The presence of uterine fibroids can affect a woman's fertility and her ability to carry a pregnancy to term. However, this will depend, above all, on the type of myoma, its size, and the effect it has on the uterine cavity.
Therefore, not all fibroids are removed before starting assisted reproduction treatment. However, there will be cases in which removal of fibroids will be recommended to increase success rates.
Provided below is an index with the 9 points we are going to expand on in this article.
- 1.
- 2.
- 3.
- 4.
- 5.
- 5.1.
- 5.2.
- 5.3.
- 5.4.
- 6.
- 7.
- 8.
- 9.
What are uterine fibroids?
Myomas, leiomyomas, or uterine fibroids are benign growths or tumors of the uterine wall, specifically of the smooth muscle layer (myometrium). These can present in a single or multiple forms and their size is variable, as well as their symptomatology. While many fibroids are asymptomatic, others may produce symptoms such as bleeding, pressure sensation, and pain.
On the other hand, it is important to consider where the fibroids are located and their direction of growth. According to these criteria, fibroids can be:
- Submucosal. The myoma grows towards the interior of the uterine cavity.
- Intramurals. In this case, the myoma grows inside the uterine wall.
- Subserosal. Myoma growth is outward.

Thus, not all leiomyomas will have the same impact on a woman's fertility when seeking pregnancy.
Do uterine fibroids affect fertility?
One of the main concerns a woman of reproductive age may have when uterine fibroids are detected is whether or not she will be able to become pregnant. First of all, women should know that the existence of uterine fibroids does not always prevent them from achieving pregnancy, even in a natural way.
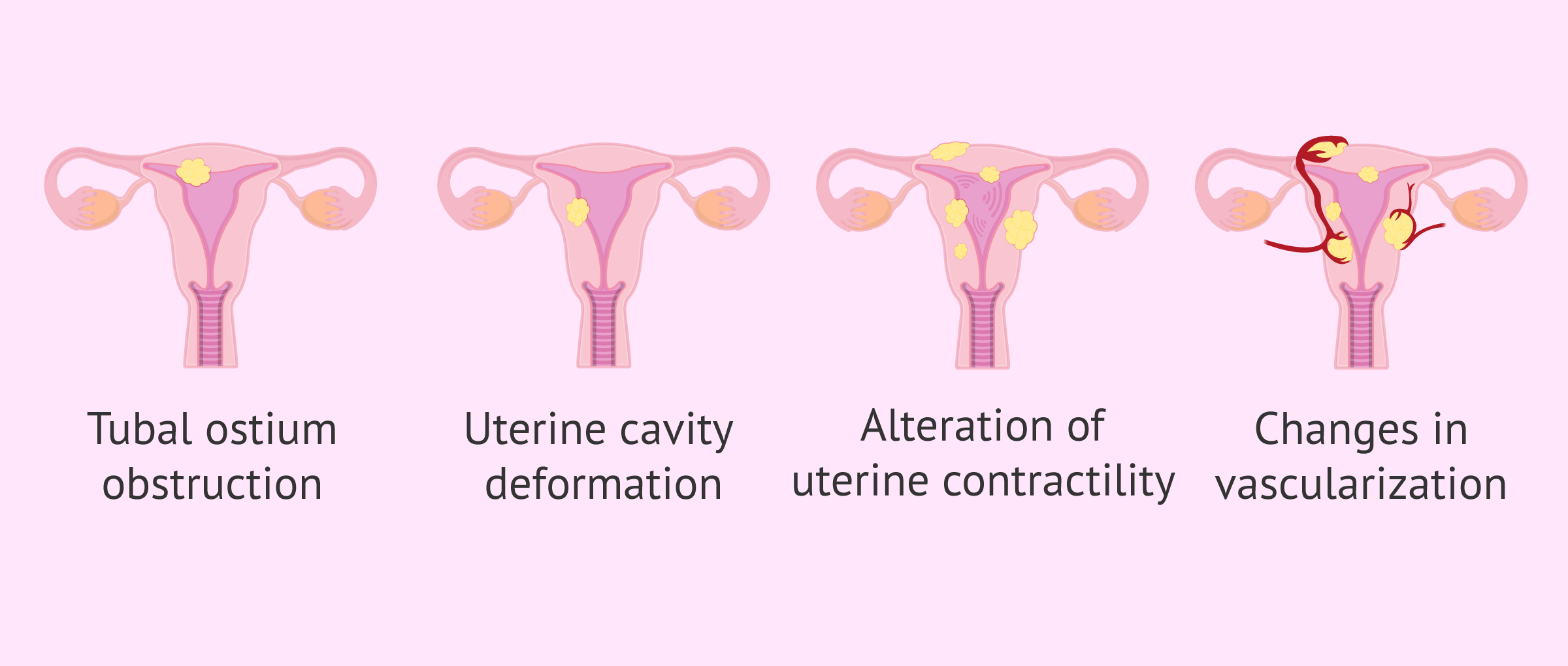
However, a fibroid can alter a woman's fertility due to one or even several of the factors mentioned below:
- Obstruction of the sperm's path through the uterus to the fallopian tubes, which hinders fertilization from occurring. There may even be a blockage of the tubal ostium, that is, the orifices that connect the uterus with the tubes.
- Modification or deformation of the uterine cavity.
- Alteration in the contractility of the uterus.
- Changes in vascularization and blood flow.
Therefore, fertilization and embryo implantation could be hindered in some women with fibroids and, consequently, the achievement of pregnancy. In general, submucous fibroids are the most frequently associated with impairment of reproductive capacity.
Myomas and in vitro fertilization (IVF)
Not all fibroids are removed prior to fertility treatment. Nevertheless, fibroids are usually removed in the following situations:
- They alter the uterine cavity.
- They are large in size.
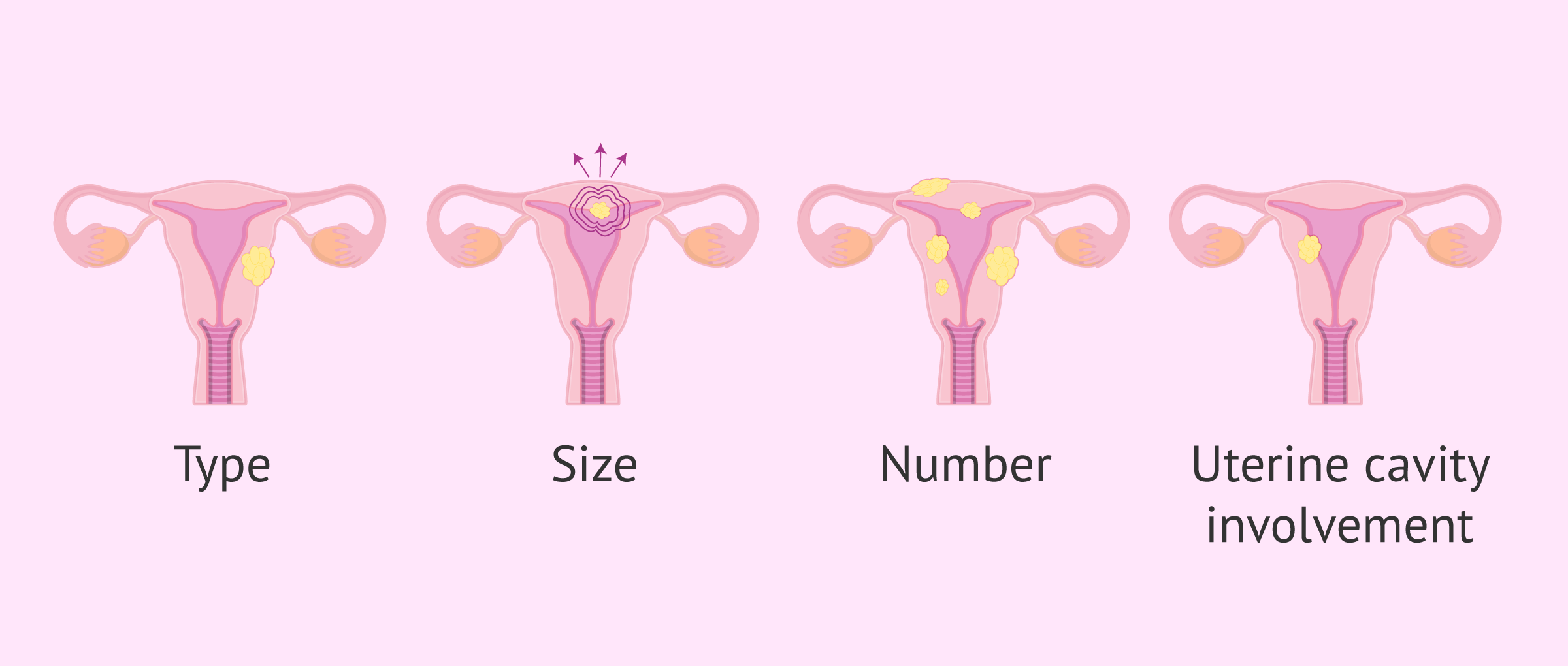
Therefore, the specialist must evaluate the situation on a personalized basis, check what type of myoma the woman has, its size, number, and whether or not the uterine cavity is affected.
Submucosal fibroids have been more clearly associated with impairment of fertility and IVF cycle outcomes, so they are usually removed. However, subserosal fibroids do not seem to have much impact when seeking pregnancy naturally or by assisted reproductive techniques (ART).
Intramural fibroids affecting the uterine cavity would have a similar effect to submucosal fibroids. In contrast, the influence on female fertility and ART outcomes of intramural fibroids that do not alter the cavity is less clear, although some studies point to a deterioration in IVF cycle outcomes.
Thus, removal of certain fibroids may be advisable before seeking ART pregnancy. This is intended to improve uterine conditions, in an attempt to increase the probability of success.
How are fibroids removed?
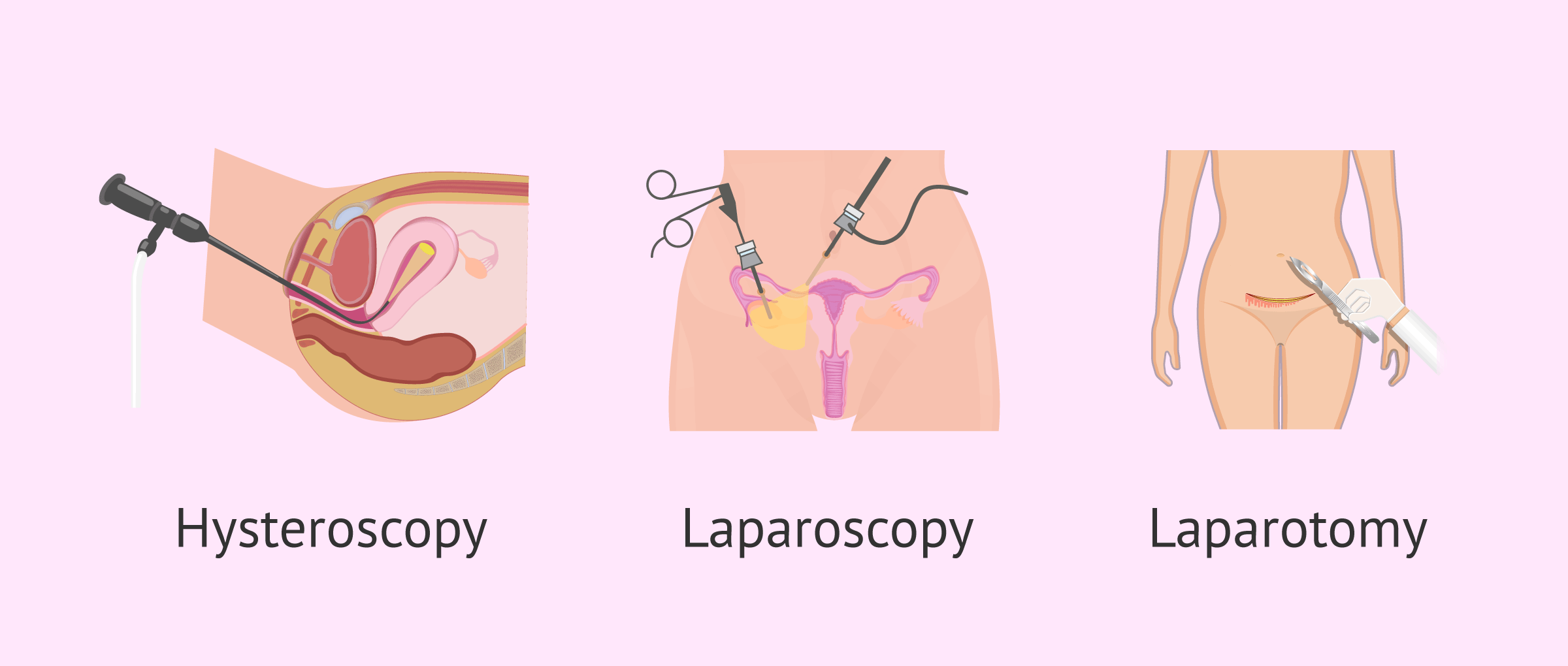
The surgical removal of uterine fibroids is called myomectomy myomectomy. The approach may be by laparotomy, laparoscopy, or hysteroscopy, depending, above all, on the location and size of the fibroids.
For submucosal myomas, myomectomy will generally be performed hysteroscopically. In the case of intramural and subserosal fibroids, the intervention will be performed by laparoscopy or laparotomy.
Of course, the gynecologist will indicate to the patient how long she should wait to seek pregnancy (naturally or by assisted reproduction) after the myomectomy. In addition, there are other treatment options for fibroids such as uterine artery embolization or radiofrequency ablation.
On the other hand, a more radical alternative is to perform a hysterectomy (removal of the uterus). However, this approach to fibroids assumes that the patient is no longer able to gestate. Therefore, whenever possible, hysterectomy should be avoided and more conservative treatment should be attempted if the woman wishes to become a mother. However, this option has usually been used if the woman has already fulfilled her gestational desire.
FAQs from users
Is it better to do uterine artery embolization or myomectomy before IVF?
Currently, both techniques are valid and some studies show similar subsequent pregnancy rates.
The choice of one technique or the other will depend on the specialist, experience, and especially on the size, number, and position of the myoma. Therefore, each case must be individualized with your doctor.
Read more
Can fibroids be the cause of a negative IVF?
Yes, the presence of uterine fibroids can lead to an impairment of fertility in women, due to several factors that could alter endometrial receptivity and embryo implantation.
However, submucous fibroids are the ones that have been most closely related to adverse IVF results, which is why their removal is usually performed prior to fertility treatment, with the intention of improving the probability of pregnancy.
Can I get pregnant by IVF with a subserosal myoma?
Yes, subserosal fibroids grow outside the uterus and appear to have little effect on a woman's fertility or the results of fertility treatments.
For this reason, subserosal fibroids are not usually removed prior to fertility treatment as long as they do not bother the woman because of their symptoms or are not too large. However, it will be the specialist who will assess the particular situation of the patient prior to IVF treatment.
Is a pregnancy with fibroids more risky?
Yes, when a woman with uterine fibroids becomes pregnant, the size of the fibroids may increase during the first trimester of pregnancy. However, this does not occur in all cases.
In addition, fibroids may lead to an increased risk of certain obstetric complications.
Read more
Recommended readings
For more detailed information about fibroids, we recommend reading the following article: Uterine fibroids: types, symptoms, diagnosis, and treatments.
On the other hand, in this article, we have discussed how different types of fibroids affect the results of IVF cycles. If you are interested in learning more about this assisted reproduction technique, you can access the following link: In vitro fertilization (IVF): What is it and how much does it cost?
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Bosteels J, van Wessel S, Weyers S, Broekmans FJ, D'Hooghe TM, Bongers MY, Mol BWJ. Hysteroscopy for treating subfertility associated with suspected major uterine cavity abnormalities. Cochrane Database Syst Rev. 2018 Dec 5;12(12):CD009461. (See)
DE Angelis MC, DI Spiezio Sardo A, Carugno J, Manzi A, Sorrentino F, Nappi L. Fertility outcomes after hysteroscopic removal of intrauterine leiomyomas and polyps. Minerva Obstet Gynecol. 2022 Feb;74(1):3-11. (See)
Di Spiezio Sardo A, Di Carlo C, Minozzi S, Spinelli M, Pistotti V, Alviggi C, De Placido G, Nappi C, Bifulco G. Efficacy of hysteroscopy in improving reproductive outcomes of infertile couples: a systematic review and meta-analysis. Hum Reprod Update. 2016 Jun;22(4):479-96. (See)
Dubuisson J. The current place of mini-invasive surgery in uterine leiomyoma management. J Gynecol Obstet Hum Reprod. 2019 Feb;48(2):77-81. (See)
Levy G, Hill MJ, Beall S, Zarek SM, Segars JH, Catherino WH. Leiomyoma: genetics, assisted reproduction, pregnancy and therapeutic advances. J Assist Reprod Genet. 2012 Aug;29(8):703-12. (See)
Loddo A, Djokovic D, Drizi A, De Vree BP, Sedrati A, van Herendael BJ. Hysteroscopic myomectomy: The guidelines of the International Society for Gynecologic Endoscopy (ISGE). Eur J Obstet Gynecol Reprod Biol. 2022 Jan;268:121-128. (See)
Metwally M, Raybould G, Cheong YC, Horne AW. Surgical treatment of fibroids for subfertility. Cochrane Database Syst Rev. 2020 Jan 29;1(1):CD003857. (See)
Rakotomahenina H, Rajaonarison J, Wong L, Brun JL. Myomectomy: technique and current indications. Minerva Ginecol. 2017 Aug;69(4):357-369. (See)
Rikhraj K, Tan J, Taskin O, Albert AY, Yong P, Bedaiwy MA. The Impact of Noncavity-Distorting Intramural Fibroids on Live Birth Rate in In Vitro Fertilization Cycles: A Systematic Review and Meta-Analysis. J Womens Health (Larchmt). 2020 Feb;29(2):210-219. (See)
Siristatidis C, Vaidakis D, Rigos I, Chrelias G, Papantoniou N. Leiomyomas and infertility. Minerva Ginecol. 2016 Jun;68(3):283-96. (See)
Stewart EA, Laughlin-Tommaso SK, Catherino WH, Lalitkumar S, Gupta D, Vollenhoven B. Uterine fibroids. Nat Rev Dis Primers. 2016 Jun 23;2:16043. (See)
Stewart EA, Nowak RA. Uterine Fibroids: Hiding in Plain Sight. Physiology (Bethesda). 2022 Jan 1;37(1):16-27. (See)
Sunkara SK, Khairy M, El-Toukhy T, Khalaf Y, Coomarasamy A. The effect of intramural fibroids without uterine cavity involvement on the outcome of IVF treatment: a systematic review and meta-analysis. Hum Reprod. 2010 Feb;25(2):418-29. (See)
Wang X, Chen L, Wang H, Li Q, Liu X, Qi H. The Impact of Noncavity-Distorting Intramural Fibroids on the Efficacy of In Vitro Fertilization-Embryo Transfer: An Updated Meta-Analysis. Biomed Res Int. 2018 Sep 4;2018:8924703. (See)
FAQs from users: 'Is it better to do uterine artery embolization or myomectomy before IVF?', 'Can fibroids be the cause of a negative IVF?', 'Can I get pregnant by IVF with a subserosal myoma?' and 'Is a pregnancy with fibroids more risky?'.
Authors and contributors




More information about Cristina Algarra Goosman

Hi, I have had several fibroids throughout my life but have never been offered surgical resection. I wonder if I will be able to get pregnant with this problem.
Hello Phalm,
The presence of uterine fibroids does not consequently mean that there is an affection to the reproductive capacity. It will depend on the location of the fibroid, the type, size, and number of fibroids present in the uterus.
I recommend that you see your doctor so that he/she can assess whether or not the fibroids you have are compatible with pregnancy.
I hope I have helped you,
Best regards.
Hello, I have very strong pains when I have my period and I don’t know what the reason could be, is it possible that I have a fibroid?
Hi Kenedee,
Pain during menstruation can have several causes, one of them being the presence of fibroids. If you have heavy periods or pain that prevents you from leading a normal life when you are on your period I recommend that you go to your doctor so he can assess whether there is some kind of pathology that is causing the pain.
I recommend you to read the following article where you will find the characteristics and treatment of menstrual pain: Painful Menstruation.
I hope I have helped you,
Best regards