Cesarean section is a surgical procedure in which an incision is made in the abdomen and another in the uterus of the pregnant woman to facilitate the delivery of the baby or babies. This implies that the delivery occurs via the abdomen, rather than the baby passing through the birth canal to be born vaginally.
Since it is a major surgery, cesarean section has some risks for both mother and baby. Therefore, a cesarean section should only be performed when there is a medical indication and the benefits outweigh the risks.
Provided below is an index with the 10 points we are going to expand on in this article.
- 1.
- 2.
- 3.
- 4.
- 4.1.
- 4.2.
- 5.
- 5.1.
- 5.2.
- 6.
- 6.1.
- 6.2.
- 6.3.
- 7.
- 8.
- 9.
- 10.
What is a scheduled or elective cesarean section?
A cesarean section is a surgical procedure performed on a pregnant woman to remove the baby or babies via the abdomen. Generally, cesarean section is performed when there are possible risks or complications in a vaginal delivery in order to avoid them.
Depending on when it is decided to perform a cesarean section, two types of cesarean section can be distinguished:
- Planned or elective cesarean section: refers to a cesarean section that is performed in a planned manner before the onset of labor, since it is already known that vaginal delivery could present risks and is inadvisable. Recommendations can be read that indicate not to schedule this type of cesarean section before 39 weeks (and earlier only if there is a medical indication that justifies it).
- Emergency cesarean section: is a cesarean section performed during the course of labor, unexpectedly and unplanned, due to the occurrence of some complication.

However, cesarean section is a major surgical procedure and, therefore, is not risk-free. Thus, the risks and benefits of performing a cesarean section must be carefully weighed.
Indications for planned cesarean section
A decision may be made to planned a cesarean section if any of the following situations occur during pregnancy:
- Podalic (breech) or transverse presentation of the baby. However, vaginal breech delivery is also possible when certain requirements are met.
- Multiple pregnancy, especially if any of the babies are not in cephalic presentation.
- Placenta previa, i.e. when the placenta covers the opening of the cervix.
- Myomas that may be obstructive.
- Hydrocephalus in the baby, which would make it difficult for the head to pass through the maternal pelvis.
- Maternal diseases, such as heart disease, or infections with risk of vertical transmission to the baby at the time of delivery.
- Previous cesarean sections, although vaginal delivery is possible after a previous cesarean section, especially if the uterine incision was horizontal.

In any case, a cesarean section should be avoided when there is no medical indication to justify it and should always be performed when the benefits outweigh the risks of this type of surgery.
How is a planned cesarean section performed?
When a scheduled cesarean section is performed, the woman is usually monitored and awake, using epidural anesthesia to avoid pain. This allows the woman to be aware of the moment of birth of her baby, unlike an emergency cesarean section where general anesthesia is usually used.
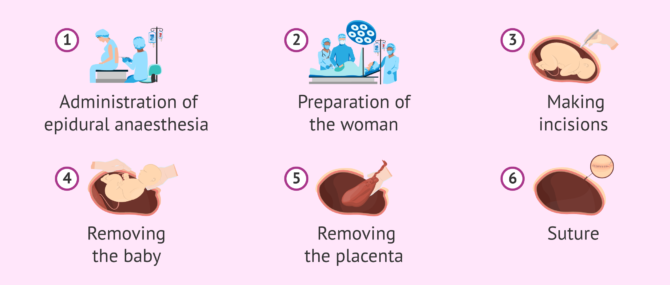
The procedure for performing a scheduled cesarean section is generally as follows:
- Monitor the pregnant woman and start an intravenous line to administer fluids and drugs.
- Shave pubic hair and disinfect the abdomen.
- Install a curtain at waist level, so that the pregnant woman cannot see her abdomen during the operation. However, it can be removed just at the moment when the baby is to be removed.
- Make an abdominal incision, usually horizontal and slightly above the pubic hairline.
- Separate the abdominal musculature.
- Make a uterine incision. Again, a horizontal incision is the most common.
- Extracting the baby.
- Extract the placenta.
- Suture uterus and abdomen.
Since the woman is awake, it is possible that a companion may enter the operating room, although this may vary from hospital to hospital.
Potential Risks for planned cesarean section
Cesarean section is a major surgery and, therefore, like any other type of surgery, it is not risk-free. Therefore, a cesarean section should only be performed when necessary and the benefits to mother and baby outweigh the risks.
Maternal risks
Possible risks to the mother of a cesarean section, in addition to longer hospital admission and recovery time, include:
- Adverse effects of anesthesia.
- Injury to nearby organs.
- Infections: in the uterus, in the urinary tract or in the incision made.
- Heavy bleeding and hemorrhage.
- Blood clots (deep vein thrombosis) and pulmonary embolism.

In addition, the risk of some complications with the placenta in a subsequent pregnancy would be higher after a cesarean section. On the other hand, if you have a vaginal delivery after a cesarean section, there is a possible risk of uterine rupture.
Risks to the baby
The baby may also experience possible problems or complications after a scheduled cesarean section. Among them, we can mention transient tachypnea of the newborn. This is a respiratory problem in which the baby will breathe faster for a few days after birth.
Rarely, however, lesions may also occur on the baby's skin as a result of the procedure.
Recommendations
A scheduled cesarean section is a surgical operation that involves a postoperative period in which the woman will gradually recover. Therefore, it may be useful to keep these recommendations in mind.
Before cesarean section
Scheduling a cesarean section assumes that there is a planned date and time for the procedure. Therefore, the woman can organize certain things in advance:
- Prepare the bag for the hospital, taking into account that the hospital stay will be longer than if the delivery were vaginal.
- Ask for help with household chores, care of other children and pets (if applicable) and any necessary tasks during the period when the woman is in the hospital and recovering.
Finally, the woman should not forget to fast on the day of the procedure and comply with the guidelines indicated by the specialist.
After the procedure
Once the cesarean section has been performed, the woman should keep in mind:
- Do not lift weight.
- Do not self-medicate and take only the analgesics prescribed by the doctor, especially if the baby is breastfed.
- Allow time for recovery and avoid sexual intercourse, strenuous exercise and driving until the specialist gives the go-ahead.
- Walking to reduce the risk of blood clots.
- Do not force yourself and ask for help when necessary.

In addition, if there are any signs of infection in the wound, fever, bleeding or any symptoms that are not considered normal, the specialist should be consulted.
FAQs from users
Do breech deliveries always end in cesarean section?
Breech presentation (breech or feet down) has an incidence of between 3 and 4%. Vaginal delivery in breech presentation has shown a higher incidence of problems at delivery and poor perinatal outcomes compared to cephalic delivery.
Therefore, it is a medical indication to perform a scheduled cesarean section at 39 weeks, which is considered a safer procedure for the newborn. However, cesarean section is not free of maternal risks mainly, so one of the current recommendations is to perform an external cephalic version (attempt to turn the baby by external obstetric maneuvers).
Is it common for twin births to be by cesarean section?
Although it is true that many multiple births are by cesarean section, this does not have to be the case. As with single births, it will depend on the situation and medical recommendations.
Which is better, vaginal delivery or a cesarean section?
There are many theories about how childbirth should be, as well as many doctors in favor of cesarean section and many advocates of natural childbirth.
It should be noted that vaginal childbirth is a natural process. The woman's body is hormonally and mechanically prepared to be able to carry it out even without medical intervention. However, unforeseen events may arise at the time of delivery that force professionals to decide to perform a cesarean section.
On the other hand, there are women who prefer to give birth by cesarean section because they are afraid of pain, but it should be noted that the recovery is much worse than with natural childbirth. In addition, women with cesarean section will need assistance and help from family members during the first few days, both for daily routines and to take care of the newborn.
In any case, at the moment of delivery, the health of both the future baby and the mother who is going to give birth will always be taken into account.
Suggested for you
If you want to read more information about how a cesarean section is performed, you can visit the following link: Cesarean section: how is it performed and what care is needed?
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Agarwal S, D'Souza R, Dy J. Induction of labour in patients with prior caesarean births or uterine surgery. Best Pract Res Clin Obstet Gynaecol. 2022 Mar;79:95-106. doi: 10.1016/j.bpobgyn.2021.12.003. Epub 2021 Dec 17. PMID: 35012884. (View)
Ahmeidat A, Kotts WJ, Wong J, McLernon DJ, Black M. Predictive models of individual risk of elective caesarean section complications: a systematic review. Eur J Obstet Gynecol Reprod Biol. 2021 Jul;262:248-255. doi: 10.1016/j.ejogrb.2021.05.011. Epub 2021 May 8. PMID: 34090730. (View)
Carter J, Bick D, Gallacher D, Chang YS. Mode of birth and development of maternal postnatal post-traumatic stress disorder: A mixed-methods systematic review and meta-analysis. Birth. 2022 Dec;49(4):616-627. doi: 10.1111/birt.12649. Epub 2022 May 13. PMID: 35561055; PMCID: PMC9790679. (View)
Fitzpatrick KE, Quigley MA, Kurinczuk JJ. Planned mode of birth after previous cesarean section: A structured review of the evidence on the associated outcomes for women and their children in high-income setting. Front Med (Lausanne). 2022 Sep 6;9:920647. doi: 10.3389/fmed.2022.920647. PMID: 36148449; PMCID: PMC9486480. (View)
Kuhr K, Axelsson PB, Andersen BR, Ammitzbøll ILA, Clausen TD, Løkkegaard ECL. Postoperative infections after non-elective cesarean section - a retrospective cohort study of prevalence and risk factors at a single center in Denmark administering prophylactic antibiotics after cord clamping. BMC Pregnancy Childbirth. 2022 Dec 17;22(1):945. doi: 10.1186/s12884-022-05300-y. PMID: 36528589; PMCID: PMC9758935. (View)
McGillick EV, Te Pas AB, van den Akker T, Keus JMH, Thio M, Hooper SB. Evaluating Clinical Outcomes and Physiological Perspectives in Studies Investigating Respiratory Support for Babies Born at Term With or at Risk of Transient Tachypnea: A Narrative Review. Front Pediatr. 2022 Jun 23;10:878536. doi: 10.3389/fped.2022.878536. PMID: 35813383; PMCID: PMC9260080. (View)
Rana T, Satwah S, Bellussi F, Berghella V. Obstetrical provider preferences for cesarean delivery on maternal request in uncomplicated pregnancies: a systematic review of the literature. Am J Obstet Gynecol MFM. 2023 May;5(5):100839. doi: 10.1016/j.ajogmf.2022.100839. Epub 2022 Dec 20. PMID: 36775197. (View)
Sotiriadis A, McGoldrick E, Makrydimas G, Papatheodorou S, Ioannidis JP, Stewart F, Parker R. Antenatal corticosteroids prior to planned caesarean at term for improving neonatal outcomes. Cochrane Database Syst Rev. 2021 Dec 22;12(12):CD006614. doi: 10.1002/14651858.CD006614.pub4. PMID: 34935127; PMCID: PMC8692259. (View)
Sys D, Kajdy A, Baranowska B, Tataj-Puzyna U, Gotlib J, Bączek G, Rabijewski M. Women's views of birth after cesarean section. J Obstet Gynaecol Res. 2021 Dec;47(12):4270-4279. doi: 10.1111/jog.15056. Epub 2021 Oct 5. PMID: 34611958. (View)
FAQs from users: 'Do breech deliveries always end in cesarean section?', 'Is it common for twin births to be by cesarean section?' and 'Which is better, vaginal delivery or a cesarean section?'.



