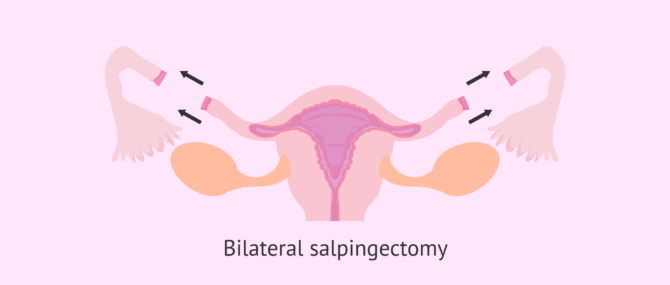
Salpingectomy is a surgical procedure that consists of the removal of a woman's fallopian tubes, thus causing sterility.
This surgery can be unilateral, if only one tube is removed, or bilateral, if both tubes are removed. Although natural pregnancy is not possible without fallopian tubes, these women can fulfill their desire to become mothers through assisted reproductive techniques.
The indications for needing a salpingectomy are diverse, as are the techniques used in surgery.
Provided below is an index with the 10 points we are going to expand on in this article.
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 6.1.
- 6.2.
- 6.3.
- 6.4.
- 6.5.
- 7.
- 8.
- 9.
- 10.
What is a salpingectomy?
Salpingectomy is the removal of one or both of a woman's fallopian tubes due to pathologies or alterations that may affect her reproductive system.
Some specialists use the term salpingectomy to refer to tubal ligation surgery, but this is incorrect.
Tubal ligation is a definitive method of sterilization in which only the tubes are cut or blocked to prevent pregnancy, not completely removed.
The consequence of removing the fallopian tubes is that once ovulation takes place, the egg is lost and cannot meet the sperm for fertilization. Therefore, natural pregnancy with a bilateral salpingectomy is impossible.
In the case of a unilateral salpingectomy, the woman would still be fertile and could achieve a natural pregnancy thanks to the other tube she keeps. However, it should be taken into account whether ovulation occurs on the right side or the left side of each particular month.
How is it carried out?
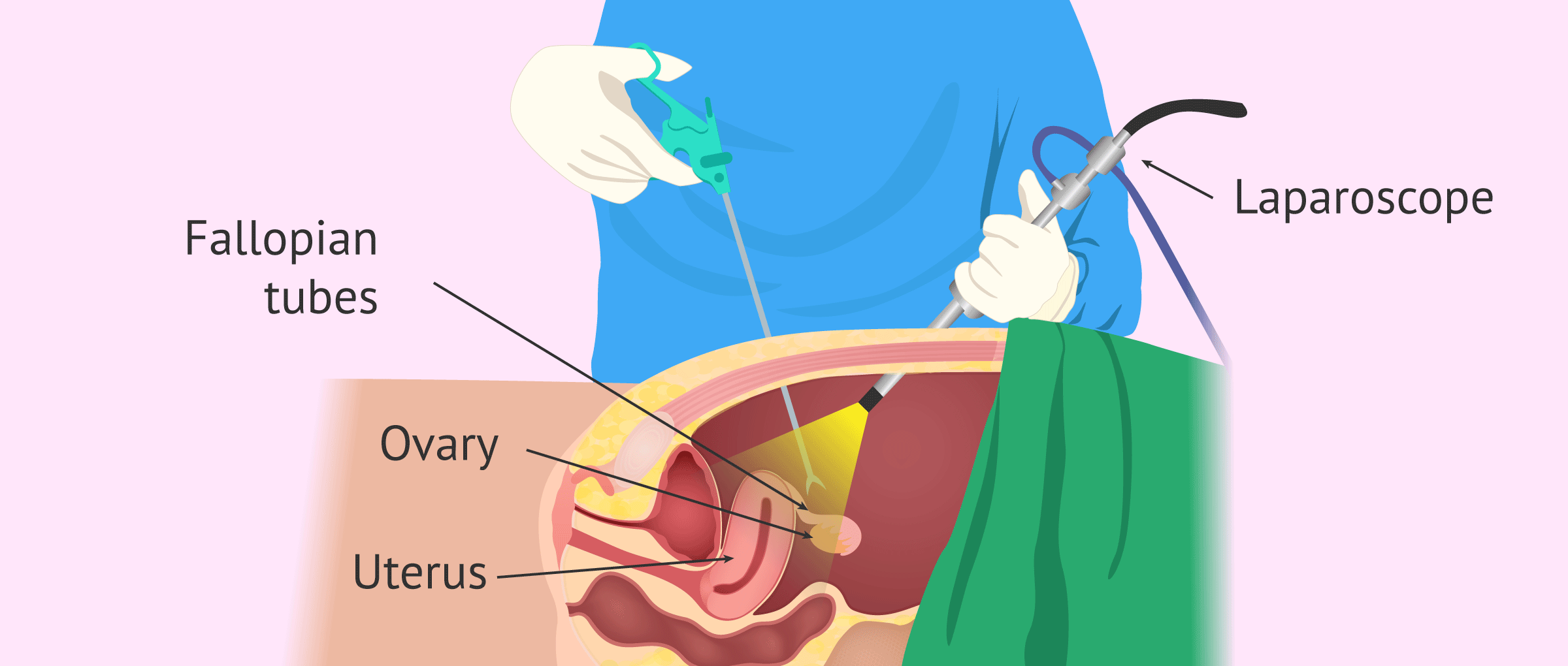
Salpingectomy can be done using two surgical techniques:
- Laparoscopy
- is a non-invasive surgery that consists of introducing an optical system through a small incision in the abdomen to observe the cavity. Another small incision is made just above the pubic hair, and the tubes are removed with a tube. It is the most widely used technique today, as women can lead normal lives after 48 hours.
- Laparotomy
- is more invasive than the previous one because it requires a 5 to 10 cm incision in the lower abdomen. Currently, there is a variant known as a mini-laparotomy, in which a smaller incision of about 5 cm is made, sufficient to allow access to and removal of the tubes.
The choice of one of these methods depends on several factors: age, weight, previous surgeries on the abdomen, diseases, etc.
When is salpingectomy indicated?
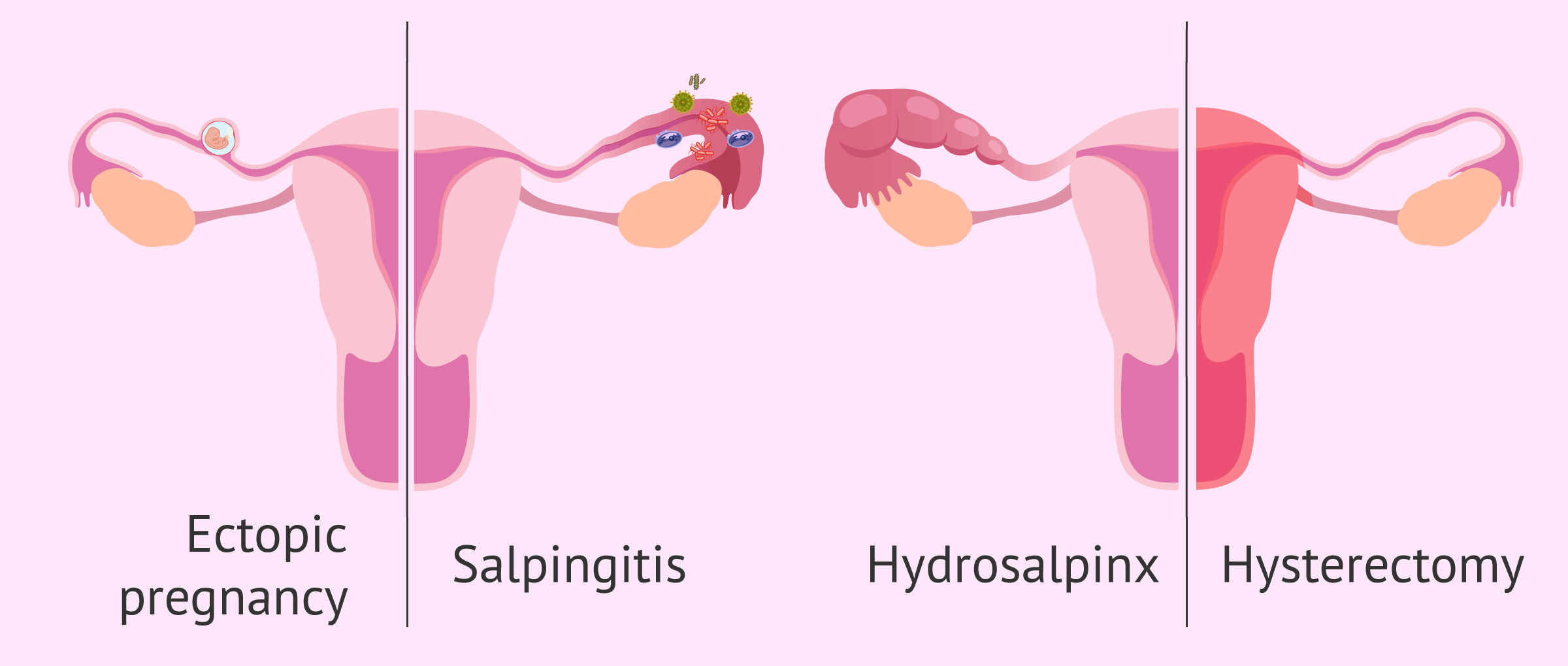
The possible pathologies and alterations that require the removal of the fallopian tubes are the following:
- Ectopic pregnancy
- implantation of the embryo in the tube instead of the uterus. The growth of the embryo in the tube can cause it to rupture and therefore it has to be removed. In this case, the salpingectomy is unilateral.
- Endometriosis
- growth of endometrial tissue outside the uterus. If the lesions caused in the tubes are very severe, it will be necessary to perform a salpingectomy, which is usually bilateral.
- Salpingitis
- inflammation of the fallopian tubes caused by an infection. In case of severe chronic infection, where antibiotics do not affect, salpingectomy will be necessary.
- Hydrosalpinx
- blocking and accumulating of fluid in the tube that causes it to dilate. In the most serious cases, when the hydrosalpinx is larger than 3 cm, one or both tubes are removed.
- Hysterectomy
- when it is necessary to remove the uterus, a salpingectomy is usually performed together, as preserving the tubes could bring complications and they do not bring any benefit. The ovaries, on the other hand, are preserved so as not to cause early menopause.
- Prevention of ovarian cancer
- some studies claim that removing the tubes may reduce the risk of ovarian cancer in women with a genetic predisposition.
Side effects of fallopian tube removal
Salpingectomy is a very safe technique that usually does not cause any short or long term complications. In any case, the possible side effects will depend on the surgical technique used.
On the one hand, laparoscopy involves a very small incision and therefore recovery time is short. However, it is possible that in the days following the surgery, the patient may experience abdominal discomfort and swelling due to the gas being injected to expand the abdomen.
On the other hand, the surgical wound from the laparotomy is larger, which implies more pain in this area and special aftercare to treat the scar. There is also an increased risk of bleeding and infection, although this is not common.
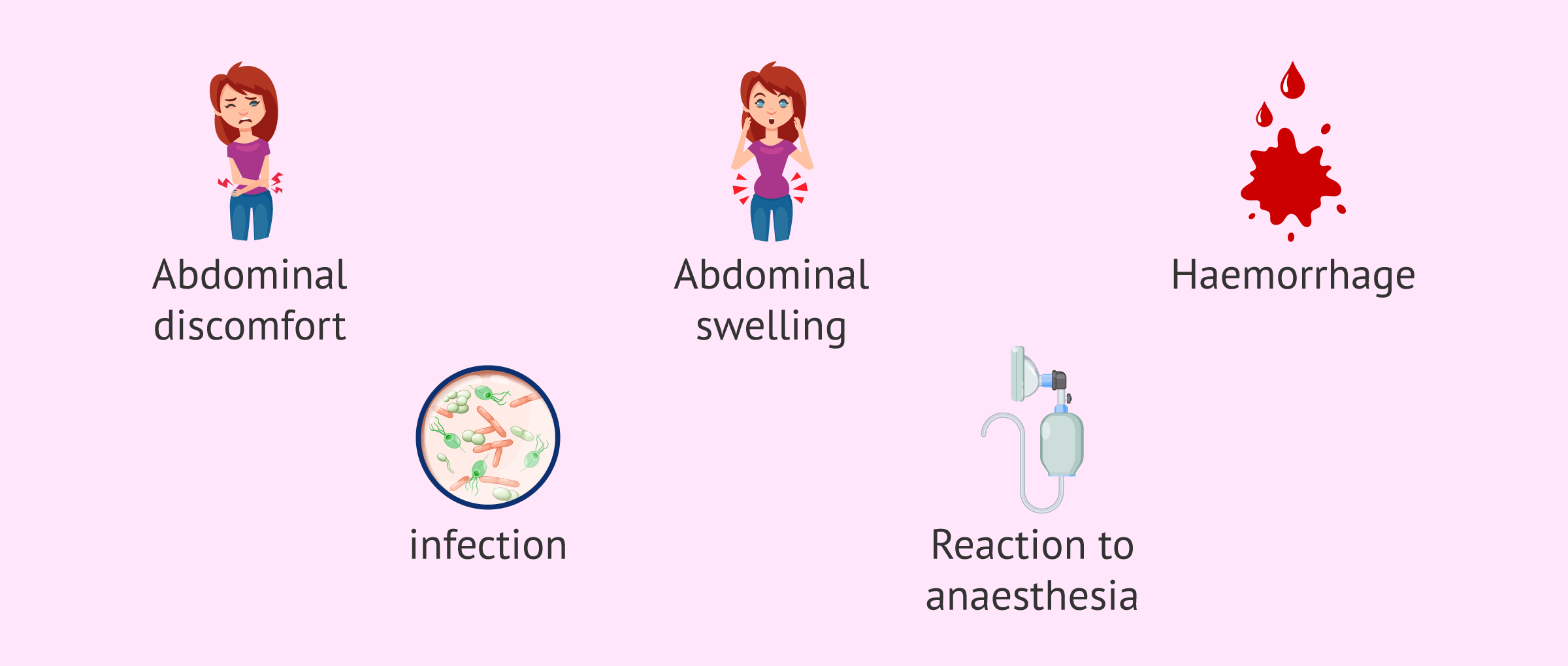
Finally, it should be noted that the risk of reaction to anesthesia is the same for both techniques and that serious injury to internal organs rarely occurs.
Pregnancy after salpingectomy
Natural pregnancy is not possible if there is no integrity in at least one of the fallopian tubes, as discussed above.
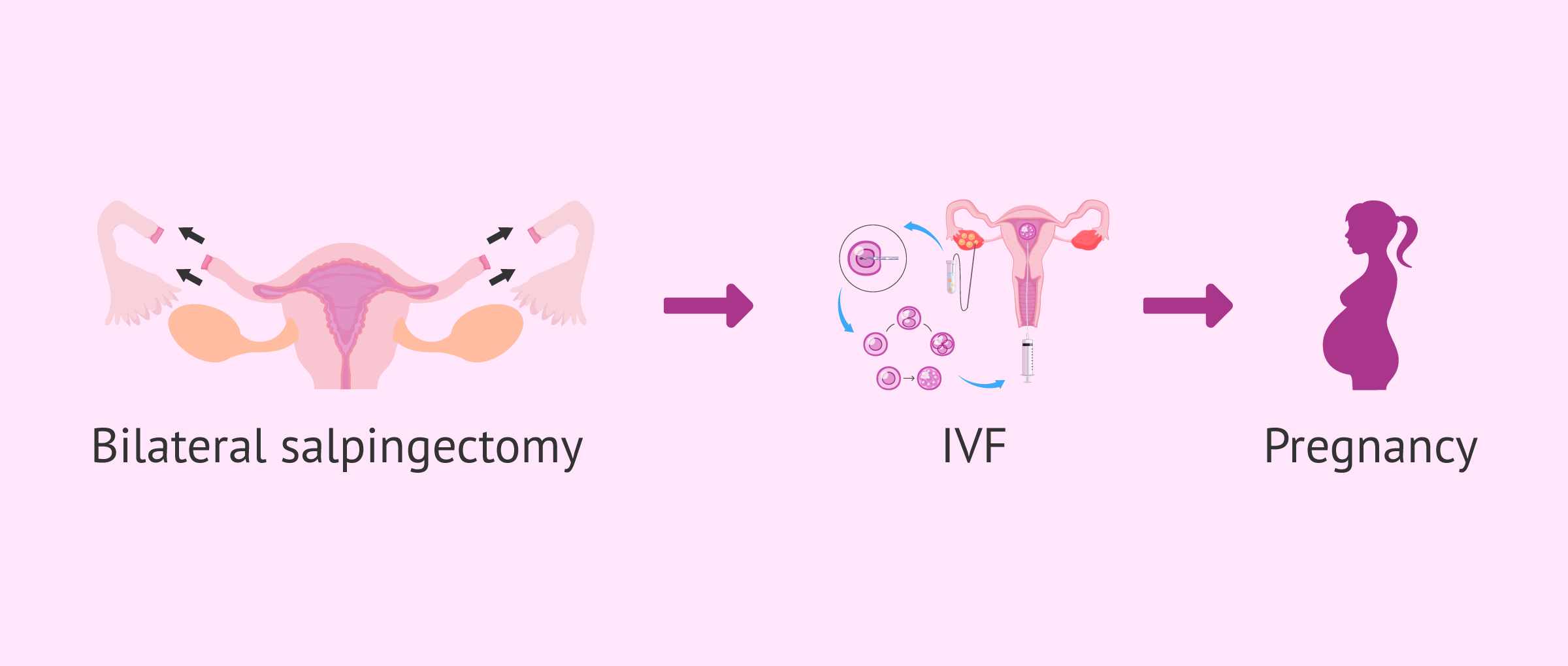
Despite this, even in the most severe cases of bilateral salpingectomy, the patient can still become pregnant thanks to assisted reproduction techniques such as in vitro fertilization (IVF).
If you need to undergo IVF to become a mother, we recommend that you generate your Fertility Report now. In 3 simple steps, it will show you a list of clinics that fit your preferences and meet our strict quality criteria. Moreover, you will receive a report via email with useful tips to visit a fertility clinic for the first time.
In IVF, the eggs are obtained directly from the woman's ovaries and therefore no tubal functionality is required. The embryos are fertilized in the laboratory with the sperm of the male partner or an anonymous donor, and then transferred directly to the mother's uterus.
The uterus, however, is strictly necessary for conception. In cases when it is even necessary to remove the uterus along with the tubes, attempts are always made to leave the ovaries so that the woman retains the production of sex hormones and to allow the possibility of having a biological child should she consider surrogacy in the future.

If you are interested in knowing what surrogacy treatment consists of in a more detailed way, we invite you to visit the following post: What is surrogacy?
FAQs from users
How can pregnancy be achieved with bilateral salpingectomy?
Bilateral salpinguectomy is an operation in which both tubes are removed. The Fallopian tube is a tubular structure that comes out of the uterus and is responsible for collecting the egg that leaves the ovary at ovulation. Inside the tube
the union between egg and sperm takes place. If neither of the two tubes are present, gestation is not possible in a natural way. Therefore, in women who do not have tubes, the only technique that can be performed is IVF.
In it we perform the first phase of ovarian stimulation to have the maximum possible number of oocytes and fertilization of the eggs is performed in the laboratory, a step that is normally done in the tubes in a natural gestation. Once the embryos are obtained, the best one or ones are transferred to the uterus. Having a bilateral salpinguectomy does not decrease the probability of pregnancy with in vitro fertilization.
Is a natural pregnancy possible with a bilateral salpingectomy?
In case of a bilateral salpingectomy, that is, in the absence of both Fallopian tubes, pregnancy cannot occur naturally. In these cases we must resort to In Vitro Fertilization (IVF) to achieve pregnancy.
In IVF, as its name indicates, the fertilization of the egg is performed in the laboratory (in vitro), so that we do not need the fallopian tube to perform its function.
We extract the eggs directly from the woman's ovaries through a procedure called follicular puncture. We take these eggs to the laboratory, where we perform the fertilization of the egg with the sperm of the couple or a donor. In this way we obtain embryos. The embryos are then transferred into the woman's uterus to achieve pregnancy.
In fact, the pathology of the fallopian tubes (tubal pathology), either by absence (post-salpingectomy) or by alteration of its function (obstruction, dilatation, etc.), was what led to the research and development of the first IVFs in history.
In what situations is it strictly necessary to perform a salpingectomy?
Salpingectomy is the surgical removal of one or both fallopian tubes.
In medicine, there is not always data to support diagnostic or therapeutic behavior. This is not the case when, in the context of the study of reproductive dysfunction, a hydrosalpinx appears.
A hydrosalpinx is the dilation of the fallopian tube due to the presence of fluid inside it. When diagnosed, salpingectomy before in vitro fertilization treatment improves the chances of achieving a pregnancy. This is according to the review carried out by the Cochrane Library, probably the most rigorous and reliable organization of researchers when making recommendations in health sciences.
Therefore this would be a case where salpingectomy would be highly advisable. This is what science says but the Law makes clear the right to patient autonomy. The law says: "Any action in the field of health of a patient needs the free and voluntary consent of the affected person, once, received the information provided in Article 4, has assessed the options specific to the case". Because of this bioethical principle of autonomy, the patient can decide, even though she knows that the prognosis of the in vitro fertilization treatment worsens, not to undergo a salpingectomy. The concept of "strictly necessary" is therefore relegated to what the patient, properly informed, decides.
Is it possible to achieve natural pregnancy with unilateral salpingectomy?
Yes, but it is more difficult because ovulation must occur through the ovary with the intact tube for there to be a chance of fertilization and pregnancy.
In the event of not achieving a natural pregnancy, it is possible to control ovulation with hormonal medication and to schedule sexual intercourse on the fertile days. It is also possible to try artificial insemination to increase the possibility of pregnancy.
What is partial salpingectomy?
As the name implies, partial salpingectomy is the cutting and removal of a segment of the fallopian tube. This method is the most commonly used to perform a tubal ligation and is known as Pomeroy.
Recommended reading
The extirpation of the fallopian tube is necessary in severe cases of a tubal factor in women. If you are interested in this topic, you can continue reading in thefollowing post: Female infertility due to tubal factor: causes and treatments
We have talked about in vitro fertilization as a fertility treatment for getting pregnant. To find out what this treatment consists of, we recommend that you read on at the following link: What is IVF?
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Ahmed Aboelfadle Mohamed, Ali Haroun Yosef, Cathryn James, Tarek Khalaf Al-Hussaini, Mohamed Ali Bedaiwy, Saad Ali K S Amer. Ovarian reserve after salpingectomy: a systematic review and meta-analysis. Acta Obstet Gynecol Scand. 2017 Jul;96(7):795-803. doi: 10.1111/aogs.13133 (View)
Diccionario de términos médicos. Real Academia Nacional de Medicina de España. 2012.
Joanne Kotsopoulos, Steven A Narod. Prophylactic salpingectomy for the prevention of ovarian cancer: Who should we target? Int J Cancer. 2020 Sep 1;147(5):1245-1251. doi: 10.1002/ijc.32916. Epub 2020 Feb 29 (View)
Johnson NP, Mak W, Sowter MC. Tratamiento quirúrgico para la enfermedad tubaria en mujeres que se someterán a una fecundación in vitro (Revisión Cochrane traducida). En: La Biblioteca Cochrane Plus, 2008 Número 4 (View)
Ley 41/2002 de 14 de noviembre, básica reguladora de la autonomía del paciente y derechos y obligaciones en materia de información y documentación clínica (View)
Marco Noventa, Salvatore Gizzo, Carlo Saccardi, Shara Borgato, Amerigo Vitagliano, Michela Quaranta, Pietro Litta, Michele Gangemi, Guido Ambrosini, Donato D'Antona, Stefano Palomba. Salpingectomy before assisted reproductive technologies: a systematic literature review. J Ovarian Res. 2016 Nov 3;9(1):74. doi: 10.1186/s13048-016-0284-1 (View)
Mary B Daly, Charles W Dresher, Melinda S Yates, Joanne M Jeter, Beth Y Karlan, David S Alberts, Karen H Lu. Salpingectomy as a means to reduce ovarian cancer risk. Cancer Prev Res (Phila). 2015 May;8(5):342-8. doi: 10.1158/1940-6207.CAPR-14-0293 (View)
Sang-Hee Yoon, Ji Young Lee, Soo-Nyung Kim, Hye Won Chung, So Yun Park, Chulmin Lee. Does salpingectomy have a deleterious impact on ovarian response in in vitro fertilization cycles? Fertil Steril. 2016 Oct;106(5):1083-1092.e5. doi: 10.1016/j.fertnstert.2016.05.030 (View)
FAQs from users: 'How can pregnancy be achieved with bilateral salpingectomy?', 'Is a natural pregnancy possible with a bilateral salpingectomy?', 'In what situations is it strictly necessary to perform a salpingectomy?', 'Is it possible to achieve natural pregnancy with unilateral salpingectomy?' and 'What is partial salpingectomy?'.
Authors and contributors






More information about Michelle Lorraine Embleton

Hi, I´m going to get my tubes tied next week. Is this the same thing?
Hi HarrieTT
A tubal ligation, commonly known as getting your tubes tied, is not the same as a salpingectomy. In a salpingectomy the Fallopian tube is removed completely, due to disease or abnormality.
In a tubal ligation procedure the Fallopian tube is closed off with tubes or rings, and the section between them is cut or burned, making the tube impassible for the egg. It is a form of permanat female contraception. You can read more about the procedure in this article: Tubal Ligation Procedure – Should You Get Your Tubes Tied?
I hope this information has helped.
Best wishes