The Fallopian tubes are structures of the female reproductive system that connect the ovaries to the uterus. Their function is to collect the ovum released by the ovary, allow the sperm and egg to meet resulting in fertilization, and the transport of the embryo to the uterus.
Therefore, any injury or obstruction of the Fallopian tubes, preventing their function, will be a cause of female sterility.
Today, in vitro fertilization (IVF) is the treatment of choice for women with tuboperitoneal factors. IVF doesn't require functional Fallopian tubes to be successful.
In the following video, embryologist Silvia Azaña explains what tubal factor is, its possible causes, how it is diagnosed, and what the most appropriate treatment is. However, you can later explore the topic in more detail by reading the article.
Provided below is an index with the 10 points we are going to expand on in this article.
- 1.
- 2.
- 2.1.
- 2.2.
- 2.3.
- 2.4.
- 3.
- 4.
- 4.1.
- 4.2.
- 5.
- 6.
- 6.1.
- 6.2.
- 6.3.
- 6.4.
- 6.5.
- 7.
- 8.
- 9.
- 10.
What is a tubal factor?
As previously mentioned, the fallopian tubes must be able to move and allow passage of the egg and / or embryo, and in order to carry out their function correctly. This is essential for pregnancy to occur naturally.
Tubal factor refers to alterations in the fallopian tubes that hinder or even prevent gestation. This type of alteration is an obstacle to achieving pregnancy in approximately 30% of patients with fertility problems.
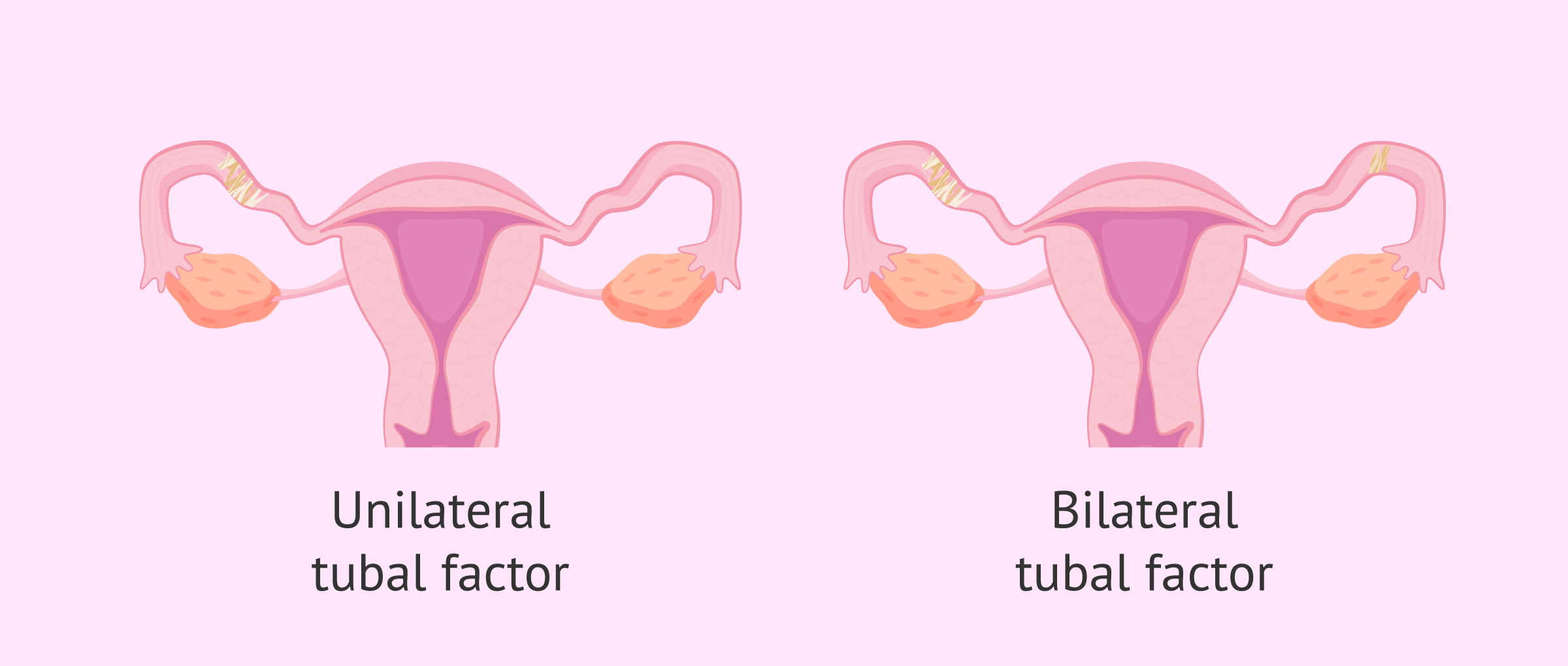
Sometimes, the woman only has a unilateral tubal factor, that is, one affected tube and one healthy tube. In this case, a natural pregnancy can occur, although the chances of achieving it may be reduced.
When the tubal factor is bilateral, both tubes are damaged and, therefore, natural pregnancy is not possible, since the encounter between egg and sperm is impeded. Therefore, a patient with bilateral tubal involvement will generally have to resort to assisted reproduction if she wishes to become a mother.
Assisted procreation, as any other medical treatment, requires that you rely on the professionalism of the doctors and staff of the clinic you choose. Obviously, each clinic is different. Get now your Fertility Report, which will select several clinics for you out of the pool of clinics that meet our strict quality criteria. Moreover, it will offer you a comparison between the fees and conditions each clinic offers in order for you to make a well informed choice.
Causes of tubal factor
Although sometimes unknown, problems with the fallopian tubes may be due to different causes. Below we will discuss the most important ones.
Pelvic infection
Pelvic infection is the most frequent cause of tubal injury. This type of infection can originate in the reproductive tract, in nearby sites such as the appendix, or from other infections, for example, tuberculosis.
The microorganisms responsible include Chlamydia trachomatis (chlamydia) and Neisseria gonorrhoeae (gonorrhea), both of which cause sexually transmitted diseases (STDs).
It is of crucial importance to be cautious with unprotected sex in order to avoid STDs.
If these microorganism infections are not treated properly and on time, the inflammatory process (pelvic inflammatory disease or PID) will trigger the appearance of adhesions that will affect tubal function.
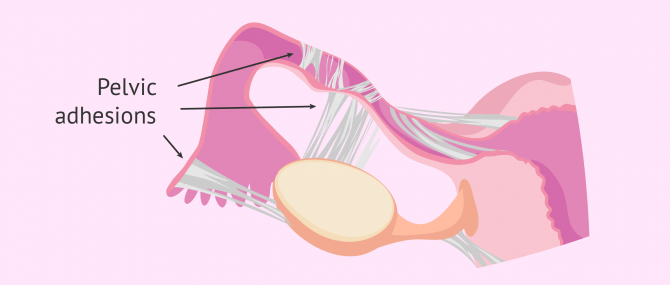
These adhesions are formed by the scar tissue that forms between the pelvic organs, causing them to stick to each other and lose their function.
Endometriosis
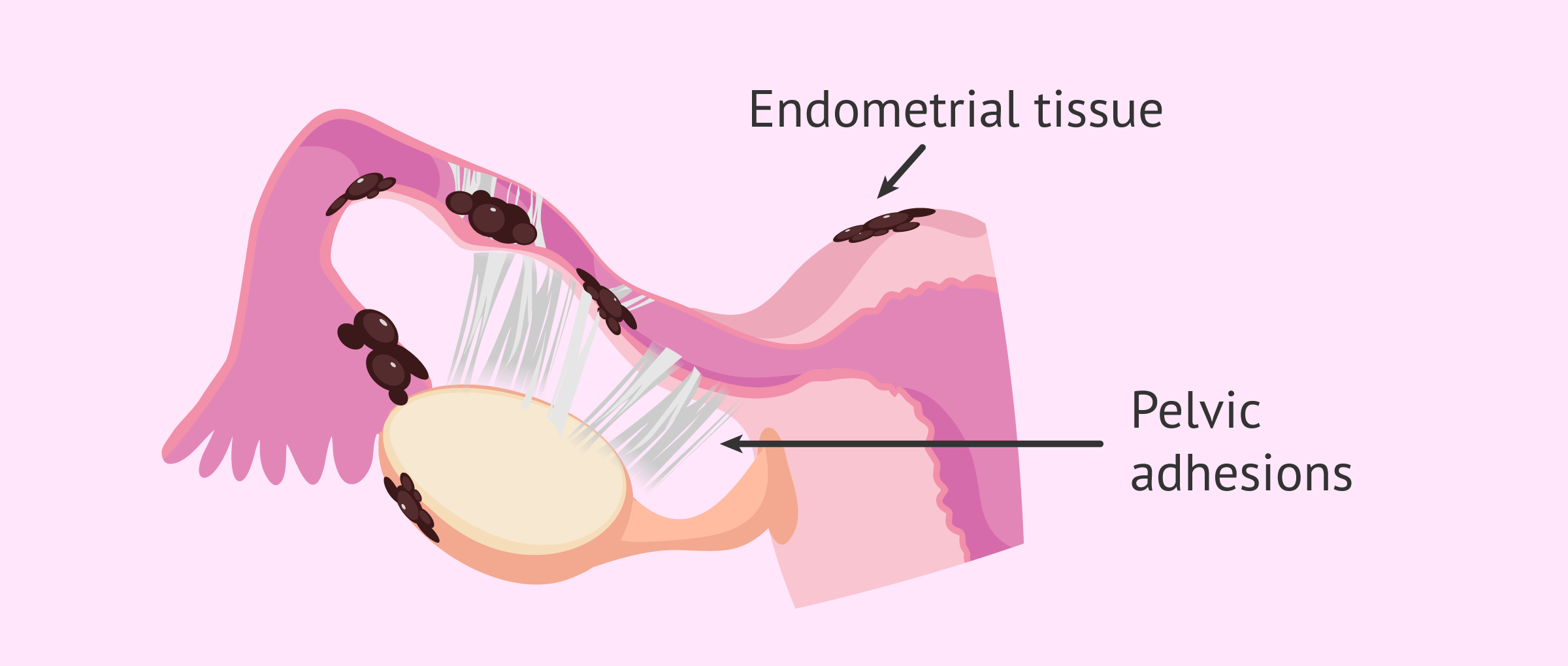
Endometriosis is a disease in which the endometrial tissue leaves the uterine cavity and implants in other locations, such as the fallopian tubes or ovaries.
Thus, endometriosis is another disorder that can cause tubal obstructions and, in addition, pelvic adhesions that hinder the mobility of the fallopian tubes.
If you want to read more about this pathology affecting women of reproductive age, you can read the following post: What Is Endometriosis? – Causes, Symptoms and Treatment
Hydrosalpinx
Hydrosalpinx is a disorder of the fallopian tubes characterized by an accumulation of fluid inside them. This causes the tube to dilate and become obstructed. The most common cause of hydrosalpinx is previous pelvic infection.
This condition, in addition to causing a blocked tube, can also affect the pregnancy rate after in vitro fertilization (IVF). The fluid that accumulates in hydrosalpinx can reach the uterus and affect embryo implantation.

You can learn more about this topic in the following post: What is hydrosalpinx? - Causes, symptoms and treatment
Other factors
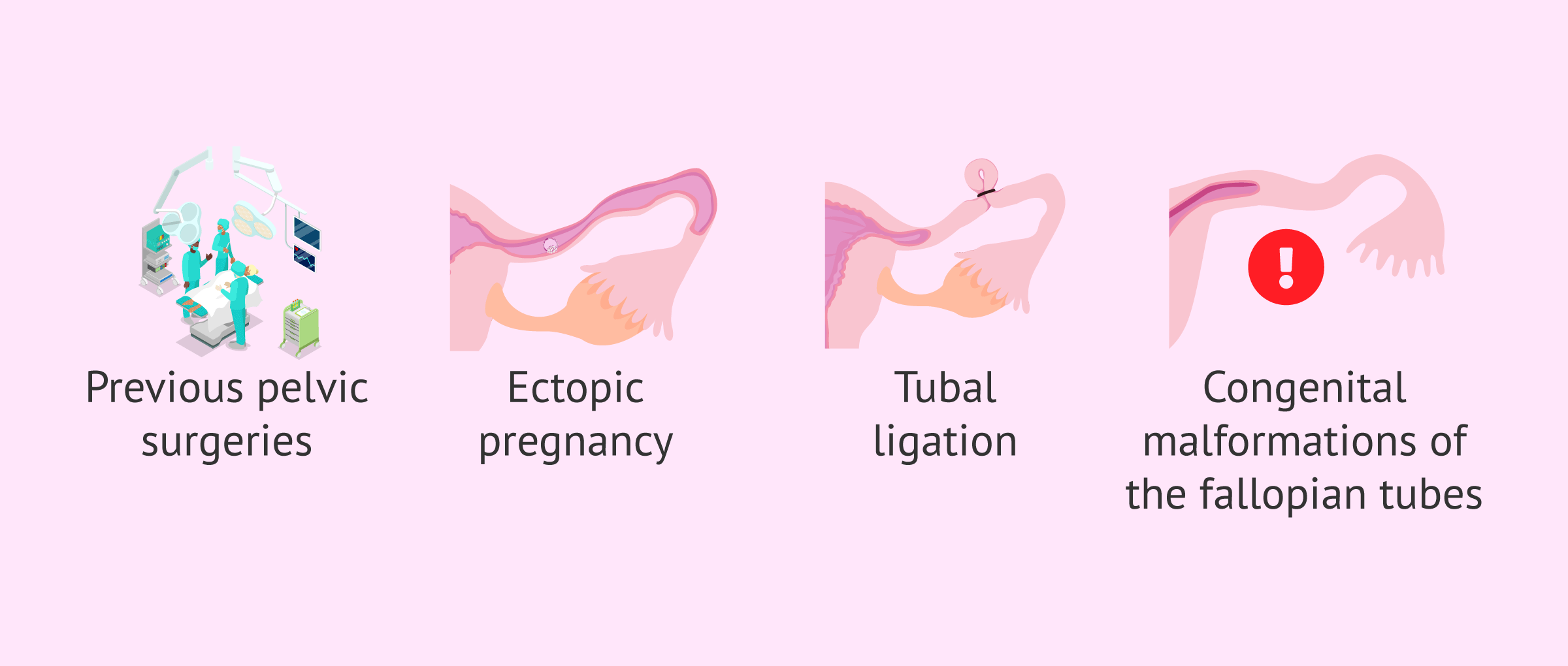
There are other problems with the Fallopian tubes that can impair their function. These are discussed below:
- Previous pelvic surgeries can result in scar tissue that limits the movement of the Fallopian tubes
- Ectopic pregnancy resulting in removal of the tube (salpingectomy)
- Tubal ligation
- Congenital malformations of the tubes
Any alteration in the Fallopian tubes that cuases their blockage and impedes their freedom of movement is a cause of tubal factor infertility.
Diagnosis of tubal factor
In most cases, problems in the Fallopian tubes do not cause perceivable symptoms. Therefore, a tubal factor is usually diagnosed only after the couple has not been sucessful in conceiving after a period of trying, and proceed to fertility testing.
Fallopian tube patency can be assessed by the following diagnostic tests:
- Ultrasound
- is performed routinely in the gynecology clinic, but this test is only capable of detecting large hydrosalpinx.
- Hysterosalpingography (HSG)
- is the most important test to check the patency of the tubes. It consists of injecting a contrast dye through the cervix to observe its trajectory towards the tubes as x-ray pictures are taken. If there is any obstruction, the contrast dye will become trapped and cause distention of the tube.
- Hysterosalpingosonography (HSSG)
- is an improved version of the previous HSG. Here, a saline solution or foaming gel is injected through the cervix instead of the contrast dye. In addition, the use of x-rays is replaced by routine transvaginal ultrasound.
- Laparoscopy
- is a surgical intervention in which two small incisions are made under the navel and a camera is introduced that allows observation of the tubes and their relationship with the rest of the structures of the reproductive system, from the abdominal cavity.

However, laparoscopy is usually only performed in cases of suspected endometriosis, adhesions or other abnormalities that can be surgically corrected at the same time.
Treatment of tubal factor
Treatment of fallopian tube conditions depends on the specific cause.
Bacterial infections such as chlamydia should be treated with antibiotics. However, if the fallopian tubes are already damaged, drugs will not be able to solve this alteration.
Furthermore, it is also important to consider whether the tubal involvement is unilateral or bilateral.
Unilateral tubal factor
As previously mentioned, in the case of unilateral tubal factor, natural pregnancy will be possible. However, the couple may resort to assisted reproductive techniques if they have difficulties in achieving gestation.
Since only one tube is damaged in these cases, artificial insemination (AI) or IVF may be recommended. The choice of one assisted reproductive technique over another will depend on the particular situation of each woman or couple.
Bilateral tubal factor
If both fallopian tubes are affected, surgery to repair and reopen the tubes may be possible, depending on the cause of the blockage and its severity.
However, it may be difficult for a woman to regain fertility after tubal surgery because of its complexity. For this reason, many women with bilateral tubal factors resort to assisted reproduction to become mothers.
The specific treatment that does not require any tubal functionality to achieve pregnancy is IVF.

In spite of this, when hydrosalpinx is present, surgery to remove the damaged fallopian tube (called salpingectomy) is recommended prior to the IVF cycle. This intervention increases the chances of getting pregnant, as it prevents the flow of the otherwise accumulated fluid into the uterus.
To find out more details of IVF treatment, access the following article: What is in vitro fertilization (IVF)? - Process, cost and success rates.
Video on female tubal factor infertility
In the following video, Dr. Antonio Forgiarini, gynaecologist at Next Fertility Valencia, talks about female infertility due to tubal factor, its causes and treatment.
FAQs from users
After Chlamydia trachomatis infection, will tubal infertility develop?
Tubal factor is responsible for 12% to 33% of female infertility. Chlamydia infection is a fairly common STD, which can affect both men and women. It can progress to PID (pelvic inflammatory disease) and cause significant and permanent damage to a woman's reproductive system, especially the fallopian tubes, and cause fertility problems.
Read more
What is the best solution for getting pregnant with blocked Fallopian tubes?
When both fallopian tubes are blocked, depending on the cause of the blockage, it may be possible to perform surgery to try to restore tubal patency and function. However, this is a complex surgery that is not always successful in enabling the woman to subsequently conceive naturally.
For this reason, in vitro fertilization (IVF) is often used directly. This is an assisted reproduction technique that does not require tubal function to be successful.
Can pregnancy be achieved with a single fallopian tube?
The answer is yes. The fallopian tube is a mobile organ responsible for collecting the oocyte once it has ovulated. It is also the site where fertilization takes place (sperm and egg usually meet in the ampullary portion), the duct that connects this site with the uterus and, therefore, with the outside of the woman. The fallopian tubes also have the important function of serving as an incubator for the development of the already fertilized embryos, moving them carefully by means of their cilia to the uterus, in a journey that will last approximately 5 days.
All these functions are performed independently by the two fallopian tubes. Thus, when one of them is missing, this cadence does not affect the other one, which could even pick up oocytes from the contralateral ovary. Therefore, even when one tube is missing, the patient can become pregnant.
What are the causes of a tubal factor?
Antonio Forgiarini, gynaecologist at Next Fertility Valencia, tells us about the possible causes of female infertility due to tubal factor:
We can have a lot of causes. I think the most frequent are adhesions from infections, from pelvic infections or from endometriosis for example. So, these are pathologies that causes inflammation in the pelvis, some scars, some adhesions that can block the tubes and can close them. We have a lot of other causes that are very rare like agenesia, some women can be birth without the Fallopian tubes for example or they cannot function properly, but I think the two most important causes are endometriosis and infections.
What symptoms can a fallopian tube blockage cause?
A fallopian tube obstruction doesn't actually cause symptoms on its own. However, the underlying cause that led to that tubal blockage can also produce other symptoms. That's the case with infections, which can cause abnormal vaginal discharge, or, for example, endometriosis, which is characterized by causing very painful periods.
Read more
Recommended readings
Hysterosalpingography is the most important diagnostic test for tubal permeability. If you're interested in reading more about this topic, have a look at this post: How Is a Hysterosalpingography (HSG) Performed?.
If you're looking to have another baby, but have had a tubal ligation, you may be interested in the following article: What Are Your Chances of Pregnancy After Tubal Ligation?.
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Camus E, Poncelet C, Goffinet F, et al. Pregnancy rates after in-vitro fertilization in cases of tubal infertility with and without hydrosalpinx: a meta-analysis of published comparative studies. Hum Reprod 1999;14:1243–9 (View)
Chua SJ, Akande VA, Mol BW. Surgery for tubal infertility. Cochrane Database Syst Rev. 2017 Jan 23;1(1):CD006415 (View)
Dun EC, Nezhat CH. Tubal factor infertility: diagnosis and management in the era of assisted reproductive technology. Obstet Gynecol Clin North Am. 2012 Dec;39(4):551-66 (View)
Heikkinen H, Tekay A, Volpi E, Martikainen H, Jouppila P. Transvaginal salpingosonography for the assessment of tubal patency in infertile women: methodological and clinical experiences. Fertil Steril 1995;64: 293–8 (View)
Mardh PA. Tubal factor infertility, with special regard to chlamydial salpingitis. Current Opinion in Infectious Diseases 2004;17:49–52 (View)
Ng KYB, Cheong Y. Hydrosalpinx - Salpingostomy, salpingectomy or tubal occlusion. Best Pract Res Clin Obstet Gynaecol. 2019 Aug;59:41-47 (View)
Papaioannou S, Afnan M, Jafettas J. Tubal assessment tests: still have not found what we are looking for. Reprod Biomed Online 2007;15:376–82 (View)
Siassakos D, Syed A, Wardle P. Tubal disease and assisted reproduction. The Obstetrician & Gynaecologist 2008;10:00–00 (View)
Suresh YN, Narvekar NN. The role of tubal patency tests and tubal surgery in the era of assisted reproductive techniques. The Obstetrician & Gynaecologist 2014;16:37–45 (View)
Thurston L, Abbara A, Dhillo WS. Investigation and management of subfertility. J Clin Pathol. 2019 Sep;72(9):579-587 (View)
Tsevat DG, Wiesenfeld HC, Parks C, Peipert JF. Sexually transmitted diseases and infertility. Am J Obstet Gynecol. 2017 Jan;216(1):1-9 (View)
FAQs from users: 'After Chlamydia trachomatis infection, will tubal infertility develop?', 'What is the best solution for getting pregnant with blocked Fallopian tubes?', 'Can pregnancy be achieved with a single fallopian tube?', 'What does female infertility due to tubal factor refer to?', 'Why are fallopian tubes important?', 'What are the causes of a tubal factor?', 'How is a tubal obstruction diagnosed?', 'Is there a cure for tubal obstruction?', 'What symptoms can a fallopian tube blockage cause?', 'Why does female infertility due to tubal factor occur?', 'How is female infertility due to tubal factor diagnosed?' and 'What is the treatment for female infertility due to tubal factor?'.
Authors and contributors





More information about Cristina Algarra Goosman

More information about Michelle Lorraine Embleton

Hi, I have a tubal ligation and I think I am pregnant, is it possible?
Hi Diana,
The effectiveness rate of a tubal ligation or bilateral tubal occlusion is 99%, that is, one in 100 women can become pregnant after this procedure.
I recommend that you go to your doctor so that he/she can check if the operation has been performed correctly.
I hope I have helped you.
Best regards.
Hi, I have been told that before trying to get pregnant I have to have a fallopian tube fixed, they say I have like fluid inside and that it will be somewhat problematic to get pregnant. Is this true? I don’t want to have surgery
Hello Nora,
The accumulation of fluid in the fallopian tubes is due to a previous infection, this case is known as hydrosalpinx, facing pregnancy is advisable to perform a surgical intervention to drain the fluid from the tube and make it permeable and functional. In this way, you will have the option of having a pregnancy in a natural way.
I hope I have helped you.
Best regards.