The womb or uterus is, along with the ovaries, the most important organ of the female reproductive system. Its function is activated thanks to the influence of sex hormones, which play a major role on the menstrual cycle. Moreover, it is home for the developing baby during the 9 months of pregnancy.
Morphological and/or functional abnormalities in the uterus can lead to female infertility.
Depending on the seriousness or the type of abnormality, the woman may experience issues in achieving pregnancy or carrying a child until birth, to the point that she may have no choice but to give up on her dream of getting pregnant and delivering a child.
Provided below is an index with the 7 points we are going to expand on in this article.
- 1.
- 1.1.
- 1.2.
- 1.3.
- 1.4.
- 2.
- 2.1.
- 2.2.
- 2.3.
- 2.4.
- 3.
- 3.1.
- 3.2.
- 3.3.
- 3.4.
- 3.5.
- 3.6.
- 3.7.
- 4.
- 5.
- 6.
- 7.
What are the uterine causes of infertility?
Uterine anomalies can be present from birth (congenital) or appear during adulthood.
In either case, uterine factor infertility (UFI) is likely to lead to sterility/infertility issues of varied severity in the affected woman. For example, it is possible that an embryo is able to attach to your womb, but that it cannot lead to an ongoing pregnancy. Oftentimes, this type of anomaly ends up in recurrent miscarriages.

In short, the following is a classification of the most common types of uterine causes of infertility in females:
Uterine malformations
The definition of uterine malformations are alterations that occur during the formation of the uterus in the fetal stage. Esto suele ocurrir entre la semana 8 y 17 de embarazo.
They are also known as Müllerian malformations, since the origin of these malformations lies in the development and/or fusion of the Müllerian ducts in female babies.
Müllerian ducts are a pair of structures of embryonic origin that develop into the uterus (womb), Fallopian tubes, cervix, and part of the vagina during embryogenesis.
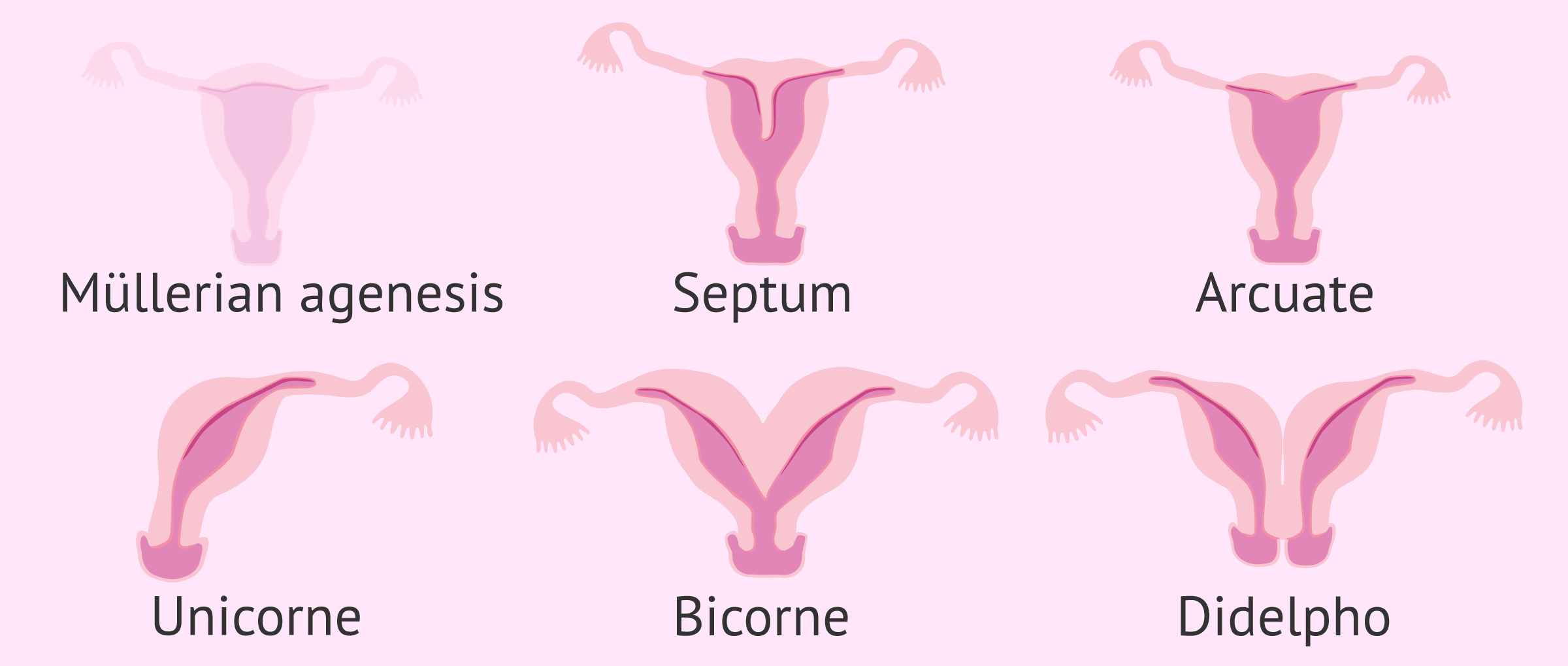
Uterine anomalies that can be present in young girls from birth due to defects in the development of Müllerian ducts are listed below:
- Müllerian agenesis
- The development Müllerian ducts is interrupted at some stag, which result in the absence of uterus. It is also known as Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome.
- Arcuate or septate uterus
- Due to defects in the lateral fusion of the Müllerian ducts. As a consequence, the uterus develops with a septum that divides it in two.
- Unicornuate uterus
- Only one Müllerian duct develops fully, which causes the uterus to have half the normal size. Only one Fallopian tube develops.
- Bicornuate uterus
- The fusion process of the Müllerian ducts is not fully completed. The result is a heart-shaped uterus.
- Uterus didelphys
- Also known as uterus didelphis or double uterus, Müllerian ducts finish their development, but don't fuse together, which results in two independent uterine cavities, with two cervices and two vaginas.
Normally, women with congenital uterine malformations are not aware of these problems until they have an ultrasound at their first gynecological visit.
Symptoms are rare, but women with uterine malformations may experience pelvic pain, dysmenorrhea, or absence of menstruation.
If you are interested in more information on this topic, you can continue reading in the following post: What Are Müllerian Duct Anomalies? – Classification with Pictures.
Synechiae
Uterine synechiae are adhesions or lesions in the walls of the uterus that cause an alteration of its morphology. This pathology is known as Asherman's syndrome.
Among the most common causes of synechiae are the following:
- Previous D&C procedures that may have caused damage to the uterine wall
- Bleeding after a C-section or vaginal birth
- Myomectomy or fibroid removal surgery
- Endometritis (infection of the endometrium)

Contrary to Müllerian duct anomalies, the Asherman's syndrome is an acquired cause of female infertility.
Tumors
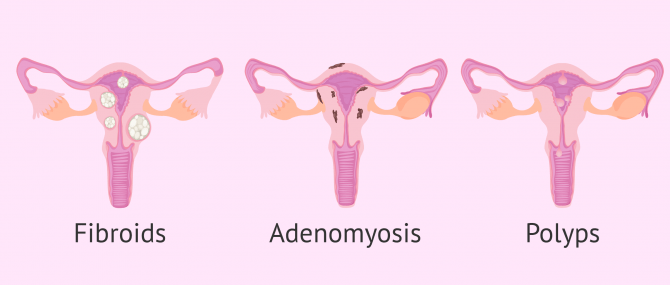
Usually, tumors that appear in the uterus are benign. The following are the most common ones:
- Fibroids
- Tumors that form in the muscular layer of the womb: the myometrium. Out of the different types of fibroids, the submucosal is the one that can alter the morphology of the uterine cavity and cause infertility.
- Adenomyosis
- The inner lining of the uterus (endometrium) breaks through the muscle wall of the uterus (myometrium).
- Uterine polyps
- Endometrial tissue that grows outside the uterine cavity and difficults embryo implantation.
In any case, the origin of these uterine tumors is the alteration of healthy cells of the uterus that begin to proliferate uncontrollably. This is the origin of the tumor mass, regardless of whether it is benign or malignant.
Causes of endometrial origin
The endometrium is the inner layer of the uterus and is where embryo implantation takes place.
The endometrium is proliferative in nature, undergoing changes in response to estrogen and progesterone hormone levels. As a result, the endometrium increases in thickness as the menstrual cycle progresses. Eventually, the endometrium sheds with menstruation if pregnancy has not occurred and, from this point on, it begins to regenerate again.
Therefore, all the alterations suffered by the endometrium can influence the correct implantation of the embryo and cause female infertility. Some of these alterations are discussed below:
- Endometritis
- Systemic inflammation of the endometrial lining due to infections caused by microorganisms like chlamydia, mycoplasma, gonococcus, or streptococcus.
- Endometrial atrophy
- The endometrial lining is too thin or even absent due to the absence of estrogens in the organism. It may be due to primary or secondary ovarian failure.
- Endometrial hyperplasia
- Increased endometrial thickness due to overstimulation caused by too high estrogen levels. The cause may be due to alterations in the functioning of the ovaries or anovulatory cycles.

Having the correct endometrial thickness at each moment of the menstrual cycle is very important, especially in women who are seeking pregnancy. The ideal would be to have an endometrium of 7-9 mm and with a trilaminar aspect, as these are the ideal characteristics that favor embryo implantation.
We recommend you to access the following article to learn more about this:What’s the Role of the Endometrium? – Function & Thickness.
What treatments are available for uterine factor?
In a situation of female sterility due to a uterine factor, first of all the doctor will have to evaluate whether it is possible to recover fertility with some pharmacological or surgical treatment.
If it is not possible to apply a drug treatment or if pregnancy is not achieved even after surgery, the couple or the woman alone will have to resort to assisted reproduction to have a child.
Pharmacological treatment
Infections that cause acute or chronic endometritis are usually treated with antibiotics based on a previous bacteriological evaluation.
In case trophic alterations of the endometrium are present, a hormone treatment based on female sex hormones like estrogens, progesterone, and FSH is effective to improve endometrial thickness.
Surgical intervention
It is usually the first option in cases of Müllerian duct anomalies. The following are the different surgical procedures used to treat uterine anomalies:
- Hysteroscopy
- To correct septa in the uterus. It is used to remove small submucosal fibroids as well as synechiae.
- Laparoscopy
- Used in the same cases as hysteroscopy but when the procedure is expected to be more challenging. Also, for the resection of horns with malformations in order to avoid the complete removal of the uterus (hysterectomy).
- Gynecological surgery
- In those cases where using endoscopic techniques is not possible. For instance, behind the presence of large subserosal fibroids.
In most cases, once the uterine abnormality has been surgically removed, the pregnancy success rates, both naturally and via fertility treatment, increase substantially.

Assisted reproduction
If it is necessary to resort to fertility treatment to achieve pregnancy due to a uterine factor, the responsible physician must assess whether it is possible to perform an artificial insemination (AI) or, instead, it is necessary to proceed directly to in vitro fertilization (IVF):
- IUI
- After processing the sperm sample, it is inserted into the uterine fundus, as it occurs during intercourse. Prior to this day, the woman undergoes mild ovarian stimulation to enhance the pregnancy chances.
- IVF
- The woman is stimulated using fertility drugs to cause the production of multiple mature eggs at the same time. Then, they are fertilized in the laboratory using the partner's sperm if possible, or donor sperm. The resulting embryos are transferred back to the womb of the intended mother after a few days of embryo culture.

The fact of using one technique or another will depend on factors such as the cause of infertility, the woman's age, the seminal quality of the male, the ovarian reserve, etc.
Surrogacy
Surrogacy, also called surrogate motherhood, is the unique reproductive option for women who don't have a womb or have a serious Müllerian duct anomaly that prevents pregnancy.
With surrogacy, another woman (the surrogate) will be in charge of maintaining the pregnancy and giving birth to the intended parents' baby.
If the intended mother is able to provide the eggs because she still has her ovaries, the baby born through surrogacy will be her biological child. If this is not possible, it will be necessary to resort to donor eggs. In no case are the surrogate woman's own eggs used.
FAQs from users
What are the chances that the mother-to-daughter uterus transplant happened in Spain as it did in Sweden?
The uterus transplant is a modality of transplantation that is in its infancy, although gynecologists are very hopeful about the good results that can be achieved at the level of reproductive problems. Spain has a large number of magnificent professionals in the field of transplants, being a pioneer in many of them. It is for this reason that, possibly, in a short time this technique can be performed in our country, if the first cases that are being carried out demonstrate the usefulness of the technique.
Are there any controversies about uterus transplantation between family members, especially between mother and daughter?
Personally, I don't think it would be any more of a problem than donating any other non-vital organ between family members (in fact, this is done with kidneys). The uterus is a very important organ as it "houses" the fetus for 9 months but does not provide any genetic information to the embryo.
What uterine malformations can diethylstilbestrol cause?
Diethylstilbestrol is a synthetic estrogen that was prescribed to pregnant women to reduce the risk of miscarriage. However, it was withdrawn from the market because it caused uterine and vaginal malformations in the daughters of women who had taken it, especially the 'T-shaped uterus'.
What is the retroverted uterus?
Retroverted or inverted uterus is a uterine anomaly that can be congenital or acquired. It consists of a variation in the position of the uterus, so that it points backwards (towards the intestine) instead of forwards (anteverted uterus).
In principle, women with a retroverted uterus do not have infertility problems, although they may experience discomfort during bowel movements or sexual intercourse.
What is the infantile uterus?
Infantile uterus or womb is a type of hypoplasia involving immaturity of the uterine tissue. During puberty in girls, their sexual organs do not develop properly and they also present delayed menarche (first menstruation).
Depending on the degree or severity of this anomaly, the woman will present sterility problems in adulthood or not.
How is uterine factor infertility studied?
Generally, the first diagnostic test to determine whether there is an alteration in the uterus is a gynecologic ultrasound.
In addition, there are other complementary tests such as hysterosalpingography, hysterosonography and hysteroscopy that can also detect uterine alterations.
What are the symptoms of uterine problems?
Although the discomfort will depend on the type of problem in the uterus that the patient presents, there are some symptoms that may raise suspicion of the existence of a uterine alteration. For example, a distended abdomen, pain in the pelvic area, frequent urination, gas accumulation and painful sexual intercourse may be a warning sign for uterine pathologies.
Therefore, it is always recommended to visit a specialist when the woman feels anything out of the ordinary in order to know the best way to proceed.
Suggested readings
When a woman is trying to conceive, having a functional, healthy womb is essential. But having a good ovarian reserve, as well as egg quality, is crucial too. To learn more about this, read: How Many Eggs Does a Woman Have? – Your Egg Count by Age.
To get a much deeper insight on all the fertility treatments available today to get pregnant, continue reading about them here: What Are Infertility Treatments? – Definition, Types & Costs.
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Christine Hur, Jenna Rehmer, Rebecca Flyckt, Tommaso Falcone. Uterine Factor Infertility: A Clinical Review. Clin Obstet Gynecol. 2019 Jun;62(2):257-270. doi: 10.1097/GRF.0000000000000448 (View)
Dominique de Ziegler, Paul Pirtea, Daniela Galliano, Ettore Cicinelli, David Meldrum. Optimal uterine anatomy and physiology necessary for normal implantation and placentation. Fertil Steril. 2016 Apr;105(4):844-54. doi: 10.1016/j.fertnstert.2016.02.023 (View)
J Preston Parry, Keith B Isaacson. Hysteroscopy and why macroscopic uterine factors matter for fertility. Fertil Steril. 2019 Aug;112(2):203-210. doi: 10.1016/j.fertnstert.2019.06.031 (View)
Kentaro Mori, Yoshimitsu Tokunaga, Tetsurou Sakumoto, Akira Nakashima, Isamu Komesu, Yutaka Hata. A Uterine Motion Classification in MRI Data for Female Infertility. Curr Med Imaging. 2020;16(5):479-490. doi: 10.2174/1573405614666180917123654 (View)
Stuart Campbell. Ultrasound Evaluation in Female Infertility: Part 2, the Uterus and Implantation of the Embryo. Obstet Gynecol Clin North Am. 2019 Dec;46(4):697-713. doi: 10.1016/j.ogc.2019.08.002 (View)
FAQs from users: 'What are the chances that the mother-to-daughter uterus transplant happened in Spain as it did in Sweden?', 'Are there any controversies about uterus transplantation between family members, especially between mother and daughter?', 'Can obesity increase the chances of having adenomyosis?', 'What uterine malformations can diethylstilbestrol cause?', 'What is absolute uterine factor infertility?', 'What is the retroverted uterus?', 'Can a woman have a baby without a womb?', 'What is the infantile uterus?', 'How is uterine factor infertility studied?' and 'What are the symptoms of uterine problems?'.
Authors and contributors




More information about Cristina Algarra Goosman

Hello, I have a problem, a few years ago I was told that I had a malformation in the uterus and that it would be difficult for me to get pregnant. Yesterday I found out that I am 4 weeks pregnant and I am afraid that the malformation may harm the pregnancy.
Hello Glenda,
Uterine malformations do not have to be incompatible with pregnancy, there are different types of malformations such as arcuate uterus, in which as a general rule there is enough space for the fetus to develop properly.
I recommend that you go to your doctor to evaluate the degree of malformation of the uterus and the viability of your pregnancy.
I hope I have helped you.
Best regards.
Hi, I’m 31 and I suffer from recurrent miscarriage. 2 years ago, I had a septate uterus surgery. Is it possible that this is the cause? Shouldn’t I be able to get pregnant after this? Thank you for your help.
Hello Clare878,
If, after the operation, there was nothing to indicate any other uterine malformation, this should not be the cause of recurrent miscarriage. Other causes may be chromosomal alteration in the embryos or coagulation problems.
I recommend you read the following post for more information: What Is Recurrent Miscarriage? – Causes, Symptoms & Treatment.
I hope I helped you.