Uterine myomatosis is the appearance of uterine myomas, which are benign tumors that develop in the uterus from its smooth muscle: the myometrium.
They are also called fibroids, fibromyomas, or leiomyomas. There are three types of myomas; subserosal, intramural and submucous. The most frequent are subserosal fibroids whose prevalence is approximately 55%.
Treatment will depend primarily on the woman's symptoms, age, and if she wants to become mother.
Provided below is an index with the 11 points we are going to expand on in this article.
- 1.
- 2.
- 3.
- 4.
- 5.
- 5.1.
- 5.2.
- 6.
- 7.
- 7.1.
- 7.2.
- 7.3.
- 7.4.
- 7.5.
- 8.
- 9.
- 10.
- 11.
What is a fibroid and what are its causes?
Fibroids are the most common benign tumors in women. Normally, they are presented in multiple forms, but we can also find them separately.
They may be asymptomatic, so their actual incidence is not precisely known. However, it is estimated that it occurs in 1 out of 4 women of childbearing age They are usually diagnosed between the ages of 30 and 40.
Its exact causes are unknown, but it is known that its appearance and growth are influenced by the hormones of the menstrual cycle, mainly by estrogens. A hormonal imbalance and increased level of estrogen in the body can lead to the appearance of this type of tumor, which is nothing more than the growth of an abnormal mass of muscle tissue.
After menopause, because estrogen levels in the blood decrease, new fibroids do not form and present fibroids usually decrease in size, although they do not disappear.
Some studies have also shown that fibroids may have genetic causes, so there is a certain genetic predisposition to develop them.
Types of uterine fibroids
All fibroids originate from the myometrium. However, three types of fibroids are distinguished depending on where they are and the direction in which they grow:
- Subserosals
- grow into the abdominal cavity. They can compress adjacent organs if they develop a lot, but they are usually asymptomatic. They are the most common (55%).
- Intramurals
- are kept in the thickness of the myometrium. They proliferate in the central portion of the myometrium and increase the size of the uterus. They are also frequent (40%).
- Submucous
- grow into the uterine cavity. They are less frequent (5%), but they cause more symptoms, as they increase menstrual bleeding (hypermenorrhea) and can cause iron-deficiency anemia. They have a better chance of becoming malignant.
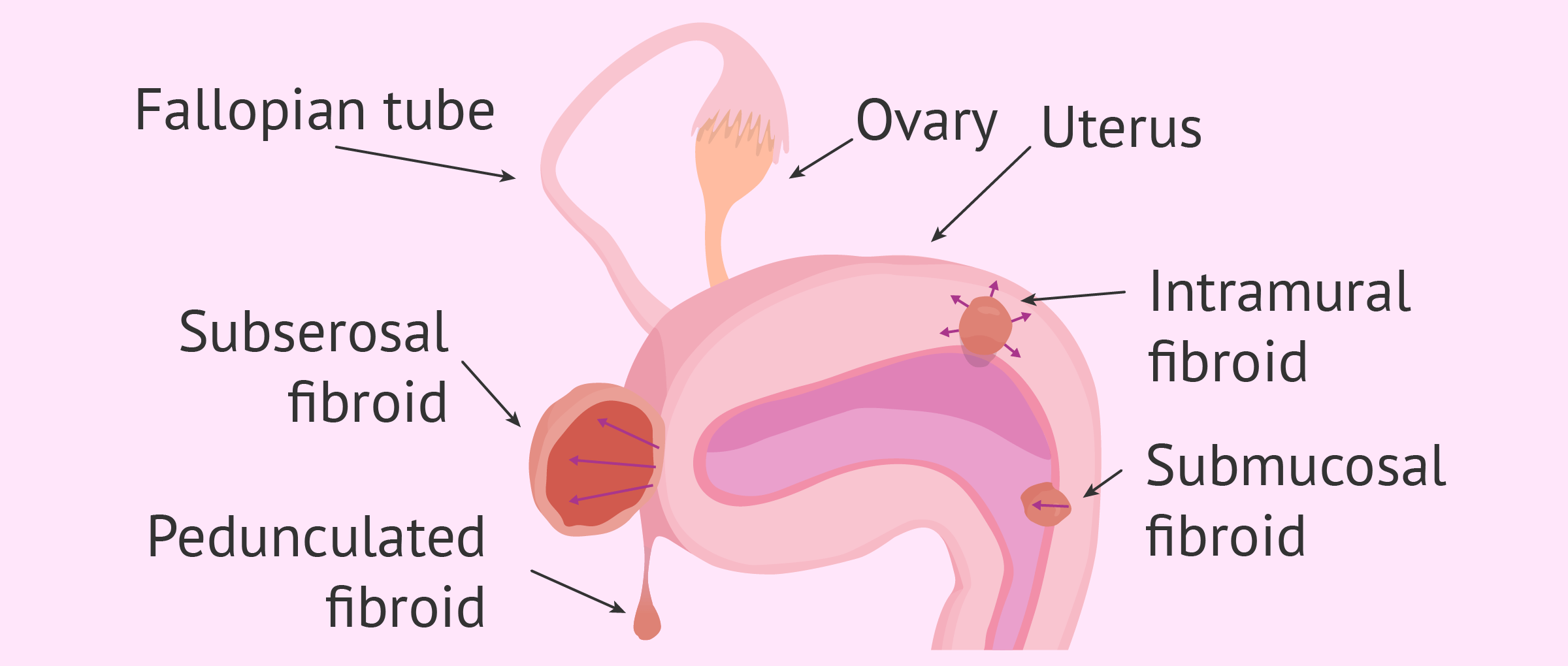
In addition, subserosal and submucosal fibroids can become pediculated, which means that they are only attached to the uterus by a fine stem called a pedicle. If it is twisted, it can cause sharp pain.
Symptoms of uterine myomatosis
As mentioned above, fibromyomas often do not cause any symptoms. However, in some women, depending on the location, size, and direction of tumor growth, they can cause:
- Bleeding between periods (metrorrhagia)
- Longer and heavier menstruation (menorrhagia)
- Painful periods (dysmenorrhea)
- Painful intercourse (dyspareunia)
- Pelvic pain and abdominal swelling
- Compression and pressure sensation in bladder, ureter, and rectum
- Increased urge to urinate
- Anemia

Other consequences of fibroids are fertility problems. The presence of fibroids is associated with an increased risk of miscarriages, premature contractions, etc.
How are fibroids diagnosed?
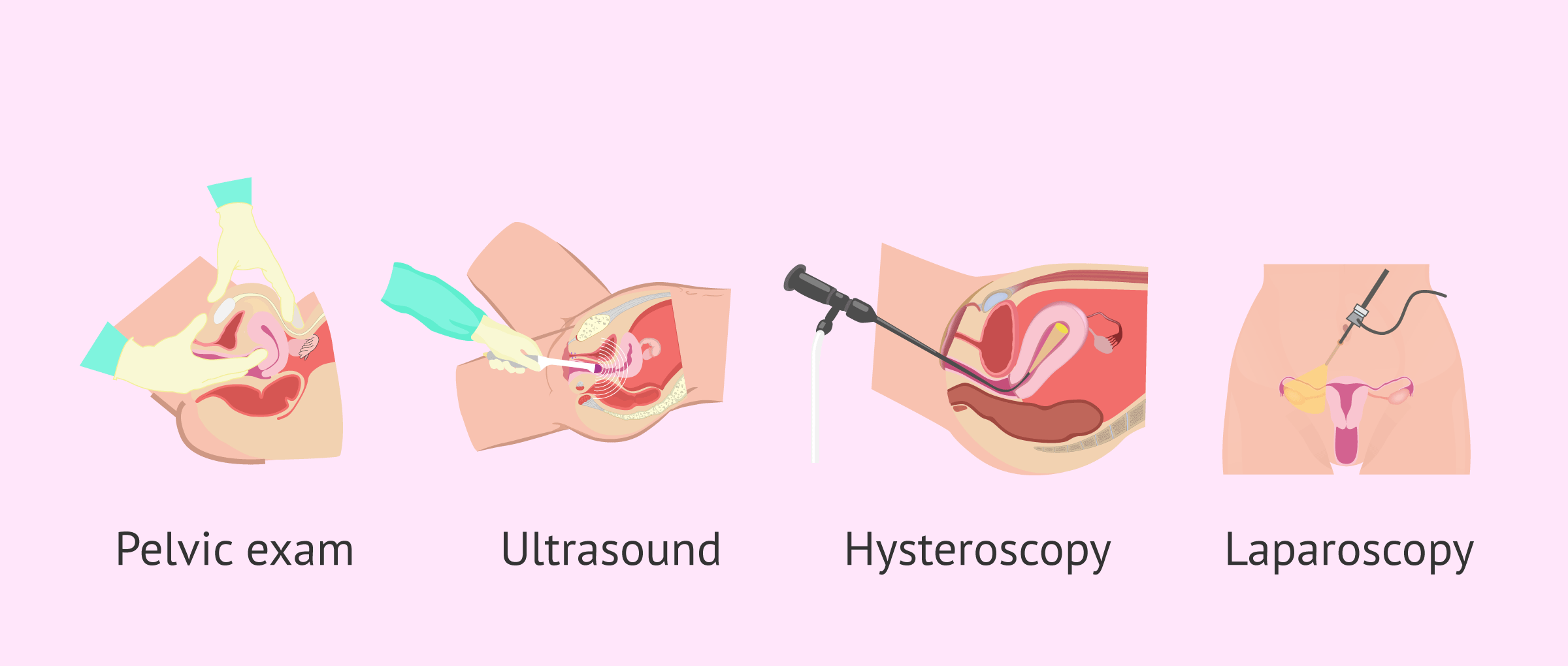
The diagnosis of fibroids is usually made by physical examination of the pelvic area, followed by abdominal or transvaginal ultrasound to confirm their presence. Diagnosis is more difficult in patients with obesity, as it requires more effort to palpate.
More complex techniques may also be used to confirm the diagnosis and rule out other types of alterations such as ovarian tumors or inflammation of the tubes:
- Hysteroscopy
- involves inserting a camera through the vagina to inspect the inside of the uterine cavity. It is useful for the diagnosis and extraction of submucosal fibroids.
- Laparoscopy
- a camera is inserted through a small hole in the abdomen to visualize the inside of the abdomen. It allows us to observe the subserosal fibroids and even extract them.
- Hysterosonography
- consists in performing an ultrasound while injecting a saline solution into the uterus to improve the visualization of the uterus.
- Magnetic Resonance
- allows you to create images using powerful magnets and radio waves. It is not usually done routinely because of its price.
- Computerized axial tomography (CAT)
- involves taking many x-rays to get a 3D image of the pelvic area. This technique is not widely used to diagnose fibroids, either.
- Endometrial biopsy
- by taking a tissue sample, allows malignant tumors to be diagnosed.
In any case, the medical specialist will be in charge of assessing which test(s) are necessary based on your suspicions.
Treatment
The treatment of myomatosis will depend on the age of the patient and her desire to have children, as well as the size and weight of the fibroids. Those that are asymptomatic and small in size have no need to be treated, only reviewed.
Non-invasive treatments
They allow you to delay or avoid surgery. Of the most common are:
- Analgesics
- to control the pain of small fibroids.
- Hormonal contraceptives
- to regulate menstrual periods and the pains they cause.
- Hormonal treatment with GnRH agonists
- reduces the level of estrogen in the blood causing a situation similar to menopause, so it is necessary to take into account its side effects. The treatment improves the symptoms but does not make the fibroid disappear, so when the medication is stopped, it grows back.

Invasive treatments
In cases in which the symptoms cannot be cured by means of drugs, surgical treatment is chosen. There are several options:
- Uterine Artery Embolization
- is used for small fibroids and consists of stopping the blood flow of the fibroid causing it to reduce its size or disappear completely. This is achieved by introducing microparticles into the uterine arteries via a catheter.
- Myomectomy
- is the removal of fibroids preserving the uterus. This technique is used by women who intend to have children. It doesn't guarantee that they won't grow fibroids again in the future. It can be performed by hysteroscopy (submucosal fibroids) or laparoscopy (subserosal fibroids).
- Hysterectomy
- is the partial or total removal of the uterus. This surgery is performed on older women who no longer intend to have children.

Rarely, morcellation is performed, i.e. cutting the fibroma into small pieces to be removed laparoscopically.
Affects on fertility and pregnancy
The presence of uterine fibroids has been related to female infertility, although only 1-2.4% of infertile patients present uterine fibroids as the sole cause of the sterility problem. Those that can make pregnancy more difficult are the submucosal ones, since they directly affect the uterine cavity.
One of the problems caused by fibroids is that they can oppress the fallopian tubes, which prevents fertilization of the egg. They may also prevent implantation in the endometrium.
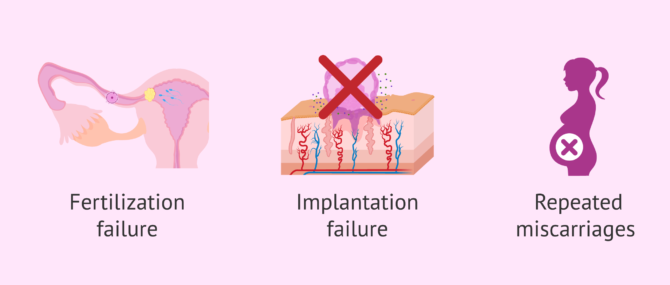
Besides, these tumors have been related to repeated miscarriages, since, depending on the size they have in the uterus, they can impede the normal development of the embryo.
Patients of childbearing age who believe that these alterations may make pregnancy more difficult should undergo a myomectomy.
If you want more information related to this topic, we recommend you to visit the following article: Do fibroids affect fertility and IVF outcome?
FAQs from users
What is the best treatment for myomatosis if I want to have children later?
In reproductive medicine a conservative approach is usually taken with fibroids, but the first thing is to know what size they are and whether or not they invade the uterine cavity.
How big are fibroids?
Fibroids can have very different sizes. To see some of them, it is necessary to use a microscope, while others are so large that they can occupy the entire uterine cavity. Depending on their size and location, they may cause more or less symptoms.
Can uterine fibroids become cancerous?
Yes, some fibroids can turn into malignant tumors, but it is very rare, as only 0.5% do. These tumors are called leiomyosarcomas.
Is there a natural treatment for uterine myomatosis?
Some of the home remedies that have been suggested to cure uterine fibroids are taking castor oil, dandelion, milk thistle, ginger or beet juice and carrot, among other things.
However, there are no scientific studies confirming the effectiveness of these natural medicine treatments. Therefore, if you have a myomatous uterus and you present symptoms, it is recommended that you resort to conventional medical treatments.
What is an intramural fibroid?
Intramural fibroids are a type of benign tumor characterized by being located in the most central part of the myometrium. This type of myoma does not reach either the internal or external area of the uterus.
Suggested for you
As we have seen, fibroids can make it difficult to achieve pregnancy, as they prevent the implantation of the embryo in the endometrium, i.e. they affect uterine receptivity. If you want to know more about this topic, we recommend you read the following post: Uterine receptivity as a cause of infertility.
However, there are other alterations in the uterus that can also affect female fertility. We tell you what they are in this article: Uterine Factor Infertility- Diagnosis, Characteristics & Treatment
If you are thinking about having children and you have any of these alterations, you can see how they influence the achievement of pregnancy through a series of tests. In this article we explain them to you: Female fertility tests.
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Bénilde Marie-Ange Tiemtoré-Kambou, Adama Baguiya, Prosper David Lamien, Adjiratou Koama, Aischa Madina Napon, Yomboué Abel Bamouni, Ousséini Diallo, Adama Gnoumou, Cissé Rabiou. Myoma, fortuitous discovery or metrorrhagia: Which is more revealing? Pan Afr Med J. 2021 Apr 20;38:388. doi: 10.11604/pamj.2021.38.388.20314 (View)
Kobra Tahermanesh, Soheil Hanjani, Roya Shahriyari, Abbas Fazel Anvari-Yazdi, Leila Allahqoli, Ibrahim Alkatout. The Blooming phenomenon: a rarity, but a dilemma in hysteroscopic resection of myomas. J Turk Ger Gynecol Assoc. 2022 Mar 8;23(1):63-67. doi: 10.4274/jtgga.galenos.2021.2021.0006 (View)
Sa Ra Lee, Ju Hee Kim, Sehee Kim, Sung Hoon Kim, Hee Dong Chae. The Number of Myomas Is the Most Important Risk Factor for Blood Loss and Total Operation Time in Robotic Myomectomy: Analysis of 242 Cases. J Clin Med. 2021 Jun 30;10(13):2930. doi: 10.3390/jcm10132930 (View)
YanZhen Peng, JiuMei Cheng, ChunYi Zang, Xi Chen, JinXue Wang. Comparison of Laparoscopic Myomectomy with and without Uterine Artery Occlusion in Treatment of Symptomatic Multiple Myomas. Int J Gen Med
. 2021 May 5;14:1719-1725. doi: 10.2147/IJGM.S310864
FAQs from users: 'What is the best treatment for myomatosis if I want to have children later?', 'How big are fibroids?', 'Can uterine fibroids become cancerous?', 'Is there a natural treatment for uterine myomatosis?' and 'What is an intramural fibroid?'.




