Endometrial or uterine receptivity is defined as the ability of the uterus to allow an embryo to implant and begin gestation.
Thanks to advances in assisted reproduction and, above all, in vitro fertilization (IVF) treatment, it has been possible to study in greater depth the role of the endometrium and its implication in reproductive success.
Alterations in endometrial receptivity, therefore, are a cause of female sterility, since they lead to suffering the so-called repeated implementation failures.
Provided below is an index with the 8 points we are going to expand on in this article.
- 1.
- 1.1.
- 2.
- 2.1.
- 2.2.
- 3.
- 4.
- 4.1.
- 4.2.
- 4.3.
- 4.4.
- 4.5.
- 5.
- 6.
- 7.
- 8.
What is endometrial receptivity?
The endometrium is the internal tissue of the uterus, whose main function is the interaction with the embryo to achieve its implantation and consequently an evolutionary gestation.
This tissue is highly dynamic and undergoes multiple changes throughout the menstrual cycle, from preparing for implantation to evacuating through menstruation when pregnancy has not occurred, through hormonal regulation and adopting an immune function.

Within this context, uterine receptivity refers to a specific state of the endometrium in which its conditions are optimal for embryo implantation to occur.
Endometrial receptivity involves a series of molecular, structural and vascular changes in the inner layer of the uterus that will allow the nesting of the developing embryo.
It should be noted that the endometrium is only receptive to certain days of the menstrual cycle, exactly 6-7 days after ovulation. This is what is known as implantation window.
The importance of endometrial thickness
The classic way to assess uterine receptivity is by measuring endometrial thickness.
An optimal endometrium for implantation must measure between 7-10 mm and have a trilaminar aspect. Endometrios with a thickness inferior to 7 mm and superior to 13 mm have demonstrated to have a smaller rate of gestation.
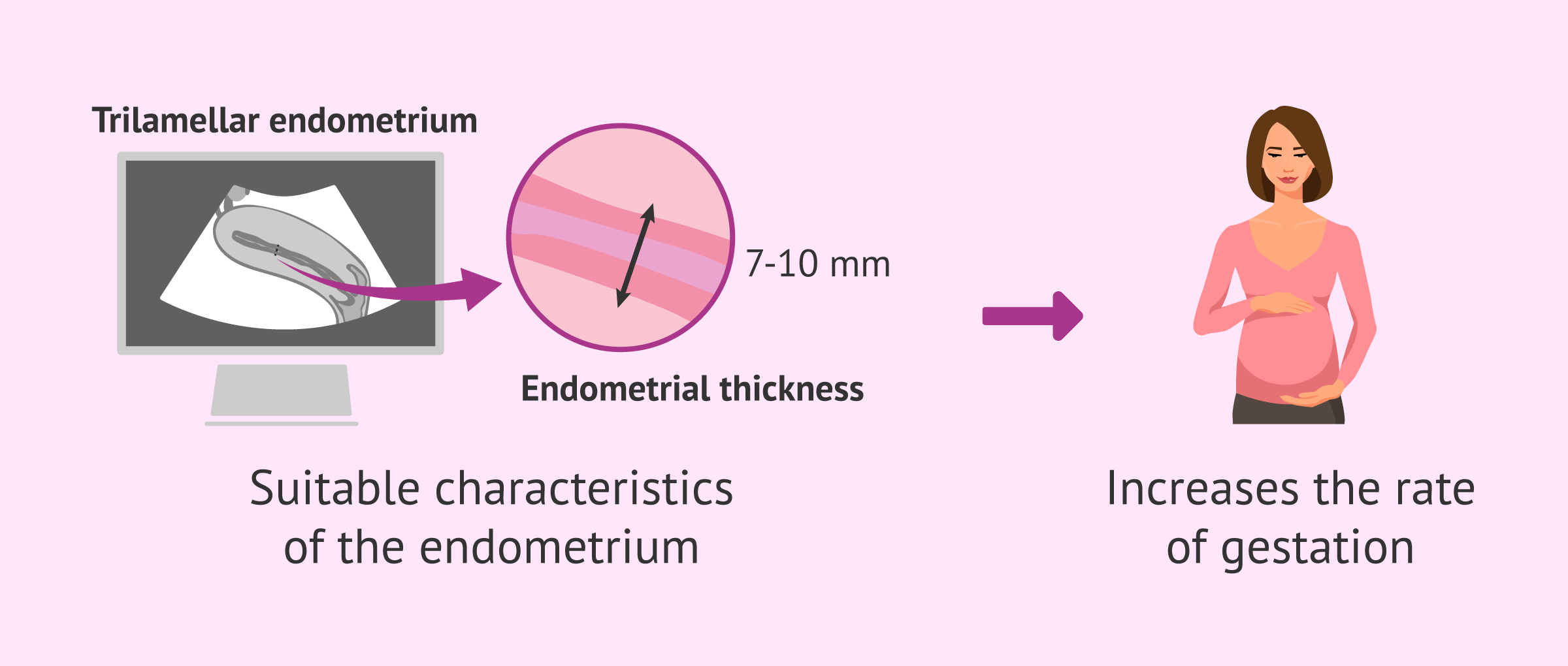
For all these reasons, ultrasound is an essential test to determine whether the uterus is ready for embryo implantation, something that must always be proven in any assisted reproduction treatment.
Low endometrial receptivity
Sometimes, when the endometrium is analyzed with ultrasound, it is verified that it does not have the adequate thickness or, even if it has the correct aspect and good quality embryos, the patient does not manage to get pregnant.
This is when the specialist must begin to pay attention to the receptivity of the uterus, as there are several causes that may be affecting it and, depending on each case, additional diagnostic tests may be indicated.
Causes
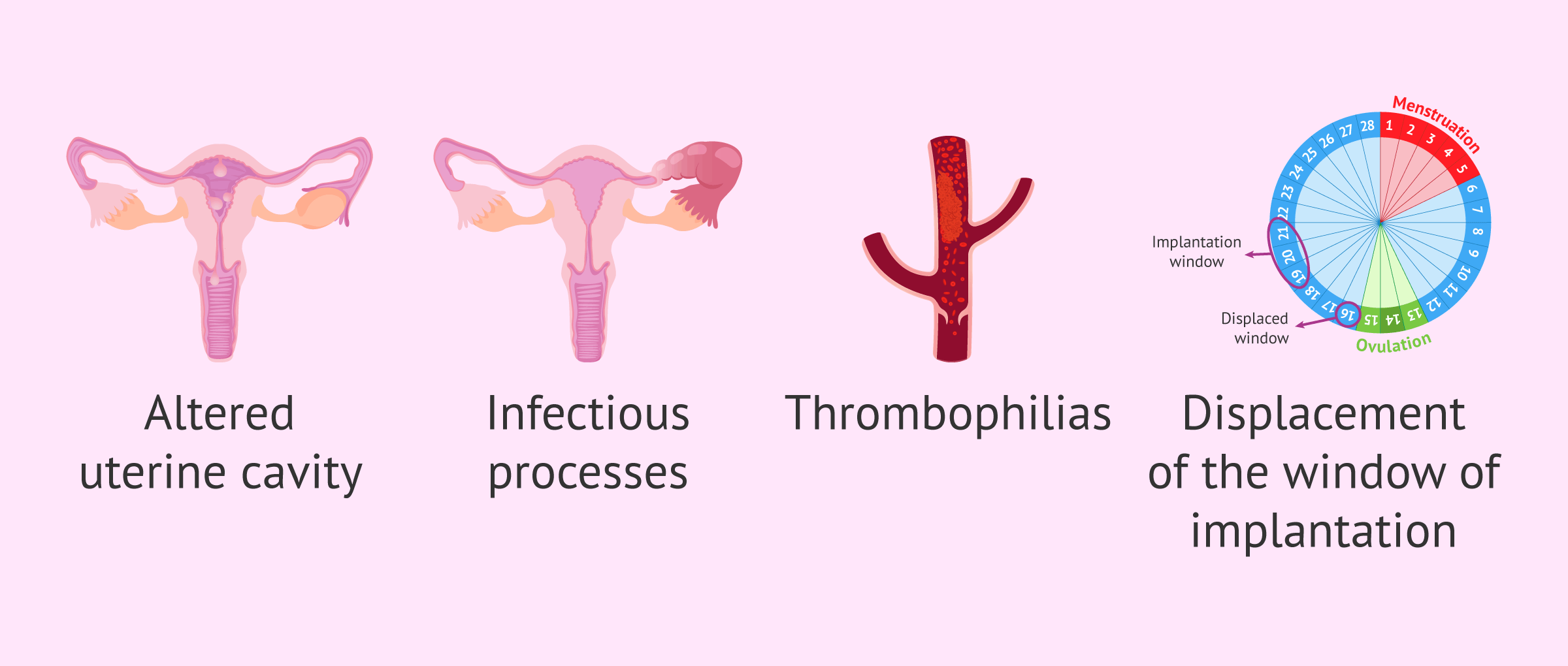
The causes of low endometrial receptivity are many and varied, with the involvement of various pathophysiological mechanisms:
- Abnormalities in the uterine cavity: polyps, partitions, myomas, synechiae, etc.
- Infectious or inflammatory processes: endometritis, hydrosalpinx.
- Deficit in endometrial proliferation: thin endometrium without sufficient thickness for embryo implantation. This is known as refractory endometrium.
- Alterations of the coagulation system (thrombophilias).
- Displacement of the implantation window.
- Chromosomal Alterations
- Systemic immunological diseases.
- Local immunological processes: in the endometrium there must be an environment of immune tolerance so that the embryo is not rejected by the mother, which is conditioned by genetic, epigenetic and environmental factors.
- Microbiota alterations: microorganisms such as bacteria, fungi, and/or viruses that establish a "biofilm" inside the uterus.
- Incompatibility of "dialogue" between embryo and endometrium: implies morphological and functional changes (genomic and/or molecular in the endometrium before the arrival of the embryo).

Occasionally, several factors cause low uterine receptivity or the cause may not yet be known, leading to the diagnosis unexplained infertility.
Endometrial testing
As we have already mentioned, the classical endometrial evaluation has been carried out by ultrasound and also hysteroscopy, histology and immunology analysis. However, today there are newer and more specific techniques that allow a more advanced study of the endometrium. That’s what’s known as genomic testingas they study the receptivity of the endometrium at the level of genes and their expression.
One of the most important tests for analyzing endometrial receptivity is the Endometrial Receptivity Array (ERA) test. This is a molecular test that studies the expression of 248 genes associated with the receptive state of the endometrium. This makes it possible to determine whether the endometrium is receptive at a specific time in the menstrual cycle or whether the implantation window is displaced.
Molecular biology, through RNA and transcriptomics and secretomics, has allowed us to deepen the endometrial receptivity and the adjustment of the embryo implantation window.
On the other hand, there are also analyses of the endometrial microbiota with the aim of getting to know the intrauterine microflora in greater depth and treating its imbalances prior to the treatments. They're called EMMA test and ALICE test.

The endometrium still hides great discoveries for scientists, and maximizing their knowledge will allow us to achieve better results in assisted reproduction techniques.
How to get pregnant?
Once uterine receptivity has been analyzed and, depending on whether it has been possible to identify the exact cause of having a nonreceptive endometrium, various strategies can be carried out to try to achieve gestation. We will discuss them below:
- If you have a displaced implantation window identified by the ERA test, you should schedule the embryo transfer at another point in the menstrual cycle where the endometrium is shown to be receptive.
- If the patient suffers from endometritis or any other infection in the reproductive tract, she must carry out a specific treatment with antibiotics before attempting a new pregnancy. The EMMA and ALICE tests identify the microorganisms responsible for the infection and determine which antibiotic is adequate to combat them.
- Treatment with aspirin and/or heparin in case of diagnosis of thrombophilia.
- Treatment with corticoids or immunoglobulins in case of immune rejection of the embryo.
- In the case of a refractory endometrium incapable of proliferating with estrogens and progesterone, drugs that favour blood supply to the endometrium, such as sildenafil, pentoxifylline, vitamin A, vitamin E, etc., may be indicated.
- Evaluating endometrial scratching. This is a small surgical procedure to damage the endometrium and cause it to regenerate.

In short, in a case of repetitive implantation failure and an endometrium with little receptivity, it is very important to carry out an exhaustive study and to carry out all the necessary tests to approach an exact diagnosis that allows to establish the reproductive strategy.
Finally, it should be remembered that maintaining healthy lifestyle habits together with a healthy and balanced diet will always help to improve overall health and facilitate the onset of pregnancy.
FAQs from users
Why doesn't my endometrium grow yet on estrogen and progesterone?
We know that correct endometrial perfusion is key to the growth of the endometrium and therefore to correct embryo implantation. If there is no correct blood supply to the endometrium, even if we administer exogenous hormones, they will never reach it properly. This is the reason why we administer drugs that promote the arrival of blood to the endometrium (sildenafil, pentoxifylline, vitamin A, vitamin E ...) when we are faced with refractory endometrios to treatment with estrogens and progesterone (those that do not grow despite the correct hormone intake).
Can you use vaginal viagra as a treatment to increase uterine lining?
Viagra works by dilating the blood vessels to increase the blood supply to the penis. Some studies have suggested that viagra can also be used as a vasodilator to increase blood flow to the uterus and improve endometrial thickness.
Even though it is rather uncommon, some specialists prescribe vaginal pessaries with viagra as an active ingredient with the purpose of increasing endometrial thickness.
When does the endometrium become receptive?
The endometrium is receptive when the embryo can adhere to the endometrial cells and then be introduced into their thickness. Classically, this process was said to occur between days 20 and 24 of a normal 28-day cycle.
Read more
Do natural killer cells provoke implantation failures?
Yes, recent studies have shown that women with repeated implantation failure have a higher number of NK cells and this increase is more significant in the endometrium than in the woman's blood.
Is a thickened endometrium receptive?
Not necessarily. A receptive endometrium is one that has a thickness between 8-12 mm and a trilaminar aspect. An endometrial thickness greater than 13 mm is associated with a low implantation rate.
In addition, for an endometrium to be receptive it must have undergone several structural changes that can only be visualised after a biopsy and observation of the endometrial tissue under the microscope: presence of pinopods, endometrial glands, greater number of cells, etc.
Suggested for you
As we have said throughout the article, low uterine receptivity can lead the patient to suffer repeated implantation failures, something that takes a toll on her physical, emotional and economic state in fertility treatment. If you want to read more about this, we recommend you read on here: Repeated embryo implantation failures: Reasons why embryos don't implant.
On the other hand, there are some recommendations that women can follow in order to improve the state of their endometrium and encourage implantation. You can read them in the next post: 6 effective ways to increase endometrial thickness naturally.
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Casper RF. It's time to pay attention to the endometrium. Fertil Steril. 2011 Sep;96(3):519-21 (View)
D'Ippolito S, Di Nicuolo F, Pontecorvi A, Gratta M, Scambia G, Di Simone N. Endometrial microbes and microbiome: Recent insights on the inflammatory and immune "players" of the human endometrium. Am J Reprod Immunol. 2018 Dec;80(6):e13065 (View)
Kliman, H. J., & Frankfurter, D. (2019). Clinical approach to recurrent implantation failure: evidence-based evaluation of the endometrium. Fertility and Sterility, 111(4), 618–628 (View)
Lessey, B. A., & Young, S. L. (2019). What exactly is endometrial receptivity? Fertility and Sterility, 111(4), 611–617 (View)
Mariani G, Bellver J. Strategies to improve endometrial receptivity. Rev. Iberoam. Fert Rep Hum, 2017; 34; 9-20 (View)
Sociedad Española de Fertilidad. Guía 9. Bruna I, Morraja J, Collado O. Estudio del fallo repetido de implantación y sus posibles alternativas terapéuticas (View)
Speroff, L., & Fritz, M. A. (2005). Clinical Gynecologic Endocrinology and Infertility. Lippincott Williams & Wilkins (View)
FAQs from users: 'Why doesn't my endometrium grow yet on estrogen and progesterone?', 'Can you use vaginal viagra as a treatment to increase uterine lining?', 'When does the endometrium become receptive?', 'Do natural killer cells provoke implantation failures?' and 'Is a thickened endometrium receptive?'.
Authors and contributors





