When a woman or couple has their first child and is considering having a second, questions may arise such as how long to wait to recover from the first pregnancy and delivery or what is the ideal age difference between the two siblings.
Of course, the final decision as to when to have another child is up to the woman or couple. However, it is advisable to follow certain recommendations and medical advice to reduce possible complications, both for the mother and the baby.
Provided below is an index with the 8 points we are going to expand on in this article.
- 1.
- 2.
- 3.
- 3.1.
- 3.2.
- 4.
- 4.1.
- 4.2.
- 4.3.
- 5.
- 6.
- 7.
- 8.
Recommended time between pregnancies
After pregnancy and childbirth, a woman's body needs time to recover. The length of this recovery period can be variable depending on the particular circumstances, but having a child very close to the previous one may pose some risks.
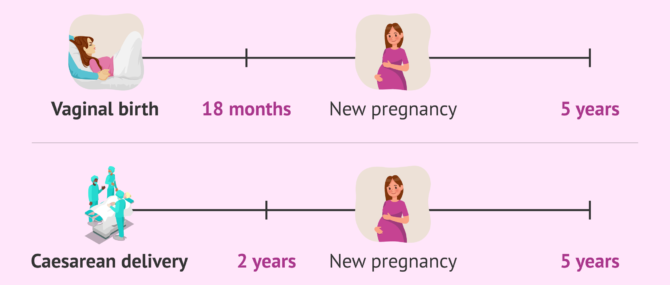
In general, it is advisable to wait at least 18 months (one and a half years) between delivery and the next pregnancy. However, this interval would be extended to 24 months (two years) if the first delivery was by cesarean section (to reduce complications due to scarring of the uterus).
In contrast, the recommendation of the World Health Organization (WHO) is to wait at least 24 months after the birth of a child before becoming pregnant again, which coincides with the recommendation for the breastfeeding period of at least 2 years.
However, on the other hand, it is not recommended to wait more than 5 years between pregnancies. At this point, it is important to mention the increased risk of complications that may arise in pregnancy if the woman is of advanced maternal age.
Nevertheless, the woman or couple must take into account their personal circumstances (health status, age, access to pregnancy control, economic situation...) and assess the risks and benefits in order to make the decision of when to have their next child.
Possible risks of two pregnancies in close succession
When a woman becomes pregnant soon after having a child, there may be more complications for her and the baby.
A time interval of less than 18 months between one delivery and the next pregnancy may increase the risk of preterm delivery and low birth weight.
Even if the woman is older than 35 years and waits only 6 months to become pregnant again after childbirth, the risk of maternal mortality may increase compared to waiting 18 months. This takes on great importance if we take into account that older women may tend to wait less time between pregnancies due to the deterioration of fertility with the passage of time.

In addition, the levels of certain compounds such as folic acid, iron or calcium should also be kept in mind. These compounds are important during pregnancy and, if they have not been allowed enough time to recover their normal values, their levels may be weakened after the previous pregnancy. Therefore, it is important to plan the new pregnancy and to take the nutritional supplements prescribed by the specialist in advance.
On the other hand, the pelvic floor needs to recover from previous pregnancy and childbirth. If sufficient time is not allowed for this and strengthening exercises (such as Kegel exercises) are not performed, problems with urinary incontinence may occur kegel exercises), there may be problems with urinary incontinence. On the other hand, if you wait more than 5 years from a delivery to become pregnant again, there would be an increased risk of preterm delivery, low birth weight and preeclampsia.
Relationship between siblings according to age difference
In addition to the medical aspects mentioned above, when planning when is the best time to have another child, it is common for the woman or couple to consider other things. Among them is the relationship the future baby will have with its older sibling.
Small age difference
When there is a small age difference between the two siblings, the following advantages may exist:
- In addition to being siblings, they will be playmates.
- Since they are at a similar stage of development, they will have similar needs and it may be easier to entertain and educate them at the same time.
- They will be able to help each other when they go to school and perhaps there is a savings in the purchase of books.
In contrast, caring for two young children of similar ages is exhausting. However, this can be an advantage in the long run: the initial effort is greater, but you only have to go through this period once to raise both children.
Greater age difference
For siblings with a greater age difference, more time can be devoted to caring for each of them since, when the baby arrives, the older one will already be more independent.
Even if there is an age difference, they can share games in different roles and some of the first child's things can be used for the second child, such as the crib, stroller, clothes, toys, etc.
However, one of the main drawbacks when the age difference is greater is possible jealousy. The older sibling will need time to assimilate that there is another person who also occupies the attention that was previously focused only on him or her.
On the other hand, in this case, the siblings will be at different stages of development and it may also be exhausting to attend to the different needs of the two.
FAQs from users
Is it necessary to wait a while for a new embryo transfer after having a child?
Jana Bechthold, gynaecologist at the Tambre clinic in Madrid, answers us in this video:
It is recommended to wait at least one year after giving birth for the next embryo transfer. The World Health Organization even recommends two years, especially if the woman had a cesarean section it is necessary to wait at least one year.
What are the advantages and disadvantages of contraceptives in breastfeeding?
The main advantage of using contraceptives during breastfeeding is to avoid an unwanted pregnancy and to prevent it from occurring too early, without the woman having recovered properly from the previous one.
As a disadvantage, it could be mentioned that some of the contraceptive methods could have some adverse effect on the woman, the baby or breastfeeding, so not all of them are valid during this period and a specialist should be consulted as to which method is the most appropriate for each particular case and when to start it.
I want to get pregnant fast after a miscarriage, is it possible?
Although the WHO recommends waiting about six months to seek pregnancy again, there are numerous studies that indicate that the sooner the pregnancy is resumed, the lower the chances of suffering a new miscarriage or other gestational complications.
The WHO recommendations are based fundamentally on emotional aspects, since miscarriage is a hard trauma and it is convenient to have overcome this grief and be prepared to face the new pregnancy with illusion. On the other hand, the studies that indicate that it is not necessary to wait to conceive again after the abortion are based on physiological aspects of the female body.
In any case, it is important to consult your doctor. Many specialists recommend waiting an average of two menstrual periods before trying again. However, this depends very much on the type of miscarriage that has occurred and the consequences of the miscarriage both physically and emotionally.
Suggested for you
If you want to know more about family planning to decide when is the right time to have a child, we recommend you to read the following article: Family planning: benefits, recommendations and methods.
On the other hand, if you want to learn more about pregnancy at an advanced age, you can access this link: How does the mother's advanced age influence pregnancy?
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Agrawal S, Chaudhary M, Das V, Agarwal A, Pandey A, Kumar N, Mishra S. Association of long and short interpregnancy intervals with maternal outcomes. J Family Med Prim Care. 2022 Jun;11(6):2917-2922. doi: 10.4103/jfmpc.jfmpc_2231_21. Epub 2022 Jun 30. PMID: 36119251; PMCID: PMC9480788. (View)
Conde-Agudelo A, Belizán JM. Maternal morbidity and mortality associated with interpregnancy interval: cross sectional study. BMJ. 2000 Nov 18;321(7271):1255-9. doi: 10.1136/bmj.321.7271.1255. PMID: 11082085; PMCID: PMC27528. (View)
Conde-Agudelo A, Belizán JM, Breman R, Brockman SC, Rosas-Bermudez A. Effect of the interpregnancy interval after an abortion on maternal and perinatal health in Latin America. Int J Gynaecol Obstet. 2005 Apr;89 Suppl 1:S34-40. doi: 10.1016/j.ijgo.2004.08.003. PMID: 15820366. (View)
Conde-Agudelo A, Rosas-Bermúdez A, Kafury-Goeta AC. Effects of birth spacing on maternal health: a systematic review. Am J Obstet Gynecol. 2007 Apr;196(4):297-308. doi: 10.1016/j.ajog.2006.05.055. PMID: 17403398. (View)
Corrigendum. BJOG. 2016 Aug;123(9):1568. doi: 10.1111/1471-0528.14191. Erratum for: BJOG. 2016 Apr;123(5):730-7. PMID: 27440609; PMCID: PMC6886033. (View)
İmamoğlu M, Şimşek D, Dinçgez B, Ünal S, Demirci A, İlhan O, İmamoğlu AG, Özçeltik G. Short interdelivery interval in modern obstetrics: Maternal and neonatal outcomes. Turk J Obstet Gynecol. 2022 Dec 13;19(4):295-301. doi: 10.4274/tjod.galenos.2022.50576. PMID: 36511629; PMCID: PMC9748857. (View)
Kangatharan C, Labram S, Bhattacharya S. Interpregnancy interval following miscarriage and adverse pregnancy outcomes: systematic review and meta-analysis. Hum Reprod Update. 2017 Mar 1;23(2):221-231. doi: 10.1093/humupd/dmw043. PMID: 27864302. (View)
Mignini LE, Carroli G, Betran AP, Fescina R, Cuesta C, Campodonico L, De Mucio B, Khan KS. Interpregnancy interval and perinatal outcomes across Latin America from 1990 to 2009: a large multi-country study. BJOG. 2016 Apr;123(5):730-7. doi: 10.1111/1471-0528.13625. Epub 2015 Sep 24. Erratum in: BJOG. 2016 Aug;123(9):1568. PMID: 26399217; PMCID: PMC4949506. (View)
Mühlrad H, Björkegren E, Haraldson P, Bohm-Starke N, Kopp Kallner H, Brismar Wendel S. Interpregnancy interval and maternal and neonatal morbidity: a nationwide cohort study. Sci Rep. 2022 Oct 18;12(1):17402. doi: 10.1038/s41598-022-22290-1. PMID: 36258030; PMCID: PMC9579163. (View)
Schummers L, Hutcheon JA, Hernandez-Diaz S, Williams PL, Hacker MR, VanderWeele TJ, Norman WV. Association of Short Interpregnancy Interval With Pregnancy Outcomes According to Maternal Age. JAMA Intern Med. 2018 Dec 1;178(12):1661-1670. doi: 10.1001/jamainternmed.2018.4696. PMID: 30383085; PMCID: PMC6583597. (View)
Wang Y, Zeng C, Chen Y, Yang L, Tian D, Liu X, Lin Y. Short interpregnancy interval can lead to adverse pregnancy outcomes: A meta-analysis. Front Med (Lausanne). 2022 Nov 30;9:922053. doi: 10.3389/fmed.2022.922053. PMID: 36530890; PMCID: PMC9747778. (View)
World Health Organization. Report of a WHO Technical Consultation on Birth Spacing, Geneva, Switzerland, 13-15 June 2005. Geneva: WHO; (2007). (View)
FAQs from users: 'Is it necessary to wait a while for a new embryo transfer after having a child?', 'What are the advantages and disadvantages of contraceptives in breastfeeding?' and 'I want to get pregnant fast after a miscarriage, is it possible?'.




My first baby turns 1 year old on September this year and now I’m 32 weeks pregnant… But now I’m totally scared of becoming a mother again, of whom I might become and all that stuff. I mean, I don’t know how I will manage having two children because my husband works a lot and I spend many hours by myself at home… Is there anyone here on the same situation? Please, I need some advice.