What are the symptoms that indicate the onset of labor?
Approximately one month before the end of the gestational stage, the woman’s body begins to prepare for labor. Normally, labor occurs between the 38th and 40th weeks of gestation. However, sometimes labor occurs earlier, which is known as preterm labor.
It is not necessary for all pregnant women to experience every symptom of labor, but they will usually notice some of them. The final stage of pregnancy is often one of the most concerning periods for expectant mothers, but they should remain calm and relaxed.
The different sections of this article have been assembled into the following table of contents.
Contents
- 1.
- 1.1.
- 1.2.
- 1.3.
- 1.4.
- 1.5.
- 1.6.
- 2.
- 3.
- 3.1.
- 3.2.
- 3.3.
- 4.
- 5.
How to know if labor is approaching?
Once the third trimester of pregnancy begins, women may feel contractions. However, these contractions do not always indicate that labor is about to start. Most commonly, at the beginning of the third trimester, Braxton Hicks contractions occur. These are irregular contractions of lower intensity compared to true labor contractions.
In addition, late-pregnancy discomfort can sometimes be confused with labor. For this reason, it is important to know which symptoms appear before labor begins. Below are some of them.
Baby dropping (lightening)
A few weeks before labor, the pregnant woman may feel pelvic or vaginal discomfort. At the same time, the pressure on the rib cage is relieved, allowing the woman to breathe more easily.
This is because the baby descends and engages in the pelvis, preparing to move through the birth canal. This descent and positioning of the baby is also known as lightening.

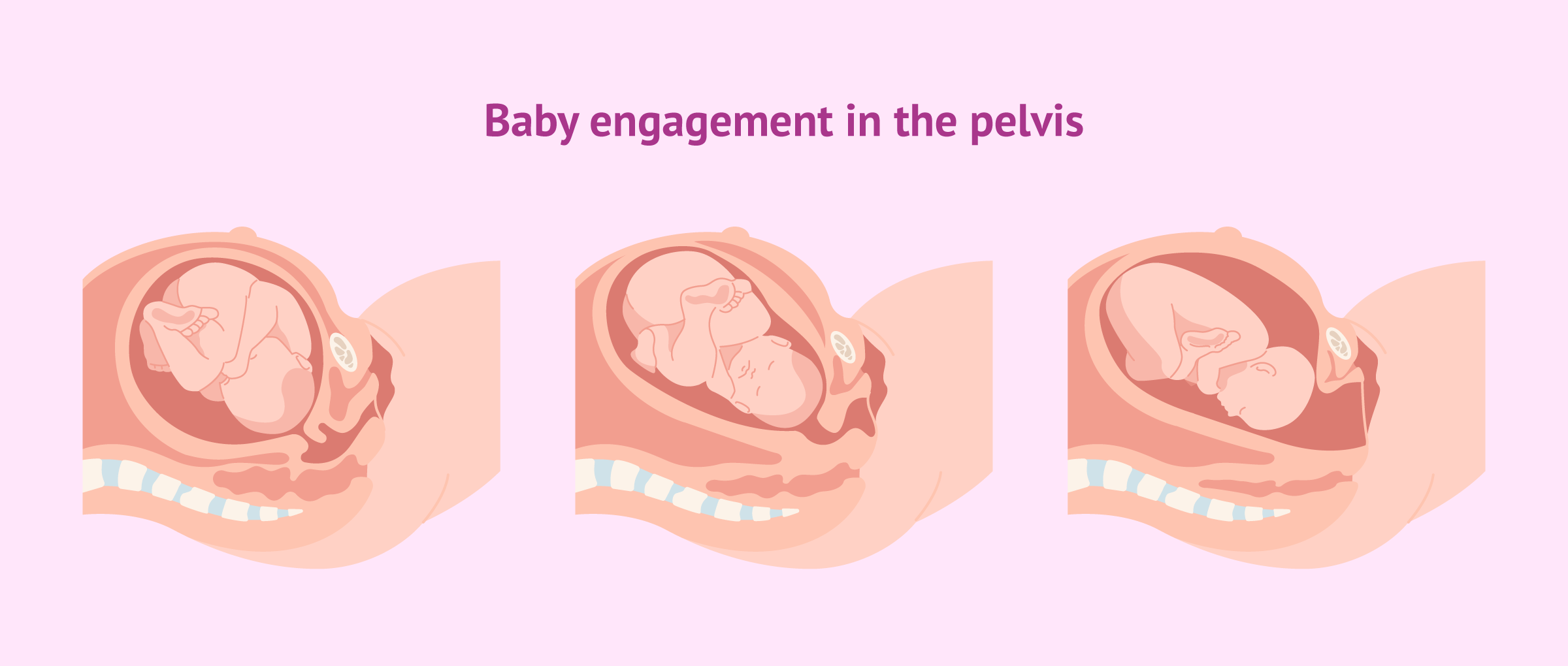
Medically, the baby is considered engaged in the pelvis when the widest part of the head has entered the pelvic inlet. If, when labor begins, the baby is already engaged, the process will be easier and faster than if the baby is not yet engaged.
Braxton Hicks contractions
These contractions begin around the third month of pregnancy, but the expectant mother will not usually feel them until later in gestation. Unlike true labor contractions, Braxton Hicks are sporadic uterine contractions.

During the last weeks of pregnancy, Braxton Hicks contractions can be mistaken for labor contractions, causing a “false alarm.” Therefore, it is important to know that labor contractions gradually increase in frequency and intensity, while Braxton Hicks, although sometimes painful, are brief.
Cervical ripening
Cervical ripening, or the maturation of the cervix, is a stage in which the cervix changes in shape, position, and consistency. The obstetrician determines the onset of labor based on cervical dilation.
If this is not the woman’s first delivery, the cervix may already be dilated by one centimeter before labor begins.
The process of cervical ripening can be accelerated through different methods:
- Traditional: evening primrose oil (may stimulate oxytocin release), acupuncture, or nipple stimulation.
- Mechanical: using dilators, Hamilton’s maneuver, or performing an amniotomy, which means rupturing the amniotic sac from the decidua.
- Pharmacological: currently the most common method, involving the administration of relaxin, oxytocin, and prostaglandins.
In any case, cervical ripening increases the likelihood of vaginal birth while reducing the rate of cesarean sections.
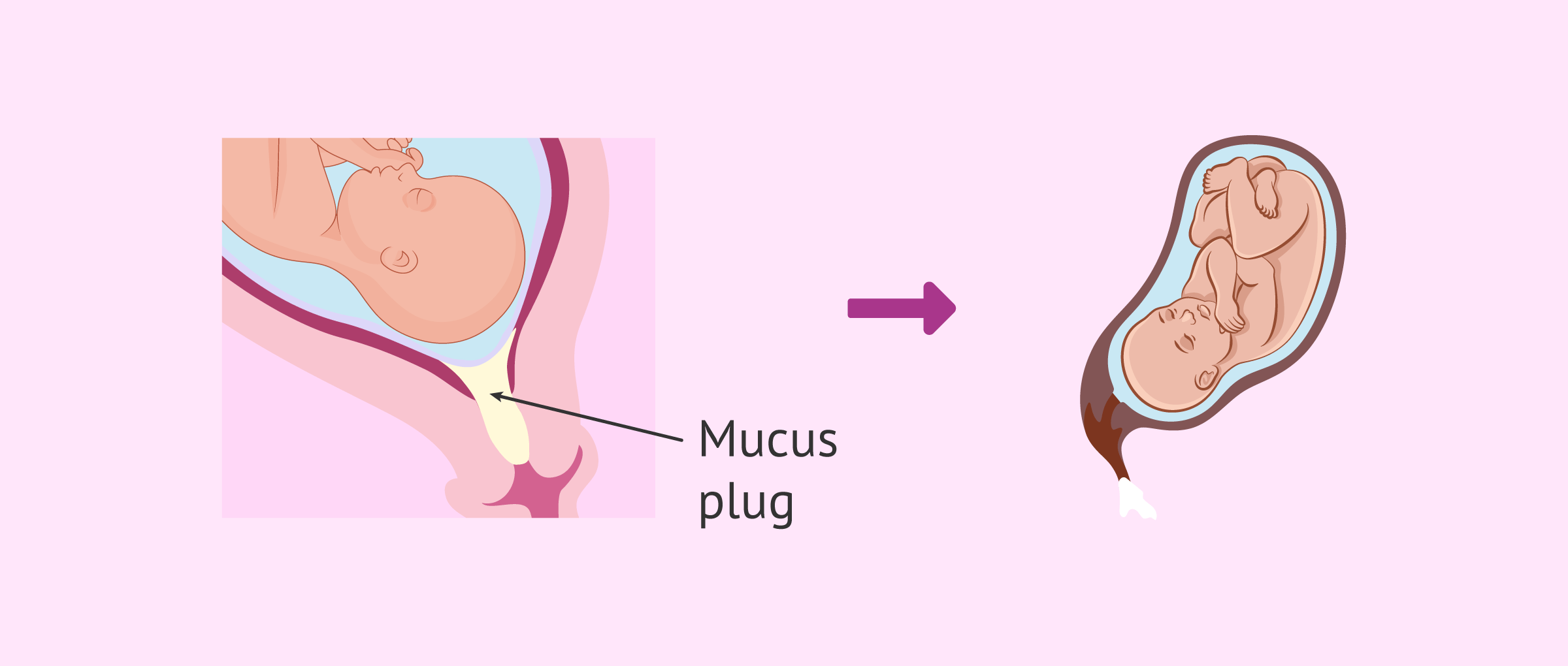
Expulsion of the mucus plug
Between the 4th and 6th weeks of pregnancy, the cervix begins producing a dense secretion known as the mucus plug. This gelatinous substance seals the cervix and protects the fetus from infections. The mucus plug also allows sexual intercourse to be carried out safely as long as the pregnancy progresses normally.
The loss of the mucus plug reflects the proximity of labor, although it is not necessarily a sign of imminent labor. The mucus plug appears as thick, sticky discharge that may be clear, yellowish, or streaked with blood due to ruptured capillaries as it passes through the cervix. This should not cause concern. It should also not be confused with the denser vaginal discharge common throughout pregnancy.
If the mucus plug is lost without contractions or rupture of membranes, it is not necessary to go to the hospital. Toward the end of pregnancy, the cervix becomes thinner and may dilate slightly due to sporadic contractions, facilitating expulsion of the mucus plug. However, this does not mean that labor will begin immediately. If the mucus plug is accompanied by heavy bleeding, immediate medical attention is required.
True labor contractions
Unlike Braxton Hicks, true labor contractions are always painful and occur with increasing frequency for at least one hour. It is recommended to go to the hospital when uterine contractions occur every 5 minutes for more than an hour. In twin pregnancies, it is advisable to go when contractions occur every 10 minutes.
As delivery approaches, contractions become more frequent and their intensity increases.
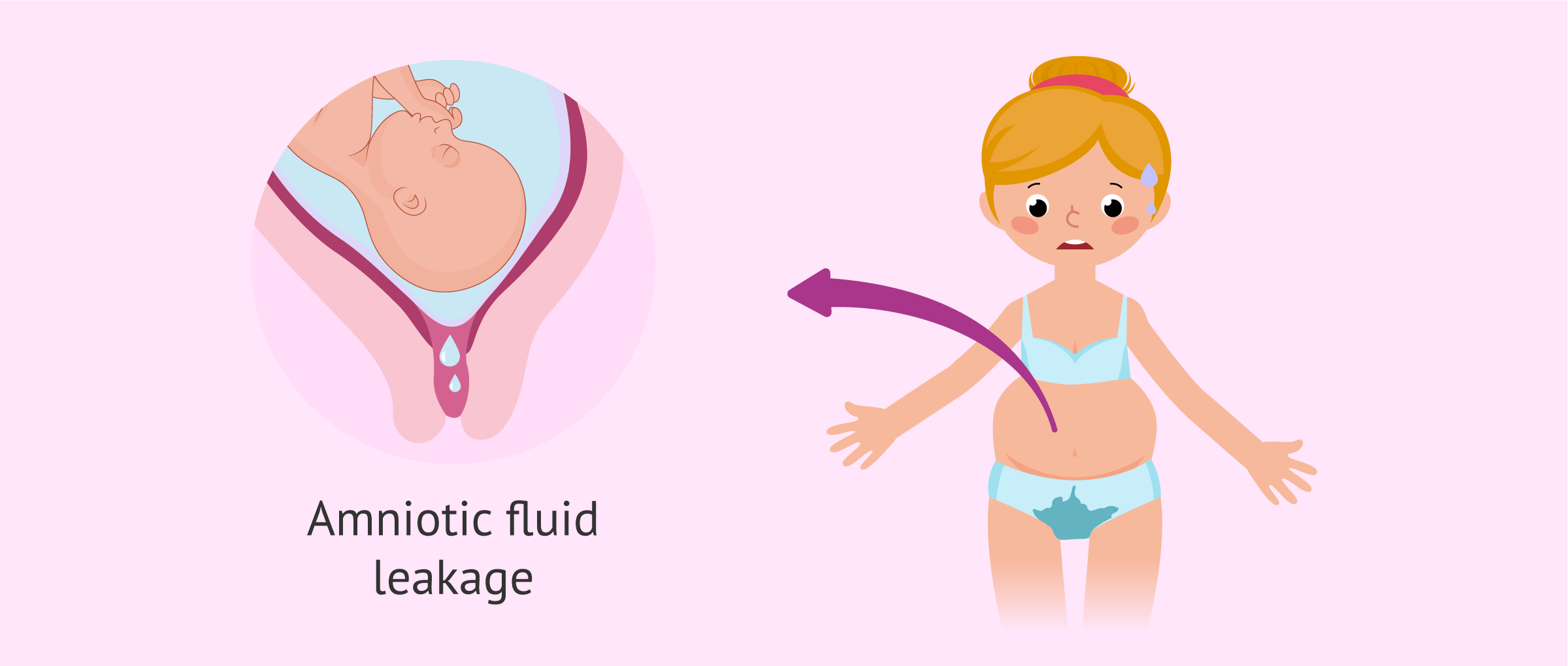
Rupture of membranes (water breaking)
The amniotic sac, which surrounds the baby and provides protection, ruptures during labor. After rupture, the amniotic fluid is released through the vagina. This is commonly known as water breaking and is noticeable due to the significant amount of fluid.
If the amniotic fluid is clear, everything is usually fine. However, it is necessary to go to the hospital because labor can start at any moment. In first pregnancies, labor may still take some time even after the waters have broken.
If the amniotic fluid is dark, this may indicate the presence of the baby’s first stool, known as meconium. This can suggest fetal distress and requires immediate medical evaluation.
Similarly, if rupture of membranes occurs before term, it is essential to go to the hospital because the baby is no longer protected and the risk of infection is high. In these cases, antibiotics may be administered to the mother. If rupture occurs before the 34th week, corticosteroids are administered to accelerate fetal lung maturation in preparation for possible preterm labor.
False alarms
Toward the end of pregnancy, the woman may be alert to any signs suggesting the onset of labor. However, false alarms are common. For this reason, it is important to distinguish between true and false labor. Some points to consider are:
- Track contraction intervals to evaluate regularity.
- Assess whether contractions are increasing in strength.
- If the pregnant woman is unable to walk during contractions, it is most likely true labor.
- Sensation of pressure in the lower back.
In any case, if the woman is uncertain about what she is experiencing, it is best to consult a specialist, who can determine whether true labor is beginning or if it is a false alarm.
FAQs from users
Can labor contractions be painless?
To answer this question, it is important to distinguish between true labor contractions and Braxton Hicks contractions.
Braxton Hicks contractions are irregular uterine contractions of low intensity which, although they can be uncomfortable, do not usually cause significant pain.
In contrast, labor contractions are regular, and as the frequency of contractions increases and the moment of delivery approaches, their intensity worsens, causing pain for the woman.
When is natural childbirth recommended and when is cesarean delivery recommended?
Childbirth is the most special and awaited moment for most pregnant women. Delivery can be done vaginally or by cesarean section.
The most physiological route is the vaginal route. However, there are circumstances in which delivery by cesarean section is indicated to safeguard the health of the mother and fetus.
There are 3 types of cesarean section:
- Elective cesarean section
- is performed in the presence of some maternal or fetal pathology such as placenta previa, breech, transverse or oblique presentation, fetal macrosomia, active infections of the birth canal, 2 previous cesarean sections, some cases of growth disturbance and multiple gestations.
- The indicated cesarean section
- is recommended in the course of labor for various alterations such as arrested dilatation or descent, cephalopelvic disproportion, arrested labor, etc.
- Cesarean section
- is recommended in the course of labor for various alterations such as arrested dilatation or descent, cephalo-pelvic disproportion, arrested labor, etc.
- Urgent cesarean section
- is one in which the life of the mother and fetus is in danger as a result of a serious acute pathology.
Are diarrhea and nausea a symptom of labor onset?
Before labor begins, the pregnant woman will be in a stage known as the prodromal or latent phase of labor. This means that the pregnant woman will notice some symptoms that are indicative that labor is about to begin.
Thus, there are women who suffer from diarrhea, cramps and nausea before giving birth. This is due to the action of prostaglandins. In addition, as the digestive tract empties, uterine contractions are more effective.
Recommended readings
However, it is also possible to experience discomfort during pregnancy that is not related to the onset of labor. In the following article, you can read more about this topic: What are the most common aches and pains during pregnancy?
We make a great effort to provide you with the highest quality information.
🙏 Please share this article if you liked it. 💜💜 You help us continue!
References
Caroline A Smith, Kate M Levett, Carmel T Collins, Hannah G Dahlen, Carolyn C Ee, Machiko Suganuma. Massage, reflexology and other manual methods for pain management in labour. Cochrane Database Syst Rev. 2018 Mar 28;3(3):CD009290 (View)
David Desseauve, Laetitia Fradet, Patrick Lacouture, Fabrice Pierre. Position for labor and birth: State of knowledge and biomechanical perspectives. Eur J Obstet Gynecol Reprod Biol. 2017 Jan;208:46-54 (View)
Edgardo Abalos, Olufemi T Oladapo, Mónica Chamillard, Virginia Díaz, Julia Pasquale, Mercedes Bonet, Joao Paulo Souza, A Metin Gülmezoglu. Duration of spontaneous labour in 'low-risk' women with 'normal' perinatal outcomes: A systematic review. Eur J Obstet Gynecol Reprod Biol. 2018 Apr;223:123-132 (View)
Vanora Hundley, Soo Downe, Sarah J Buckley. The initiation of labour at term gestation: Physiology and practice implications. Best Pract Res Clin Obstet Gynaecol. 2020 Aug;67:4-18 (View)
Wayne R Cohen, Emanuel A Friedman. Clinical evaluation of labor: an evidence- and experience-based approach. J Perinat Med. 2020 Oct 19;49(3):241-253. doi: 10.1515/jpm-2020-0256 (View)