Cesarean section is a surgical intervention that allows the birth of a baby through the mother's abdomen.
Cesarean section has some advantages over natural childbirth, such as less suffering for the baby. However, the disadvantages of this surgical technique are greater, and, therefore, the general recommendation is to apply it only in specific cases where vaginal delivery is not possible.
Provided below is an index with the 10 points we are going to expand on in this article.
- 1.
- 1.1.
- 1.2.
- 2.
- 2.1.
- 2.2.
- 2.3.
- 3.
- 4.
- 5.
- 6.
- 6.1.
- 6.2.
- 6.3.
- 6.4.
- 6.5.
- 6.6.
- 6.7.
- 7.
- 8.
- 9.
- 10.
When is a cesarean section indicated?
Cesarean section is a surgery to remove the baby at the time of birth through a double incision in the mother's abdomen and uterus.
In most cases, it is preferable for babies to be delivered naturally. However, the cesarean section has often saved the life of both mother and baby. As a result, it is a common practice in day-to-day hospital operations.
Cesarean section should be performed when there is a medical indication, either by the mother or the baby.
Maternal Indications
The reason for performing a cesarean section, urgently or not, is due to complications or illnesses of the mother who is going to give birth. The most common indications are as follows:
- Previous surgery on the uterine muscle or previous cesarean sections.
- Serious illness: cancer, heart disease, nephropathy, etc.
- Deformities or narrowing of the pelvis.

- Severe urinary or intestinal fistulas.
- Alterations in the cervix: tumor, infection, herpes, etc.
- Infection susceptible to transmission to the child through the birth canal (vertical transmission): HIV, herpes, etc.
- Diseases such as diabetes or hypertension that require speed in the process.
- Rupture of the uterus at the time of delivery.
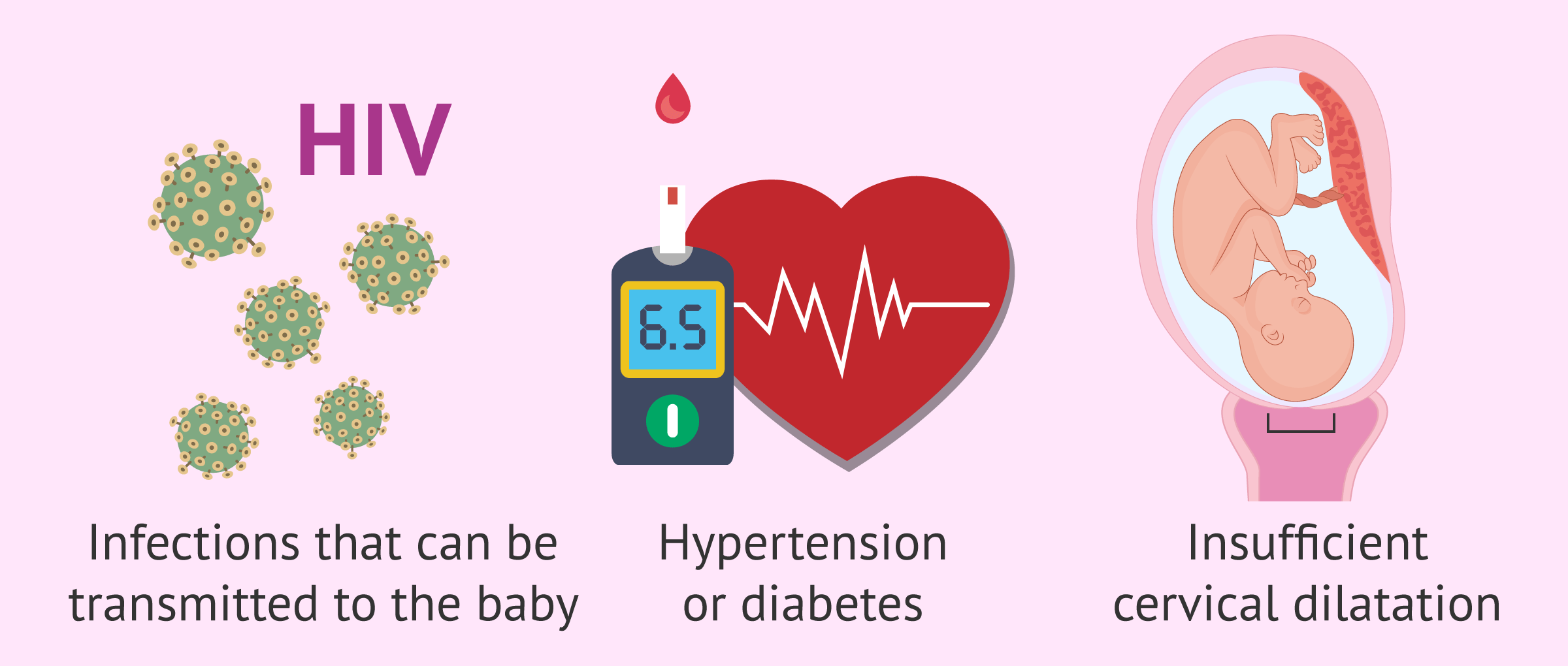
In addition, when labor stops and does not progress, or if the cervix does not dilate enough, it may also be necessary to perform a cesarean section.
Fetal Indications
In this case, the decision is made to perform a cesarean section due to complications in the fetus that may endanger the life of the fetus or the mother. These are as follows:
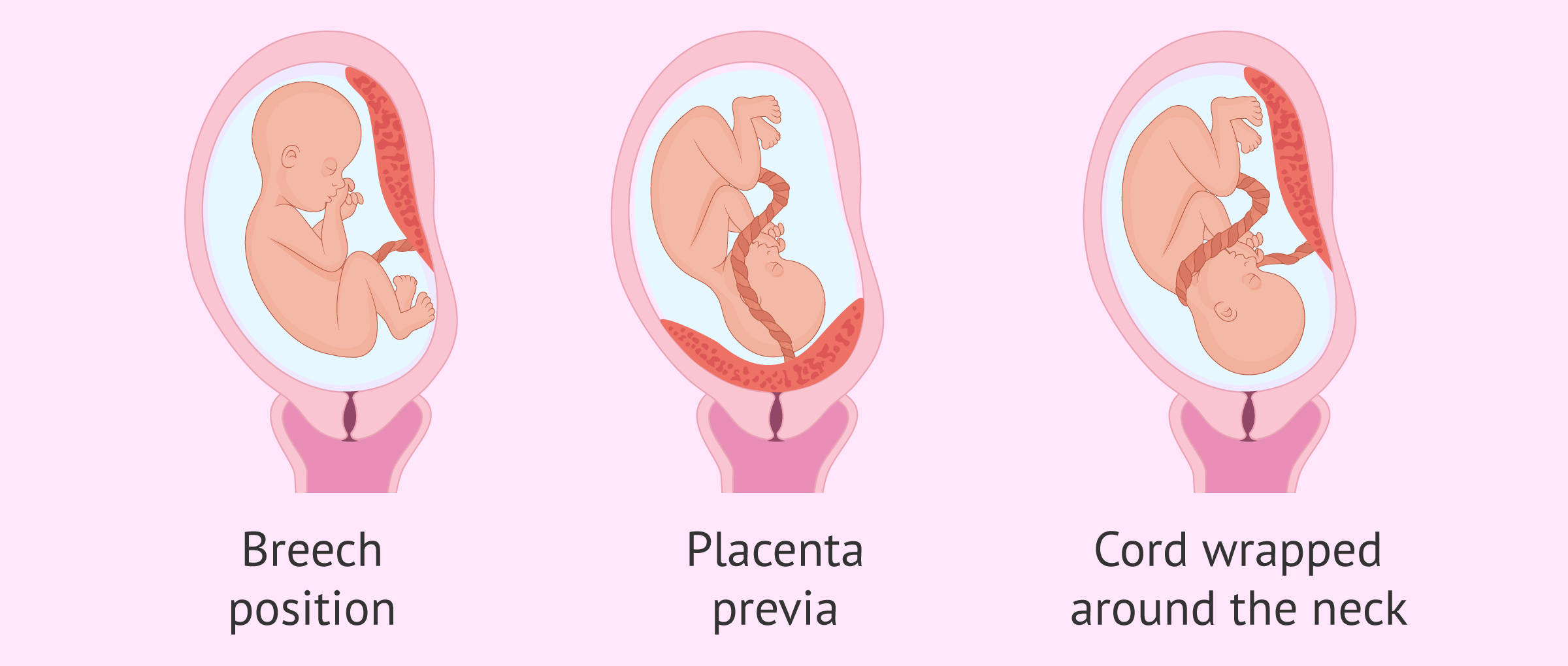
- The child is in a breech, transverse or feet-first position.
- Malformation in the fetus or Siamese twins.
- Multiple pregnancy, such as triplets.
- Previous fetal deaths.
- Placenta previa or premature detachment of the placenta.
- Cephalopelvic disproportion (CPD): the baby is too large to pass through the pelvis.
- Prolapse of the umbilical cord or when the child comes with the cord wrapped around the neck.
- Bradycardia (decreased heart rate) or any other stress indicating fetal distress.
Some of these indications are more controversial than others, as specialists consider that there is no benefit to performing a cesarean section instead of a vaginal delivery. For example, this would be the case of multiple pregnancies.
It should not be forgotten that, although the cesarean section is a relatively safe operation, it is still a major surgical procedure, with all the risks and complications that this entails.
What types of cesarean sections are there?
Depending on the factor considered, it is possible to classify the types of cesarean section in different ways.
Normally, its classification is based on the shape of the abdominal incision made in the mother. On the other hand, it is also possible to differentiate the types of the cesarean section according to the time at which it is decided to do it or if the patient already had a previous cesarean section.
Cesarean section according to abdominal cut
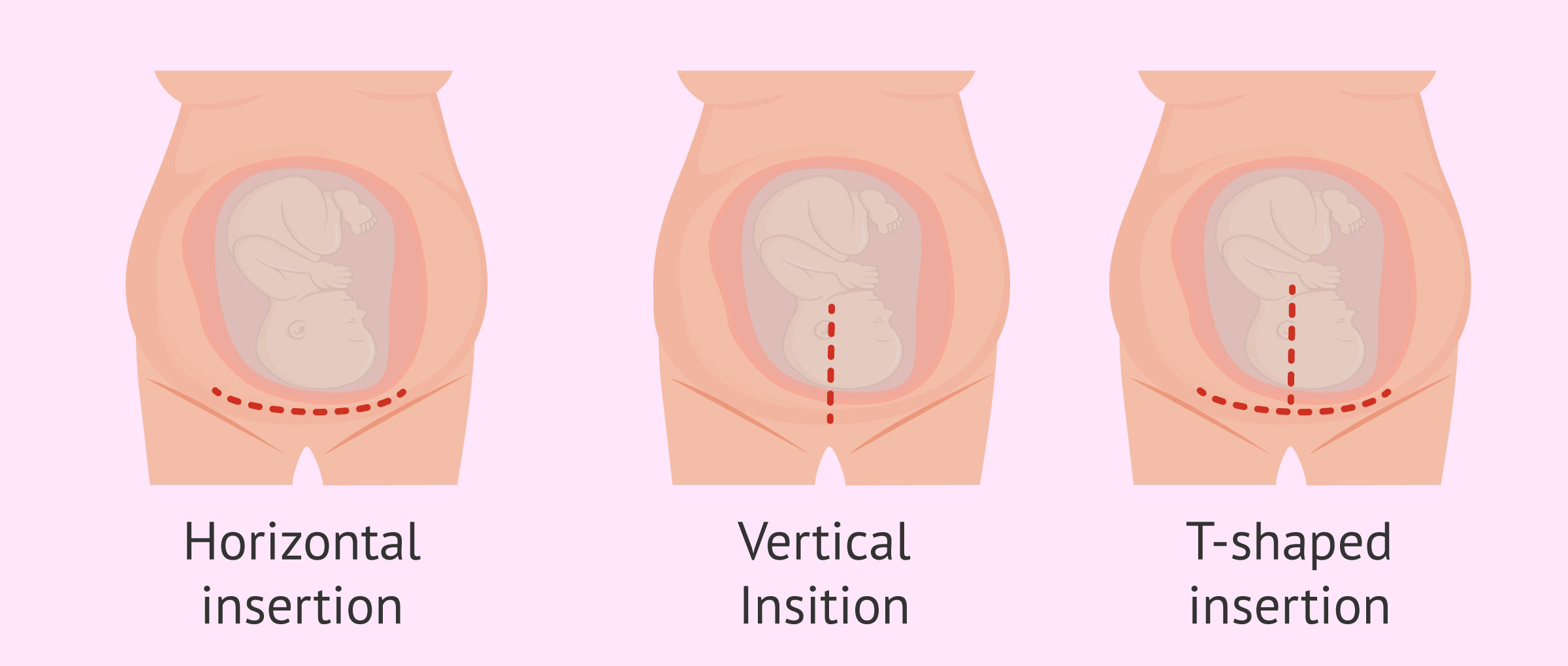
Currently, cesarean sections are segmental, which means that the cut is made in the lower segment of the uterus, where there is less damage and faster healing. We will now discuss the 3 types that exist:
- Horizontal or transverse cesarean section
- is the most common one due to the advantages it offers since there is less bleeding, the opening is easy, fewer fibers are damaged, and it leaves a more resistant and less visible scar. The cut is made in the lower belly area and is known as a bikini cut.
- T-shaped caesarean section
- involves a double cut, one horizontal and the other vertical. The scar is more conspicuous and more difficult to repair. Although it is not common, it is performed in some cases of premature delivery, large baby, breech baby or other complications, since the opening is larger and this makes it easier for the baby to come out.
- Vertical Cesarean section
- this cut fragments more fibers and causes further hemorrhage. Therefore, it is not usually done, except in certain situations such as placenta previa. In addition, the scar it leaves is aesthetically very attractive.
On the other hand, there is another type of cesarean section that is no longer commonly practiced today: the corporal or classic cesarean section. The incision is made longitudinally and goes through the uterine musculature, which implies a larger hemorrhage and a more fragile scar.
A corporal cesarean section is only performed in cases of severe myomatosis, adhesions, programmed hysterectomy, carcinoma of the cervix, etc.
Cesarean section depending on when the decision is made
Most often, a woman does not know what her delivery is going to be like until that very moment, that is, whether it will be vaginal or cesarean. However, some situations do involve making a prior decision on whether or not to have a cesarean section.
In this section, we will distinguish the following types of cesarean section:
- Emergency cesarean section
- is performed in the event of a complication during pregnancy or vaginal delivery. This makes it necessary to extract the baby as soon as possible through the abdomen to avoid serious consequences that could compromise the baby's life or that of the mother.
- Programmed or elective cesarean section
- is performed when there is a medical indication before delivery takes place. It is usually scheduled between 37 and 38 weeks of gestation. This ensures that the child is born when it is sufficiently developed and does not affect its health or that of the mother.
It should be noted that scheduled cesarean sections are currently discouraged except in very specific cases, as the risks are very high.
Cesarean section according to obstetric history
Occasionally, some doctors decide to perform a cesarean section when women have already had a previous delivery by this surgery. The reason for this is to try to prevent the previous wound from opening during labor contractions.
In this sense, we find the following classification of the cesarean section.
- Cesarean delivery
- when it is the first time the woman gives birth by this procedure.
- Previous cesarean section
- when the woman has already given birth on a previous occasion. Therefore, this would be a second cesarean delivery.
- Iterative cesarean section
- when a cesarean section is performed for the third or fourth time in the woman.
Despite all this, medical studies have shown that it is not entirely true that there is a risk of reopening of the scar and, therefore, a woman could give birth by natural childbirth without any problems after a cesarean section.
Cesarean section step by step
Cesarean section is a surgical technique that requires anesthesia to avoid pain and suffering for the mother during delivery. Currently, the type of anesthesia that offers the greatest advantage is the epidural, as it allows the mother to be conscious during the birth and avoids sedation of the baby.
In the following, we will discuss all the steps of cesarean section in general:
- Epidural anesthesia is administered.
- The pelvic area is shaved.
- A sheet is placed around the waist as a window. In this way, the mother does not see the whole procedure, as she may find it somewhat unpleasant, especially because of the blood.
- The area is disinfected and the successive layers are cut until the uterine cavity is reached.
- After the water breaks, the baby is removed. It is common for the window to be removed just as the baby is taken out so that the mother can see the baby.
- The baby is brought close to the mother so that she can cuddle it.
- The placenta is removed.
- The incisions are closed with staples and/or stitches.

Nowadays, surgery has advanced a lot and the whole process can take about 15-20 minutes, including the removal of the placenta. To this time it is necessary to add about 30-40 minutes more to close the uterus and the abdomen.
The relative safety of this intervention has made us forget its risks. This has led to an increase in the percentage of births by cesarean section so that the average is above the recommendations of the World Health Organization (WHO).
Special care
Unlike natural childbirth, recovery from a cesarean section is more expensive and involves the mother and child spending a greater number of days in the hospital, usually about 4 days.
It is important to pay close attention to the medical recommendations to treat the cesarean wound so that complications do not arise.
Some of the most important care after this operation is discussed below:
- Analgesics to relieve pain, especially during the first few days.
- Walk slowly and progressively after 24 hours to speed recovery.
- Use sanitary pads when lochia (blood loss) appears. Do not use tampons.
- The wound should be washed with soap and water daily, although iodine-based antiseptics may also be used. It is then dried well and a sterile gauze is applied over it.
- The stitches are usually removed 10 days after surgery by a physician or midwife.
- Keep the scar well hydrated with gels and creams to facilitate its deflation and subsequent disappearance. Rosehip oil is very effective for skin regeneration.
- Wear a seamless postpartum girdle for about 30 days. This will help to close all tissues well and facilitate both internal and external healing.

In addition to all these recommendations, it is advisable to wait about 40 days before resuming sexual relations or activities that require physical effort. This period is known as the postpartum quarantine.
Risks
There is a general tendency to perform more cesarean deliveries nowadays. However, in many cases, it is completely unnecessary. It should not be forgotten that cesarean section involves major abdominal surgery and therefore presents more risks compared to vaginal delivery.
Possible complications that may arise in the mother after cesarean section are as follows:
- Hemorrhages and blood clots.
- Pain after childbirth.
- Puerperal fever: fever after childbirth.
- Appearance of a seroma: infection of the surgical wound.
- Increased likelihood of complications in future pregnancies: placenta previa or placenta accreta.

On the other hand, there are also some risks for the baby born by cesarean section:
- Respiratory problems if the cesarean section is scheduled before 39 weeks.
- Broncoaspiration of amniotic fluid.
- Laceration or cut with the scalpel.
- He spends more time away from his mother during the first days, which makes it difficult to create a bond between the two.
In addition, the hospital stay and recovery from the cesarean section are longer and more complicated than those of vaginal delivery. Therefore, it is vitally important that physicians practice safe medicine and perform cesarean section only when vaginal delivery poses a real risk.
FAQs from users
When is natural childbirth recommended and when is cesarean delivery recommended?
Childbirth is the most special and awaited moment for most pregnant women. Delivery can be done vaginally or by cesarean section.
The most physiological route is the vaginal route. However, there are circumstances in which delivery by cesarean section is indicated to safeguard the health of the mother and fetus.
There are 3 types of cesarean section:
- Elective cesarean section
- is performed in the presence of some maternal or fetal pathology such as placenta previa, breech, transverse or oblique presentation, fetal macrosomia, active infections of the birth canal, 2 previous cesarean sections, some cases of growth disturbance and multiple gestations.
- The indicated cesarean section
- is recommended in the course of labor for various alterations such as arrested dilatation or descent, cephalopelvic disproportion, arrested labor, etc.
- Cesarean section
- is recommended in the course of labor for various alterations such as arrested dilatation or descent, cephalo-pelvic disproportion, arrested labor, etc.
- Urgent cesarean section
- is one in which the life of the mother and fetus is in danger as a result of a serious acute pathology.
Is it common for twin births to be by cesarean section?
Although it is true that many multiple births are by cesarean section, this does not have to be the case. As with single births, it will depend on the situation and medical recommendations.
What are the indications for a cesarean section?
The general course of action at the end of a pregnancy is natural childbirth and a cesarean section will only be performed in certain situations such as the following:
- Abnormal heart rate of the baby
- Position of the baby that hinders natural childbirth
- Developmental problems of the baby such as spina bifida or hydrocephalus
- Some cases of multiple pregnancies
- Genital infection of the mother
- Serious illness of the mother
- That the natural delivery is prolonged too long
- Placenta praevia or placental abruption
- Prolapse of the umbilical cord
In general, any situation that endangers the life of the baby or the mother will be indicative of a cesarean section.
Can cesarean section be performed under general anesthesia?
It is usual and recommended to perform the cesarean section under local anesthesia so that the mother can participate in the birth of her child and have direct contact with it from the very moment it begins its extrauterine life. However, there are risky cases in which the doctor may recommend the use of general anesthesia.
Can tubal ligation be done at the same time as a cesarean section?
Yes, in fact, it is something that many women do. It is a way of taking advantage of the abdominal cut from the cesarean section to do the definitive sterilization. In addition, the recovery from the cesarean section is the same whether it is done with or without tubal ligation.
Is it possible to have hemorrhoids after cesarean delivery?
It is not common, as hemorrhoids appear as a consequence of the great efforts made by the mother in a natural childbirth. The force of pushing causes dilatation of the rectal veins which protrude through the anus in the form of hemorrhoids.
What can I eat after a cesarean section?
As a general rule, the woman will be able to start drinking liquids and eating light food about 6-8 hours after the procedure. We refer to bland foods such as vegetable puree or soup. Gradually, the physician will introduce more foods during the hospital stay.
Once at home, the woman should follow a soft and healthy diet, with plenty of fruits and vegetables to avoid constipation.
It is also very important to avoid foods that cause gas, such as legumes, dairy products, and some vegetables. Eating slowly and chewing well also helps to avoid the gas that tends to accumulate after abdominal surgery, which is very uncomfortable.
Recommended readings
If you want to learn more about the advantages and disadvantages of cesarean birth compared to vaginal birth, you can continue reading in the following post: Which is better: natural childbirth or cesarean?
Once you have given birth, the baby's breastfeeding period will begin. To get all the information you need on this subject, we recommend you to read the following article: Infant feeding.
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Agarwal S, D'Souza R, Dy J. Induction of labour in patients with prior caesarean births or uterine surgery. Best Pract Res Clin Obstet Gynaecol. 2022 Mar;79:95-106. doi: 10.1016/j.bpobgyn.2021.12.003. Epub 2021 Dec 17. PMID: 35012884. (View)
Ahmeidat A, Kotts WJ, Wong J, McLernon DJ, Black M. Predictive models of individual risk of elective caesarean section complications: a systematic review. Eur J Obstet Gynecol Reprod Biol. 2021 Jul;262:248-255. doi: 10.1016/j.ejogrb.2021.05.011. Epub 2021 May 8. PMID: 34090730. (View)
Carter J, Bick D, Gallacher D, Chang YS. Mode of birth and development of maternal postnatal post-traumatic stress disorder: A mixed-methods systematic review and meta-analysis. Birth. 2022 Dec;49(4):616-627. doi: 10.1111/birt.12649. Epub 2022 May 13. PMID: 35561055; PMCID: PMC9790679. (View)
Fitzpatrick KE, Quigley MA, Kurinczuk JJ. Planned mode of birth after previous cesarean section: A structured review of the evidence on the associated outcomes for women and their children in high-income setting. Front Med (Lausanne). 2022 Sep 6;9:920647. doi: 10.3389/fmed.2022.920647. PMID: 36148449; PMCID: PMC9486480. (View)
Kuhr K, Axelsson PB, Andersen BR, Ammitzbøll ILA, Clausen TD, Løkkegaard ECL. Postoperative infections after non-elective cesarean section - a retrospective cohort study of prevalence and risk factors at a single center in Denmark administering prophylactic antibiotics after cord clamping. BMC Pregnancy Childbirth. 2022 Dec 17;22(1):945. doi: 10.1186/s12884-022-05300-y. PMID: 36528589; PMCID: PMC9758935. (View)
McGillick EV, Te Pas AB, van den Akker T, Keus JMH, Thio M, Hooper SB. Evaluating Clinical Outcomes and Physiological Perspectives in Studies Investigating Respiratory Support for Babies Born at Term With or at Risk of Transient Tachypnea: A Narrative Review. Front Pediatr. 2022 Jun 23;10:878536. doi: 10.3389/fped.2022.878536. PMID: 35813383; PMCID: PMC9260080. (View)
Rana T, Satwah S, Bellussi F, Berghella V. Obstetrical provider preferences for cesarean delivery on maternal request in uncomplicated pregnancies: a systematic review of the literature. Am J Obstet Gynecol MFM. 2023 May;5(5):100839. doi: 10.1016/j.ajogmf.2022.100839. Epub 2022 Dec 20. PMID: 36775197. (View)
Sotiriadis A, McGoldrick E, Makrydimas G, Papatheodorou S, Ioannidis JP, Stewart F, Parker R. Antenatal corticosteroids prior to planned caesarean at term for improving neonatal outcomes. Cochrane Database Syst Rev. 2021 Dec 22;12(12):CD006614. doi: 10.1002/14651858.CD006614.pub4. PMID: 34935127; PMCID: PMC8692259. (View)
Sys D, Kajdy A, Baranowska B, Tataj-Puzyna U, Gotlib J, Bączek G, Rabijewski M. Women's views of birth after cesarean section. J Obstet Gynaecol Res. 2021 Dec;47(12):4270-4279. doi: 10.1111/jog.15056. Epub 2021 Oct 5. PMID: 34611958. (View)
FAQs from users: 'When is natural childbirth recommended and when is cesarean delivery recommended?', 'Is it common for twin births to be by cesarean section?', 'What are the indications for a cesarean section?', 'Can cesarean section be performed under general anesthesia?', 'Can tubal ligation be done at the same time as a cesarean section?', 'Is it possible to have hemorrhoids after cesarean delivery?' and 'What can I eat after a cesarean section?'.
Authors and contributors



More information about Cristina Algarra Goosman
Find the latest news on assisted reproduction in our channels.

Hello, is there a way to try to have a vaginal delivery after a cesarean? I had an emergency c-section with my last pregnancy two years ago and now I’m pregnant and want to try for a vaginal birth.
Hola RubyAnn,
Having a vaginal delivery after a c section is known as a VBAC. Depending on the professional that monitors your pregnancy and their experience they will recommend going to a vaginal delivery or opt for another c section. It will most likely depend on how the previous c section scar healed and the time that passed from the previous surgery.
I recommend you speak to your provider and communicate your desire to try a vaginal delivery, they will assess the possibility of this type of delivery and possible risks and complications.
I hope everything goes okay,
All the best
Hi, I am 35 weeks pregnant and the baby has been very big all along. I have been told that I will most likely need a c-section but now that the time is approaching he is breech and will not be able to come out. I am scheduled for induction in a few weeks and I am scared.
Hi Bobbie,
There are some situations where the cesarean section is medically necessary. If the baby is measuring above the weight considered average for its gestational age there may be complications for a vaginal delivery as it can cause vaginal tears or ruptures both of which are harmful to the mother. It can also become wedged and require an emergency cesarean section, which can put the baby under stress during labor.
Therefore I recommend you to follow the advice and recommendations of the doctor as he/she will be able to assess the safest option for both of you.
Best regards
During my whole pregnancy, I prayed so that I had a natural, easy delivery. However, when the day arrived, a caesarean had to be performed. But the truth is that it was wonderful. I didn’t suffer a lot with the removal o the stitches.Now, I just have a small scar.