Problems with a woman's fertility can have different origins depending on the point at which the alteration occurs. Thus, we can find problems due to ovarian endocrine factor (hormonal), tubal factor (in the Fallopian tubes), uterine factor and cervical factor (in the uterine cervix).
However, nowadays, one of the most common reasons for female infertility is advanced maternal age. The pace of life in today's society means many women are delaying having chidren.This leads to a deterioration in female fertility due to a decrease in the number and quality of oocytes as ages increases.
Despite this, the different assisted reproduction techniques can help, in many cases of female infertility, to achieve the desired pregnancy.
Provided below is an index with the 8 points we are going to expand on in this article.
- 1.
- 2.
- 2.1.
- 2.2.
- 2.3.
- 3.
- 4.
- 4.1.
- 4.2.
- 4.3.
- 4.4.
- 4.5.
- 4.6.
- 5.
- 6.
- 7.
- 8.
Indications for infertility treatment
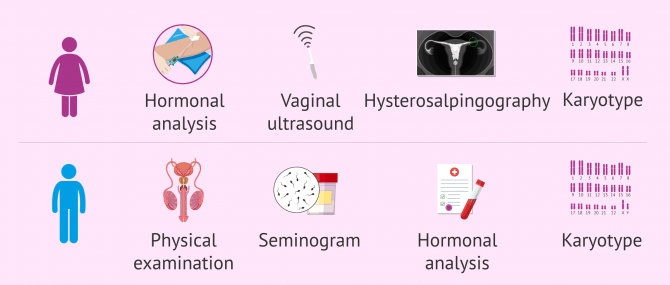
In order to choose the most appropriate female infertility treatment for each situation, the necessary fertility tests must be performed. This fertility study should be carried out on both the woman and the man, as there are times when the problem is not only with the woman or the with the man, but with both.
There are also situations in which the fertility tests in both partners are correct and, nevertheless, pregnancy is not achieved. These are cases of infertility of unknown origin or unexplained fertility.
Depending on the problem that causes female infertility and the woman's age, different assisted reproduction treatments may be recommended. These can be more or less complex, but they all have the same goal: to make it possible to get pregnant and have a healthy baby at home.
Assisted procreation, as any other medical treatment, requires that you rely on the professionalism of the doctors and staff of the clinic you choose. Obviously, each clinic is different. Get now your Fertility Report, which will select several clinics for you out of the pool of clinics that meet our strict quality criteria. Moreover, it will offer you a comparison between the fees and conditions each clinic offers in order for you to make a well informed choice.
Assisted reproduction and female infertility
When the fertility problem is caused by a female factor, there are several reproductive options that can be carried out. Here are the main assisted reproductive techniques that are performed for the treatment of infertility.
Artificial insemination (AI)
Also known as intrauterine insemination, IUI, this assisted reproduction technique consists of introducing a seminal sample, previously processed in the laboratory, directly into the woman's uterus through the cervix. It should be noted that this technique is performed during the woman's ovulatory period, in order to increase the chances of gestation.
To use this assisted reproduction treatment, the degree of infertility of the patient must be mild. In addition, the woman should be no older than 35-37 years of age to ensure success.

Additionally, it is an absolute requirement for the Fallopian tubes to be functional in order to perform an IUI, since the Fallopian tubes are where the egg waits for the sperm. If the tubes are blocked, the union of egg and sperm cannot take place.
AI is used as a treatment in cases of female infertility in which the woman presents:
- Mild endometriosis.
- Ovulatory dysfunctions such as, for example, those caused by Polycystic Ovary Syndrome (PCOS).
- Changes in the cervix (cervical factor).
- Unexplained infertility. In the cases where the reason for the couple's infertility is not known, the specialist may choose to begin performing IUI.

AI is also used for women without a partner or for same sex female couples who wish to become pregnant and, in principle, do not have any infertility problems. In this case, AI would be performed with sperm from a donor.
The price of IUI in the USA is $600-$3000, with an average of approximately $1500. It is important to note that the price of additional medication is usually excluded from the estimate.
If you would like to read more about intrauterine insemination, then please click the following link: What Is Artificial Insemination (AI)? - Process, Cost & Types.
In vitro fertilization (IVF)
As the name suggests, the union between the egg and sperm in IVF takes place in the laboratory, in vitro, the latin for "in glass". For this, the patient needs to undergo ovarian stimulation and the specialist obtains the eggs by follicular puncture, or ovum pickup. Subsequently, these eggs are placed in contact with a previously obtained and prepared semen sample, so that fertilization can take place.
The embryos generated after fertilization remain in culture for a few days, after which they are transfered to the woman's uterus in order to produce pregnancy. Generally, it is decided to transfer a single embryo in each embryo transfer, and if there are "leftover" embryos of good quality, they can be vitrified for future transfers.
IVF is used to treat female infertility when there is/are:
- Problems in the Fallopian tubes (tubal factor).
- Low ovarian reserve.
- Advanced maternal age.
- Endometriosis

IVF would also be recommended when there are previous failures of artificial insemination (AI) or unexplained fertility.
The cost of IVF using your own eggs can range from $8,500 to $12,000 for a single cycle. However, it may vary depending on the tests needed and the fertility clinic. Again, the cost of additional medication is usually excluded from the estimate.
ICSI
There is a variation of conventional IVF. This is the ICSI technique or intracytoplasmic sperm injection, which involves greater intervention by the embryologist. The whole process is identical in both cases, except that in ICSI the union between egg and sperm is performed by microinjecting the sperm directly into the oocyte.
This advanced in vitro fertilization process is especially indicated for severe male fertility problems. However, ICSI is generally displacing the use of conventional IVF. Furthermore, ICSI is the technique of choice after previous failures of conventional IVF or when a preimplantation genetic test (PGT) is to be performed.

If you are interested in more information about IVF and ICSI, you can click here: In vitro fertilization (IVF): What Is In Vitro Fertilization (IVF)? - Process, Cost & Success Rates.
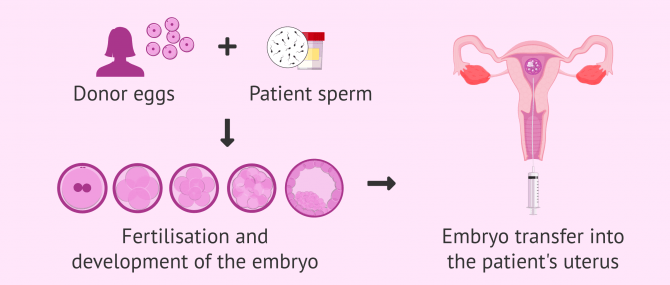
Ovodonation
This assisted reproduction technique consists of using the oocytes, egg cells, of an anonymous donor instead of the patient's own oocytes. Using egg donation means the patient must renounce that the embryos and, therefore, their possible future children, carry her genetic load.
There are occasions in which the specific cause of female infertility prevents the use of the patient's own egg cells (for example, in a woman who lacks ovaries) or in which assisted reproduction techniques have a very low success rate with the patient's own oocytes (for example, if the maternal age is advanced).
Ovodonation is one of the most expensive assisted reproduction treatments. The price in the USA can range between $14,000 and $20,000 depending on the fertility clinic and the type of egg donation.
If you would like to read more in depth about ovodonation, you can find lots more information in this article: What is IVF with egg donation and how much does treatment cost?.
Video on ART for female infertility
In the following video, Michelle Emblenton, a biochemist at inviTRA, explains the different assisted reproduction techniques (ART) to combat infertility in women:
Female infertility can be caused by a variety of factors. So, in order to find the best treatment, we need to start with fertility studies. Fertility studies have to be carried out in both the man and the woman, because sometimes the fertility issues with the woman, sometimes with the man and, in a proportion of cases, with both.
FAQs from users
What are the results like for female infertility treatments?
The results for a particular patient depend mainly on four factors: age, ovarian reserve, the laboratory and the gynecologist.
The age of the patient is undoubtedly the most important factor in predicting the results of the assisted reproduction technique. The older the patient, the worse the results. The ovarian reserve is not such a conclusive predictor of the rate of results of assisted reproductive techniques. A good ovarian reserve allows a higher cumulative pregnancy rate (after having transferred all the embryos resulting from an ovarian puncture). As more eggs have been obtained, there are more embryos, therefore more transfers and more attempts.
In relation to the laboratory, it is important to transfer embryos at day +5 and to have done preimplantational genetic diagnosis (PGD). This implies that the live birth rate is more solid.

Last but not least, there is the gynecologist dependent factor. Scientific studies show differences in gestation rates of more than 15% in gynecologists working in the same center. Therefore, stimulation and transfer are key to the success of fertility treatments.
The fact that a gynecologist knows the patient and takes her from the beginning to the end, that will strengthen the trust and the doctor-patient relationship, making everything more favorable to achieve pregnancy. Continuous changes of medical personnel do not favor the whole process Z well controlled.
What are the possible treatment options for female infertility?
After a study of the couple as a whole, female infertility may be detected. Some of the most common causes of female fertility problems are PCOS, endometriosis, tubal obstruction, low ovarian reserve and advanced maternal age.
Depending on the reason for female infertility, there are several treatment options. For example, clomiphene could be used to induce ovulation in women with PCOS, assisted reproductive techniques such as AI or IVF could be used, donor eggs could be used, and so on.
Read more
What are the main female infertility tests?
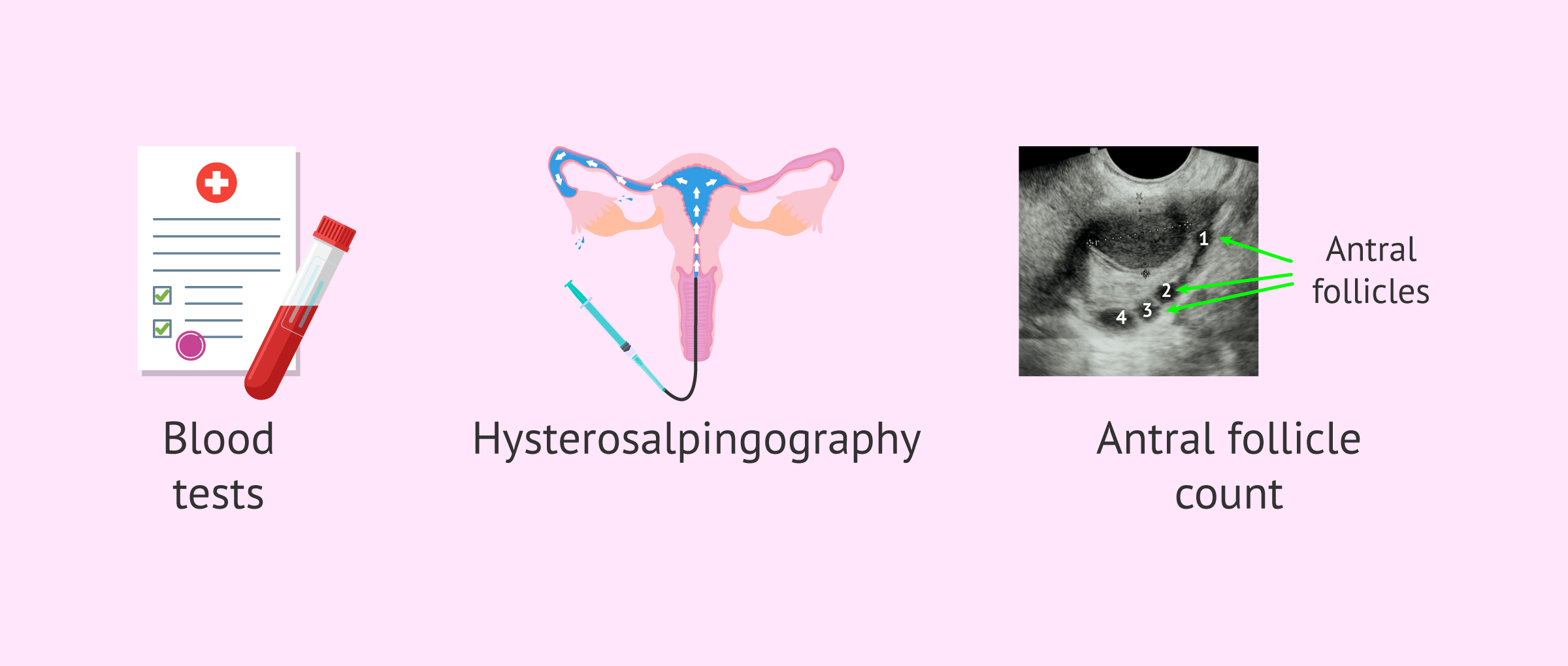
The main tests for studying female fertility are as follows:
- Blood tests where different hormones are analyzed, such as FSH, LH, estradiol, Anti-Müllerian Hormone (AMH), TSH, prolactin, and progesterone.
- Test to evaluate tubal patency known as hysterosalpingography.
- Ultrasound with antral follicle count (AFC).
Although these are the basic tests in the study of female fertility, it is also possible to request complementary tests such as karyotype analysis, a hysteroscopy, or an endometrial biopsy if the specialist considers it appropriate.
Is it possible to have assisted reproductive treatment for female infertility in a hospital?
Yes, currently in Spain a woman (or a couple) can access assisted reproduction treatments through Social Security.
However, there are a series of requirements that must be met in order to be able to access these treatments through Social Security. These requirements may vary slightly between the different autonomous communities and generally have to do with age and the number of previous children.
Are there any surgical treatments for female infertility?
Yes, on some occasions surgery may be necessary to increase a woman's chances of becoming pregnant, or prior to assisted reproduction treatment.
In certain cases of endometriosis, fibroids, adhesions, etc., the specialist may consider surgery to be appropriate.
Tubal surgery is rarely performed, as it is more common to resort directly to in vitro fertilisation (IVF). However, in the case of hydrosalpinx, it seems that its removal by salpingectomy (surgery to eliminate the fallopian tube) prior to IVF improves the possibility of pregnancy.
Are there any natural treatments for female infertility?
Michelle Emblenton, a biochemist at inviTRA, answers this question in the video:
There are always natural ways and remedies to increase your fertility as a woman. Leading a healthy lifestyle, avoiding an excess of alcohol, not smoking, not taking street drugs, keeping your weight at the desirable level and moderate exercise. All of these things really help to increase the woman's fertility. However, some cases of infertility in women won't respond well to natural remedies and will need some kind of intervention in order for the woman to become pregnant.
Recommended reading
If you want to learn more about the female fertility study, you can visit the following link: Female Fertility Tests - How Do You Know if You Can't Get Pregnant?
Alternatively, if you are interested in the treatment of male infertility, we recommend you read the following article: Treatments for Male Infertility.
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Babayev SN, Park CW, Bukulmez O. Intracytoplasmic sperm injection indications: how rigorous? Semin Reprod Med. 2014 Jul;32(4):283-90 (View)
Bosch E, Espinós JJ, Fabregues F, Fontes J, García-Velasco J, Llácer J, Requena A, Checa MA, Bellver J; Spanish Infertility SWOT Group (SISG). ALWAYS ICSI? A SWOT analysis. J Assist Reprod Genet. 2020 Sep;37(9):2081-2092 (View)
Goverde AJ, McDonnell J, Vermeiden JP, Schats R, Rutten FF, Schoemaker J (2000). Intrauterine insemination or in-vitro fertilisation in idiopathic subfertility and male subfertility: a randomised trial and cost-effectiveness analysis. Lancet; 355: 13 –18 (View)
Haddad M, Stewart J, Xie P, Cheung S, Trout A, Keating D, Parrella A, Lawrence S, Rosenwaks Z, Palermo GD. Thoughts on the popularity of ICSI. J Assist Reprod Genet. 2021 Jan;38(1):101-123 (View)
Ibérico G, Vioque J, Ariza N, Lozano JM, Roca M, Llàcer J, Bernabeu R (2004). Analysis of factors influencing pregnancy rates in homologous intrauterine insemination. Fertil Steril;81:1308 – 1313 (View)
O'Neill CL, Chow S, Rosenwaks Z, Palermo GD. Development of ICSI. Reproduction. 2018 Jul;156(1):F51-F58 (View)
Practice Committees of the American Society for Reproductive Medicine and the Society for Assisted Reproductive Technology. Electronic address: asrm@asrm.org. Intracytoplasmic sperm injection (ICSI) for non-male factor indications: a committee opinion. Fertil Steril. 2020 Aug;114(2):239-245 (View)
Ragni G, Somigliana E, Vegetti W. (2004) Timing of intrauterine insemination: where are we? Fertil Steril;82:25 – 26 (View)
The ESHRE Capri Workshop Group (2009). Intrauterine insemination. Human Reproduction Update; 15 (3): 265–277.64 (View)
FAQs from users: 'How is intrauterine insemination (IUI) used to treat female infertility?', 'What are the results like for female infertility treatments?', 'What are the possible treatment options for female infertility?', 'What are the main female infertility tests?', 'What are the indications for female infertility treatments?', 'Is it possible to have assisted reproductive treatment for female infertility in a hospital?', 'What assisted reproduction techniques do we have to treat female infertility?', 'Are there any surgical treatments for female infertility?', 'Are there any natural treatments for female infertility?', 'How does in vitro fertilization (IVF) combat infertility?', 'How can we use donor eggs to treat female infertility?', 'What kind of results do we get from female infertility treatments?' and 'Are there any surgical treatments for female infertility?'.
Authors and contributors





More information about Michelle Lorraine Embleton

Hi there. I don’t know if you can help? I have a bilateral tube obstruction and my fertility doctor has advised me to go for IVF. But, I would much rather have IUI becuase it is so much simpler and cheaper. Is it possible for me? Thanks
Hi Nora_99days
To perform an intraunterine insemination (IUI) at least one of the Fallopian tubes must be patent and have function, meaning it is not obstructed and can allow passage of the egg and the sperm.
If both of the Fallopian tubes are blocked, as in your case, then the sperm and egg can not meet in the tubes and therefore and IUI will not have any chance of success.
For this reason, your doctor has recommended you go for IVF, as for IVF tubal patency is not needed. Fertilization, where the sperm meet the egg, takes place in the laboratoty, bypassing the need for the Fallopian tubes.
I hope this has helped!
All the best
Hi, just want to say that this is a very interesting article and I will be getting my girlfriend to read it. She has been told she has some fertility issues and is scared to go back for her appointment and face the problems.