Tubal ligation is a surgical intervention on a woman's fallopian tubes to prevent pregnancy.
It is a permanent method of contraception that has advantages and disadvantages. Therefore, a woman must be sure that she does not want any more children before having a tubal ligation. However, there are alternatives for getting pregnant after tubal ligation.
Provided below is an index with the 9 points we are going to expand on in this article.
- 1.
- 1.1.
- 1.2.
- 1.3.
- 1.4.
- 2.
- 3.
- 4.
- 5.
- 5.1.
- 5.2.
- 5.3.
- 5.4.
- 5.5.
- 5.6.
- 5.7.
- 5.8.
- 5.9.
- 5.10.
- 5.11.
- 6.
- 7.
- 8.
- 9.
How is a tubal ligation performed?
Tubal ligation, also called bilateral tubal bilateral tubal occlusion(BTO), is a definitive sterilization method. There are several types of surgery to close the fallopian tubes and prevent them from carrying out their function:
- The transport of the egg from the ovary to the uterus.
- The meeting of the egg with the sperm for fertilization to take place.
Therefore, the procedure must be done in both fallopian tubes, so that the sperm cannot reach the egg and attach to it. Tubal ligation surgery can be performed laparoscopically or hysteroscopically, requires anesthesia and lasts approximately 30 minutes.
Depending on the method used to obstruct or cut the tubes, the following types of tubal ligation are differentiated:
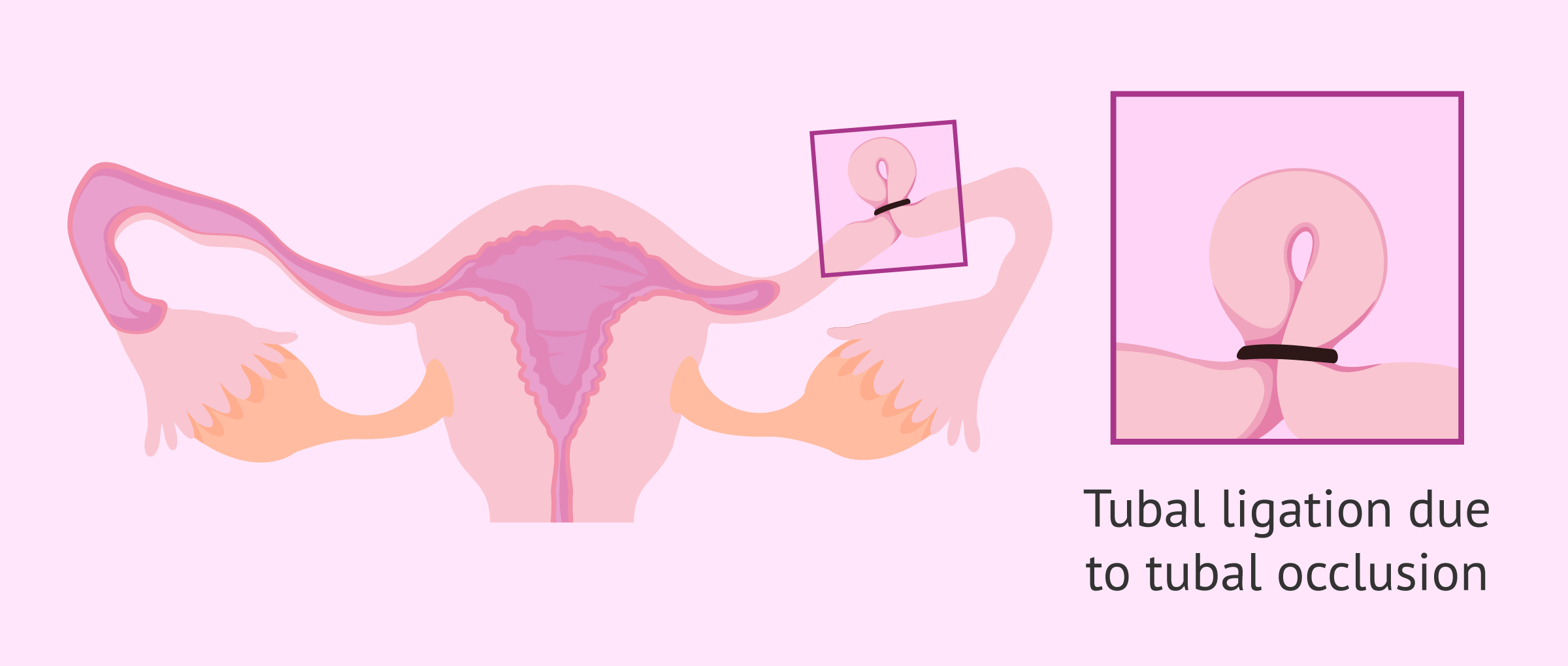
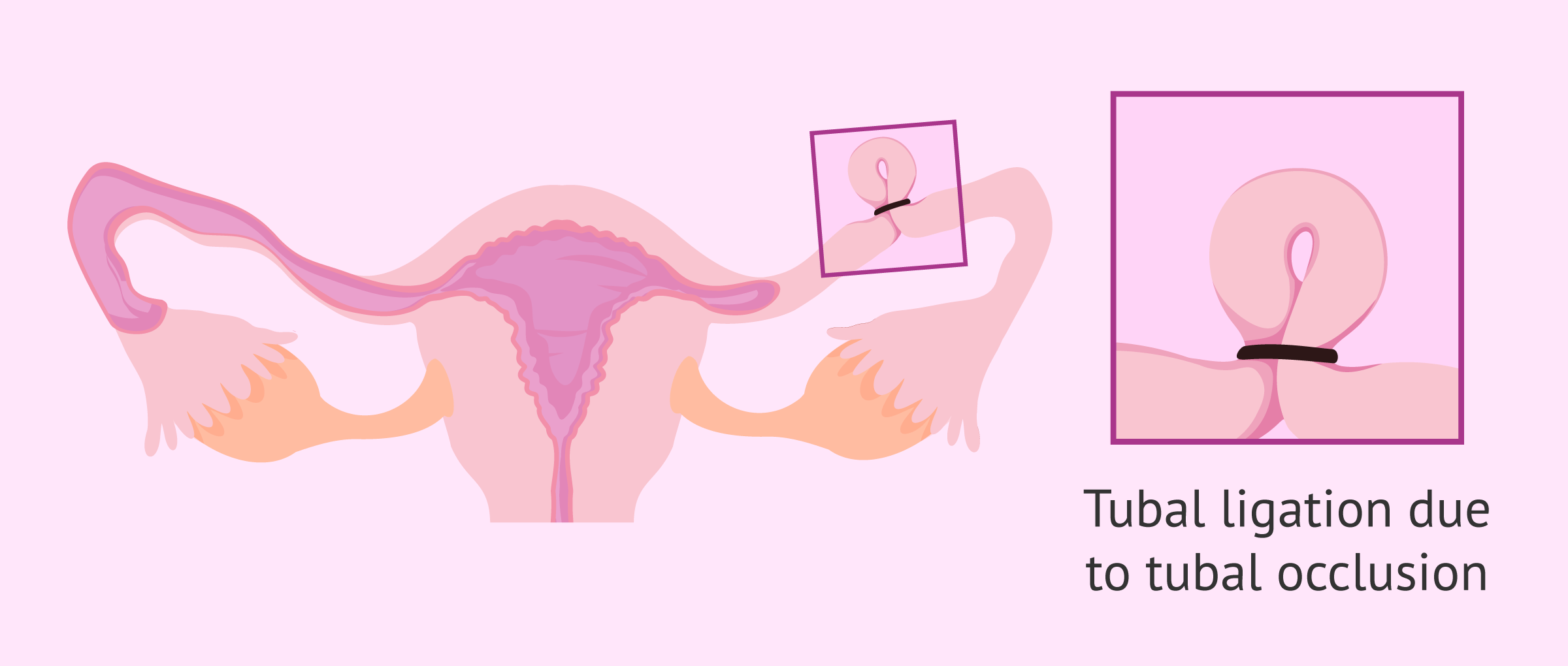
Partial salpingectomy
Partial salpingectomy consists of cutting the tubes and tying their ends with suture material.

The Pomeroy technique is one of these types of tubal occlusion most commonly used today. This method consists of tying the base of a loop about 3-4 cm from the tube and removing the upper segment.
Generally, the term Pomeroy is used as a synonym for tubal ligation.
Tubal occlusion
This technique consists of placing a ring, clip or staple to cause a compression and obstruction in the tube that prevents its functioning.
The objects used in this type of ligation can be made of titanium (Filshie clamp), plastic (Wolf clamp) or silicone (Yoon ring).
This is the easiest type of surgery to reverse in case you regret tubal ligation in the future. However, regaining tubal function will depend on the site of insertion of the clip, the damage done to the tube, the woman's age, etc.
You can read the following article for more information on this: Is It Possible to Reverse Tubal Ligation?
Electrocoagulation
This is a method that uses an electric current to coagulate or cauterize the ends of the fallopian tube that remain after cutting it.

This method is also known as fallopian tube cauterization. Coagulation can be unipolar or bipolar. In the case of unipolar, the electric current passes through a forceps and exits through an electrode placed on the woman. In contrast, if it is bipolar, the current enters the woman's body and exits through the electrodes of the forceps.
Despite the existence of these two methods, it is more common to opt for bipolar coagulation because it is safer.
Essure
The Essure method of tubal ligation does not require a surgical incision or anesthesia. It is a titanium metal micro-insert that, when inserted inside the tube, produces an inflammation that will eventually lead to scarring. This scar will then act as a natural barrier and obstruct the tube.

For the Essure method to be effective, at least 3 months must pass since its placement. During this time, it is necessary for the woman to use other contraceptive methods. The effectiveness of the Essure method of tubal ligation is quite high, around 99.8%.
When is tubal ligation indicated?
Tubal ligation is a relatively easy and safe surgery for women. However, it should be noted that this is a permanent sterilization method.
To reverse tubal ligation, it is necessary to undergo another surgical procedure which, moreover, does not guarantee success in achieving pregnancy.
For all these reasons, a woman should be completely sure about having a tubal ligation, the most common indications being the following:
- The woman already has several children and does not wish to have more in the future.
- The woman is of advanced maternal age and no longer wants to have children.
- Women aged 40-50 years with a history of ovarian cancer, as removing the fallopian tubes may decrease this risk.
- When the woman's health condition does not allow a proper pregnancy or may even represent a danger to her life.

Despite all this, there are women who regret tubal ligation and wish to have another child after a few years. This is one of the main reasons why a couple goes to an assisted reproduction clinic nowadays.
Assisted procreation, as any other medical treatment, requires that you rely on the professionalism of the doctors and staff of the clinic you choose. Obviously, each clinic is different. Get now your Fertility Report, which will select several clinics for you out of the pool of clinics that meet our strict quality criteria. Moreover, it will offer you a comparison between the fees and conditions each clinic offers in order for you to make a well informed choice.
Advantages of tubal ligation
One of the main advantages of tubal ligation is that it is quite effective and has a high reliability. The probability that the procedure will go well is 99%. Numerous benefits of tubal ligation as a method of permanent contraception for women are listed below:
- It avoids being continuously on hormonal contraceptives, which is beneficial for the body, as it does not alter the menstrual period or natural hormones.
- It avoids the need to take a daily contraceptive pill or use a condom for every sexual intercourse, which improves the couple' s sex life.
- The effectiveness of tubal ligation is very high, preventing pregnancy in more than 99% of cases.
- It can be performed at any time, even at the time of delivery if it is by cesarean section, always with the woman's consent.
- The operation is not complicated and, if everything proceeds normally, you can leave the hospital 2 to 6 hours after the operation.
- It does not require revisions or continuous medical visits, unless there are complications or the patient feels the need.
The woman should only have a check-up 7 days after the operation to ensure that there is no infection or other side effects from the surgery.
Disadvantages and/or side effects
Despite the benefits of tubal ligation, it is important to keep in mind that it is an intervention and, therefore, the patient must assume the surgical and anesthetic risks derived from it.
In the short term, recovery from the ligation operation is usually rapid and without major discomfort. However, there may be a series of symptoms or complications in the postoperative period: problems due to anesthesia, hemorrhages, hematomas or infection of the scar.
There are also some long-term consequences such as:
- It is irreversible. The woman may not become fertile again even if a tubal ligation reversal is performed.
- Increased risk of ectopic pregnancy.
- It does not protect against sexually transmitted diseases.
- In case of becoming a mother again, it is necessary to resort to IVF, a very expensive assisted reproduction technique.

Finally, it should be noted that there is a risk of unwanted pregnancy in 1 in 200 women with tubal ligation due to spontaneous tubal recanalization.
FAQs from users
Is tubal ligation dangerous for women?
Tubal ligation is a permanent method of contraception in which the fallopian tubes are cut, tied, or blocked to prevent pregnancy. The procedure itself has no consequences for the woman's menstrual cycle.
However, since tubal ligation is an operation under anesthesia that involves incision of the abdomen, there are some risks associated with the surgical intervention:
- Damage to intestines, bladder, or major blood vessels
- Reaction to anesthesia
- Inadequate wound healing or infection
- Continuous pelvic or abdominal pain
- Failure of the procedure, resulting in unwanted future pregnancy
What possibilities does assisted reproduction offer to become a mother after a tubal ligation?
The best option to achieve a pregnancy after having had a tubal ligation is to resort to in vitro fertilization (IVF). Another possible option would be to try to repair the fallopian tubes by an operation called tubal reanastomosis, i.e. joining the ends of the cut tubes together again.
Read more
How much does tubal ligation cost?
The cost of tubal ligation ranges from €1,000-€7,000. In comparison, the cost of a vasectomy is much less, so couples who agree to have no more kids are advised to consider the type of surgery they want to undergo taking this factor into account. Centers and hospitals carrying out this procedure may different different financing options for patients.
Is a tubal ligation less successful during a C-section?
Actually, there is no scientific research that confirms this theory. What has been shown, however, is that a woman is likely to get pregnant after having tubal ligation through laparotomy (during a C-section), vaginal delivery or laparoscopic surgery.
Can you get your tubes tied on the NHS?
Some patients may be referred for free sterilization on the NHS by their GP or another GP they have registered with for family planning services. Nevertheless, you should take into account that the waiting list on the NHS may be quite long, so you may consider getting private treatment—the cost is often more than £1,000.
Endometrial ablation (NovaSure), hysterectomy or tubal ligation, what's better?
Endometrial ablation means having your endometrial lining removed, while hysterectomy means having your uterus removed, so it should be clear that they are not a birth control methods. It is indicated in cases of women with heavy menstrual bleeding. If the purpose of considering these procedures is just being unable to conceive, we recommend you to go for tubal ligation, as it could be reversed in case you wanted to have a baby in the future.
Is it possible for me to get tubal ligation reversal insurance coverage somewhere?
In general, women will not get health insurance coverage if it is an elective tubal ligation reversal, and the same applies in case you want to have your Essure coil removed. On the other hand, you may find insurance coverage if it is medically necessary (e.g. it prevents or treats an injury, disease or the symptoms associated with a certain condition).
Can having your tubes tied cause early menopause?
Although tubal ligation does not stop periods, tubal ligation can make women experience some menopause-like symptoms. It actually leads to premature menopause rarely.
Can you get your tubes tied without having a baby?
The truth is, most doctors are not willing to perform a tubectomy on women under 32 with less than 3 children as a general rule. Take into account that you can change your mind when you turn 35 and regret the choice you made at 26, for example.
Does having your tubes tied while breastfeeding affect your milk supply?
No, tubal ligation procedures are fully compatible with breastfeeding. However, medications prescribed during the tubectomy procedure may cause a temporary effect on it.
Is there any type of tubal ligation which is temporary?
No, tubal ligation procedures are meant to be permanent, that is why it is considered to be a permanent birth control method. If you want to be protected against an unplanned pregnancy during a particular period of time, you should consider using a non-permanent birth control method, including the birth control pill or the vaginal ring.
Suggested for you
There are numerous female contraceptive methods and it can be confusing for women to decide on one. For more information on this topic, we recommend you visit the following post: Contraceptive methods.
There is another method of definitive sterilization for men that is simpler than tubal ligation. We refer to vasectomy and you can get all the information about this procedure in the following article: What is vasectomy?
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Alessandra J Ainsworth, Sarah C Baumgarten, Jamie N Bakkum-Gamez, Celine M Vachon, Amy L Weaver, Shannon K Laughlin-Tommaso. Tubal Ligation and Age at Natural Menopause. Obstet Gynecol. 2019 Jun;133(6):1247-1254. doi: 10.1097/AOG.0000000000003266 (View)
Christine R Langton, Brian W Whitcomb, Alexandra C Purdue-Smithe, Lynnette L Sievert, Susan E Hankinson, JoAnn E Manson Bernard A Rosner, Elizabeth R Bertone-Johnson. Association of oral contraceptives and tubal ligation with antimüllerian hormone. Menopause. 2021 Dec 6;29(2):225-230. doi: 10.1097/GME.0000000000001905 (View)
Laleh Loghmani, Nafise Saedi, Reza Omani-Samani, Saeid Safiri, Mahdi Sepidarkish, Saman Maroufizadeh, Arezoo Esmailzadeh, Maryam Shokrpour, Esmaeil Khedmati Morasae, Amir Almasi-Hashiani. Tubal ligation and endometrial Cancer risk: a global systematic review and meta-analysis. BMC Cancer. 2019 Oct 11;19(1):942. doi: 10.1186/s12885-019-6174-3 (View)
Sharon Sung, Aaron Abramovitz. Tubal Ligation.In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan.2023 Jul 25 (View)
FAQs from users: 'Is tubal ligation dangerous for women?', 'What possibilities does assisted reproduction offer to become a mother after a tubal ligation?', 'How much does tubal ligation cost?', 'Is a tubal ligation less successful during a C-section?', 'Can you get your tubes tied on the NHS?', 'Endometrial ablation (NovaSure), hysterectomy or tubal ligation, what's better?', 'Is it possible for me to get tubal ligation reversal insurance coverage somewhere?', 'Can having your tubes tied cause early menopause?', 'Can you get your tubes tied without having a baby?', 'Does having your tubes tied while breastfeeding affect your milk supply?' and 'Is there any type of tubal ligation which is temporary?'.
Authors and contributors





I’m considering getting my tubes tied but I’m worried if I’ll enter early menopause. Please help!
Hello Melanie
Although tubal ligation does not stop periods, tubal ligation can make women experience some menopause-like symptoms. It actually can lead to premature menopause in rare cases.
Best
Hello, I’m 36 and already have 3 children. My husband and I don’t want to have more children but wish to leave condoms, pills, etc. behind and enjoy a full sexual life now that our children are teenagers. I’ve considered tubal ligation, but I’m afraid of surgery, so I’ve thought about using the contraceptive implant, as it can be changed every 3 years, which is very comfortable as well. How effective is it?
Dear Virginia,
the implant must be inserted during the first 5 days of your menstruation and it is a highly accurate method of birth control. However, if you do not wish to take additional hormones, the implant works by releasing them too, so it may become uncomfortable for you as well. Anyhow, consider it twice before undergoing a tubal ligation.
The following articles may be of interest:
1. Birth control methods
2. Tubal ligation and pregnancy
Best regards