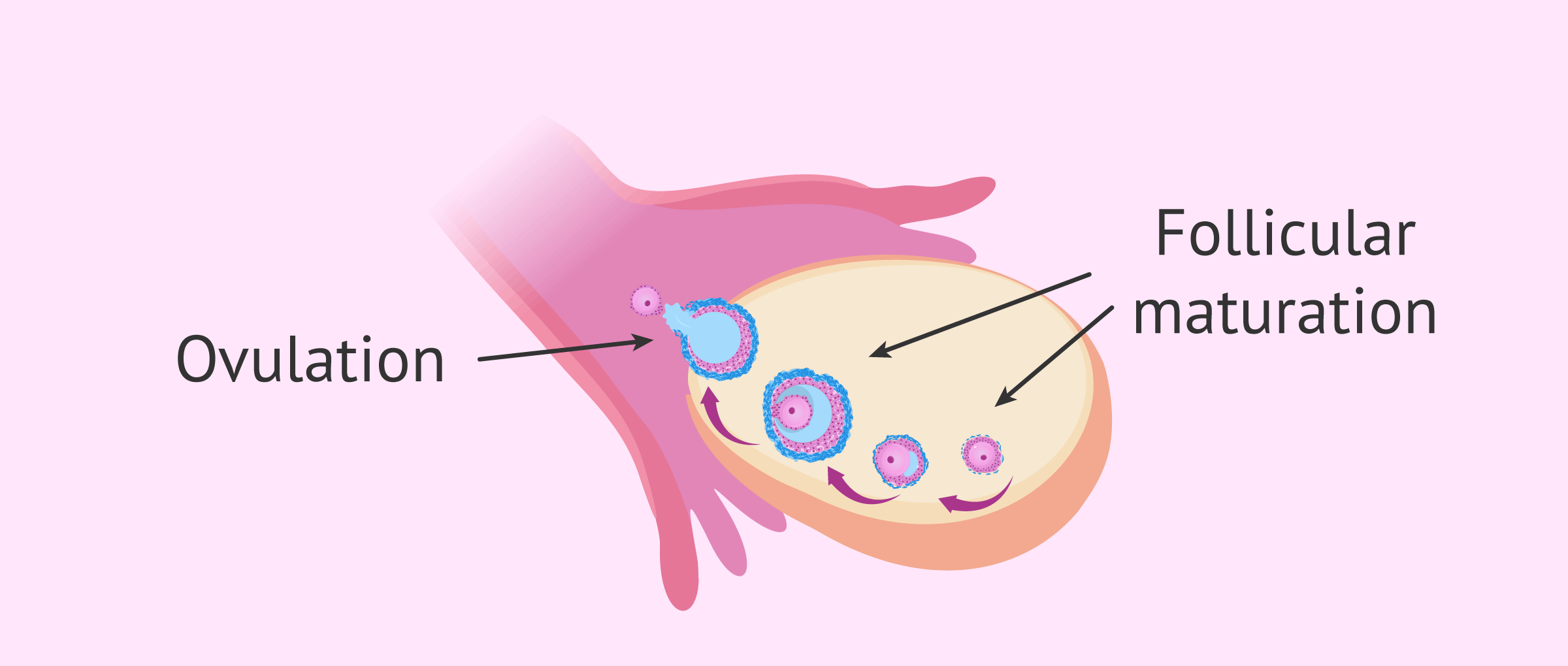
Anovulation consists of the absence of ovulation (expulsion of the mature egg from the ovary) in a menstrual cycle, so there will be no encounter of the egg with the sperm in the fallopian tube and fertilization will not occur.
Anovulatory cycles can be associated with a wide range of menstrual alterations and can be of two types:
- Sporadic anovulatory cycles
- the vast majority of women at some point in their lives have had a stage of anovulation due to periods of stress, anxiety, lack of food, etc.. In principle, this type of anovulation is neither worrying nor serious, as the ovulatory cycles will be restored.
- Chronic anovulatory cycles
- these women spend long periods of time without ovulation, so it is a cause of sterility. Without ovulation, the egg will never be able to join the sperm, form an embryo and result in pregnancy.
Prolonged or chronic anovulation may be caused by several factors that the World Health Organization (WHO) classifies into different groups:
- Group I
- hypothalamus and pituitary dysfunction. These include disorders such as hypogonadotropic hypogonadism, Kallman syndrome, etc.
- Group II
- alteration of hormonal secretion by the hypothalamus-hypophysis axis. This includes polycystic ovary syndrome (PCOS), hyperprolactinemia, etc.
- Group III
- primary and secondary ovarian insufficiency, which is also known as early menopause.

You can get more information about this in the following article: Anovulation- Symptoms and Treatment.
Polycystic ovary syndrome (PCOS)
PCOS is the most common endocrine disruption in infertile women.
These women have ovaries full of cysts corresponding to the ovarian follicles that do not develop, so there is no ovulation.
In addition, the level of estrogens and androgens is also altered and, as a consequence, these women show signs of masculinization, amenorrhea, insulin resistance, obesity, etc.

For more detailed information on this syndrome, we encourage you to read on here: What is PCOS?
Hyperprolactinemia
Hyperprolactinemia is the excessive production of the hormone prolactin, which is secreted by the pituitary gland and has the function of stimulating the production of breast milk after delivery.
Too much prolactin inhibits the functioning of the hypothalamus, so that the hormones regulating the menstrual cycle are not secreted and the woman also suffers anovulation.

For more information on the causes and treatment of hyperprolactinemia, we recommend the following post: What is hyperprolactinemia?
Premature ovarian failure (POF)
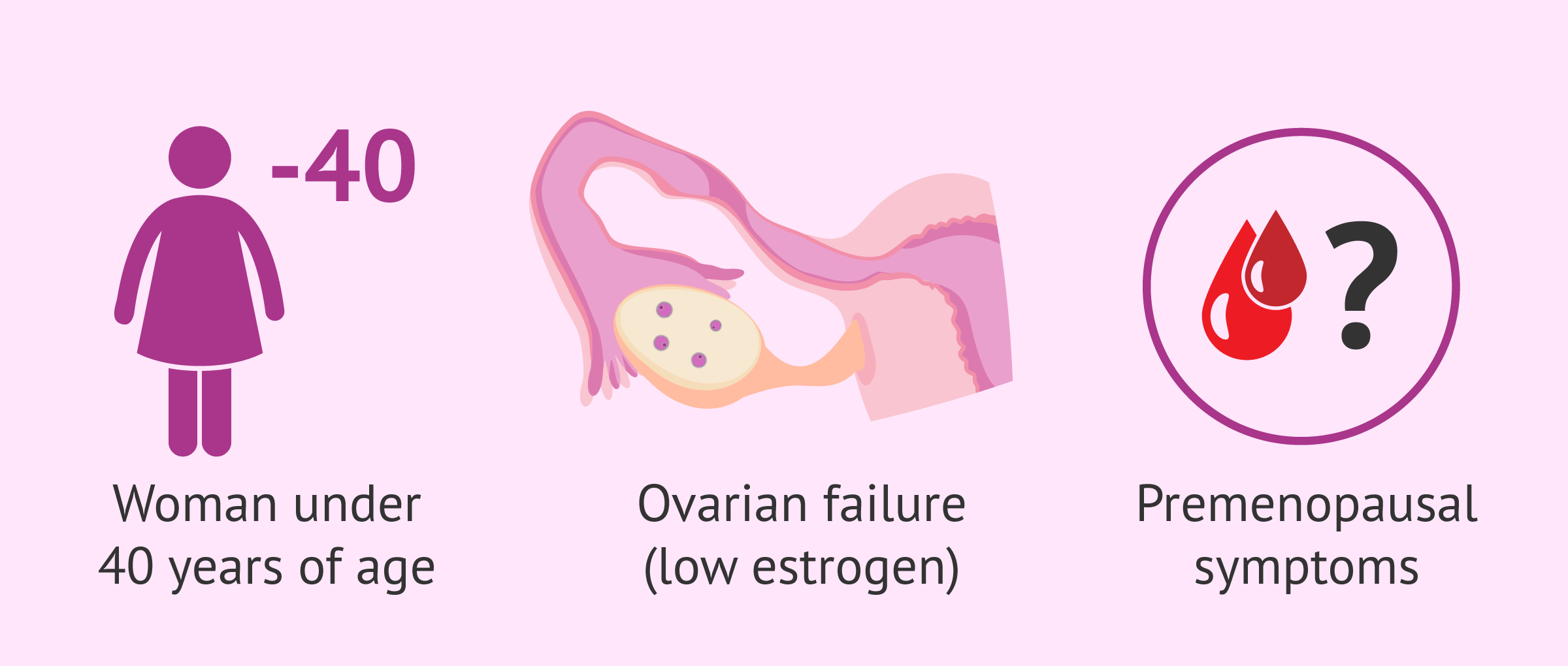
Premature ovarian failure also called primary ovarian insufficiency, refers to the loss of ovarian function in women of an early age, that is, before the average age of menopause, which is usually between 45 and 55 years.
Specifically, premature ovarian insufficiency is spoken of when a woman under 40 years of age presents amenorrhea, very low levels of estrogens, and levels of gonadotropins above 40 mIU/mL.
Throughout a woman's reproductive life, the ovaries progressively deteriorate, but in some women, they stop functioning sooner than expected, so they will not be able to achieve a natural pregnancy.
Read more about POF here: What is Premature ovarian failure (POF)?
Occult premature ovarian insufficiency
Occult ovarian insufficiency is an alteration that consists of the deterioration of ovarian function in women under the age of 40, but without having symptoms of menopause.
In other words, these women do not see their menstrual cycle altered and have regular menstrual bleeding, so the only way to diagnose ovarian insufficiency is by determining female sex hormones in the blood.
Problems with the luteal phase
The luteal phase is the second phase of the menstrual cycle, when ovulation has already taken place and the ovarian follicle becomes a corpus luteum that secretes progesterone.
In relation to this phase, there may be two situations that lead to sterility:
- Luteal phase defect (LPD)
- the ovaries do not secrete enough progesterone for endometrial development, so the embryo will not be able to implant and give rise to gestation.
- Luteinized unruptured follicle syndrome (LUF)
- occurs when the follicle continues its development to form the corpus luteum, but without having released the egg, ie, the corpus luteum is formed without having previously produced ovulation.

How to get pregnant?
Women who are trying for pregnancy and are unable to achieve it due to any of these alterations will have to go to the gynecologist and/or endocrinologist's office to carry out all the necessary diagnostic tests.
Once the exact cause preventing pregnancy is known, the specialist may consider one of the following specific treatments:
- Clomiphene citrate to induce ovulation and programmed intercourse
- Hormonal treatments such as progesterone to maintain the luteal phase
- Artificial insemination
- In vitro fertilization
- Egg donation in cases of early ovarian insufficiency

In short, this is a question of seeking the right treatment to restore the balance of sex hormones that act throughout the ovarian cycle of women. If this is not possible, the couple will have to move on to a more complex assisted reproduction treatment such as those mentioned above.
FAQs from users
Are premature ovarian failure and early menopause the same thing?
Menopause is defined as the absence of menstruation for at least one year, and this is a situation that usually occurs around the age of 51-52. We talk about early menopause when it occurs before the age of 40.
Although menopause is the final consequence of functional ovarian failure, and therefore it can be expected to happen over time, there may be a paradox that ovarian failure exists but that menstruations still occur with a certain regularity. It’s what we call occult ovarian failure.
Therefore, although related, both concepts cannot be confused since the definition of menopause is very specific and concrete.
What are the symptoms of female infertility of endocrine origin?
The main symptoms of any hormonal disorder in women are the following:
- Irregular menstrual bleeding
- No menstruation
- Acne
- Hirsutism
- Weight gain
- Changes in mood
However, these symptoms can vary from woman to woman and do not always have to occur.
Is premature ovarian failure reversible?
No. Women with ovarian insufficiency will hardly be able to regain normal ovarian function.
However, in some cases the ovary may have some intermittent activity, so these women may have spontaneous ovulations and even become pregnant.
Recommended readings
Low ovarian reserve is another cause of female sterility related to a woman's ovaries. If you would like more information, we recommend that you continue reading the article: What is an ovarian reserve and how does it affect fertility?
If you want to read more about female sterility, its causes, symptoms and treatments, we encourage you to access the following article: What causes female sterility?
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Kaiser UB. Decade in review-reproductive endocrinology: Understanding reproductive endocrine disorders. Nat Rev Endocrinol. 2015 Nov;11(11):640-1 (View)
Laven JS. Primary Ovarian Insufficiency. Semin Reprod Med. 2016 Jul;34(4):230-4 (View)
Vilaclara Mir J. Endocrine and metabolic aspects of female sterility. Rev Clin Esp. 1954 Nov 30;55(4):242-5 (View)
FAQs from users: 'Are premature ovarian failure and early menopause the same thing?', 'What are the symptoms of female infertility of endocrine origin?' and 'Is premature ovarian failure reversible?'.
Authors and contributors




More information about Cristina Algarra Goosman

Hi, I was diagnosed with early ovarian failure and we are trying to have a baby. Does this mean I will only be able to have a baby with IVF?
Hello Jasmina56,
Early ovarian failure can have several causes and being usually an endocrine thing, IVF is not necessarily the only solution.
Based on the deficiencies or excessive presence of hormones as well as the functional aspect of the reproductive system, one treatment or another may be recommended. This can range from ovulation induction through medication to ovodonation based on the needs.
If you want to know more about this condition you should read this article: Premature ovarian failure.
I hope I have helped you,
Best regards.
Hi, I’m 34 years old and already two miscarriages at 9 weeks of pregnancy… I have been treated due to endocrine causes (high prolactin and low progesterone). However I am afraid of having another abortion. What kind of check up could I do to know if there is no other reason that is preventing my pregnancies? Thank you.
Hello Glorya,
In the following post, you will find all the tests that may be done in case of repeated abortion: What Is Recurrent Miscarriage? – Causes, Symptoms & Treatment
I hope it will help you,
Have a nice day!