The placenta is a maternal-fetal organ that develops during pregnancy, is found in the uterus and is responsible for meeting the basic needs of the fetus through the mother: breathing, feeding and excretion.
Some problems during pregnancy can arise as a result of alterations in the placenta. One of these cases is placenta previa, which occurs when the placenta grows in the lowest part of the uterus and covers all or part of the opening of the cervix.
Provided below is an index with the 10 points we are going to expand on in this article.
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 6.1.
- 6.2.
- 6.3.
- 6.4.
- 6.5.
- 7.
- 8.
- 9.
- 10.
Types of placenta previa
As the pregnancy progresses and the uterus grows, the placenta moves through the uterus. During the first months of pregnancy, it is common for the placenta to be in the lower part of the uterus, but as the weeks progress, it grows and is located in the upper part.
Once the third trimester of pregnancy arrives, the placenta measures about 22 cm and weighs about 0.5 kg, and must already be at the top of the uterus to clear the birth canal.
If this does not happen, there will be a placenta previa problem, in which the following types can be differentiated:
- Low lying placenta
- the placenta is in the lower segment of the uterus but does not reach the opening of the cervix.
- Marginal previa
- the placenta is next to the cervix but does not cover the opening.
- Partial previa
- the placenta covers part of the cervical opening.
- Complete previa
- the placenta covers the entire cervical opening. This type is also known as type IV placenta previa.
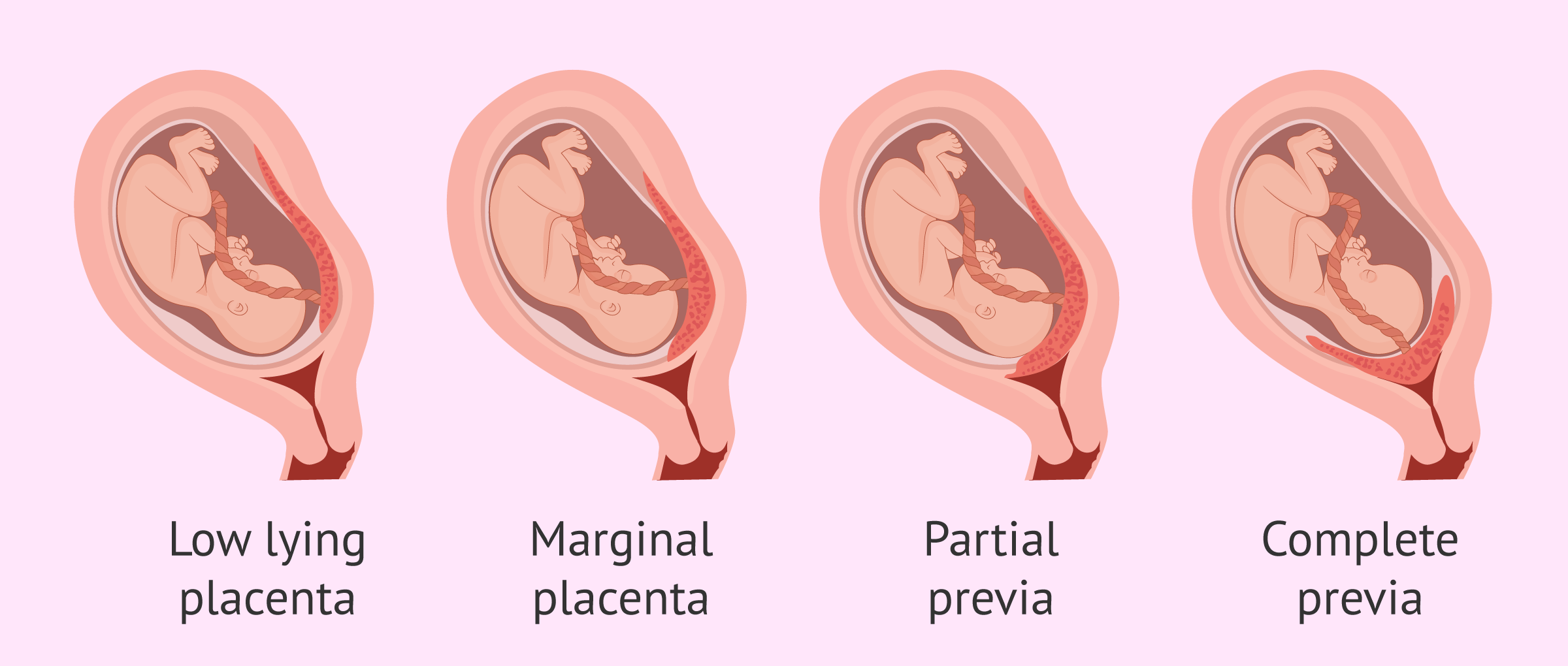
Therefore, the different types of placenta previa are distinguished depending on the severity of uterine obstruction. Nevertheless, some specialists only differentiate between minor or low-lying placenta previa and complete or major placenta previa.
What are the causes of placenta previa?
The exact cause of placenta previa is unknown. The most common belief is that this placental abnormality is related to uterine causes or to alterations in the placenta itself.
However, there are some risk factors that predispose women to this complication. They are listed below:
- Uterine malformations
- Twin pregnancy or multiple pregnancy
- Having had several previous pregnancies
- Short time between two births
- Having had a previous cesarean delivery
- Uterine scars from previous abortions or surgeries
- Advanced maternal age
- Tobacco and cocaine abuse

Placenta previa occurs in 1 in 200 pregnant women in the third trimester of gestation.
How is placenta previa diagnosed?
The placenta previa is diagnosed by ultrasound, which shows whether the position of the placenta is correct or not.
If this condition is detected before the third trimester of pregnancy, there is no cause for alarm, as the placenta is likely to vary in position as the uterus enlarges.
Only 30% of women with placenta previa before the 24th week of pregnancy still keep it in that position at the time of delivery.
If the woman has vaginal bleeding after 20 weeks, it is necessary to go to the gynecologist to perform an ultrasound and check whether it is due to a previous placenta or some other problem.

The evolution of this complication will depend on the intensity of the bleeding and the exact week of pregnancy. The likelihood of having placenta previa at the time of delivery increases with gestational age.
Specifically, about 70% of women will have placenta previa at the time of delivery if the diagnosis is made from 30 weeks. It is also more likely to persist if it is a complete placenta previa, rather than a marginal or partial placenta.
Symptoms and Treatment
Most women with placenta previa before the 20th week of gestation remain asymptomatic.
Symptoms of placenta previa usually occur when placenta previa persists later in pregnancy, starting at 20 weeks. The main symptoms are painless vaginal bleeding with bright red blood and variable intensity.
Bleeding occurs because the cervix begins to dilate and ruptures the blood vessels in the placenta and the area where it is implanted. This bleeding may stop on its own and start again a few days later. Sometimes vaginal bleeding does not occur until labor begins.
Depending on the intensity of the vaginal bleeding and the type of placenta previa, the procedure will be as follows:
- Mild bleeding and low or marginal placenta previa
- the doctor will order absolute bed rest, to reduce activities and rest the pelvis, which means not having sex or using tampons.
- Heavy bleeding and partial or total placenta previa
- the woman is likely to be hospitalized for more monitoring and treated with blood transfusions. Increased bleeding can put the mother's and baby's health at risk.
The doctor will then have to make a decision about the type of delivery, which in most cases will be scheduled.
Childbirth with placenta previa
The way to proceed when giving birth with placenta previa will depend on the type and severity.
In case of pregnancy with uncomplicated placenta previa, a vaginal delivery or cesarean section is scheduled around 37 weeks. Carrying a pregnancy to term is not recommended as the risk associated with placenta previa could be much worse than having a preterm birth. For example, an emergency cesarean section should be performed if severe bleeding occurs in the last weeks of gestation.
Generally, most women with partial or total placenta previa will give birth through a cesarean section, as a vaginal delivery could cause heavy bleeding that could be deadly to the mother and baby.
In case of pregnancy with placenta previa that presents abundant bleeding and other risk factors, a cesarean section will be performed if the woman is at least in the 36th week of gestation. Before this, corticosteroids may be needed to speed up the fetal lung maturation process.

If the woman is less than 35 weeks pregnant, she will remain hospitalized to control bleeding and, in case of fetal distress and/or unstoppable bleeding, a c-section will also be performed.
FAQs from users
What are the signs and symptoms of placenta previa during pregnancy?
Placenta previa is a pregnancy problem in which placenta grows in the lower part of the cervix causing a complete or partial obstruction of its opening.
The main symptom is sudden painless vaginal bleeding. It is detected by ultrasound, which shows the position of the placenta.
It is convenient to have an exhaustive ultrasound control in these cases in order to avoid premature birth.
Sometimes it may be necessary to perform an emergency caesarean section.
Is it possible to have a vaginal delivery with placenta previa?
Is it possible to have a vaginal delivery with placenta previa?
This depends on the type of placenta previa. If it is a complete or partial placenta previa, but with a border less than 2 cm from the exit orifice of the cervix, the birth canal will necessarily be a cesarean section.
On the other hand, if the edge of the placenta is more than 2 cm from the cervix outlet, vaginal delivery is possible. In this case, if any complications arise during delivery or there is bleeding, a cesarean section should be performed immediately.
What complications can arise in pregnancy with a placenta praevia?
The main complication is heavy bleeding that may occur before or during childbirth. Bulky blood loss is life-threatening to the mother and fetus. Moreover, in case of an emergency cesarean section, the baby may be born very prematurely, without its major organs, such as the lungs, having developed.
Another much feared complication is the likelihood of the placenta praevia becoming a placenta accreta. This happens when the placenta implants deeply in the uterus and does not finish taking off at the time of delivery, which can cause massive bleeding and have to resort to a hysterectomy (removal of the uterus).
What is occlusive placenta previa?
Occlusive placenta previa is a type of placenta previa that is also known as complete placenta previa. This means that the placenta grows in the lowest part of the uterus, completely covering the cervical opening.

Women with this condition will not be able to deliver vaginally and will need to have a cesarean section.
What care should be taken during pregnancy with placenta previa?
When a case of placenta previa is diagnosed, the specialist usually recommends avoiding physical exertion and leading a calm lifestyle. Additionally, it is generally advised to avoid sexual intercourse if placenta previa is present.
Long trips, especially abroad, are also not recommended during pregnancy with placenta previa, nor is becoming overly stressed or exhausted.

If the pregnant woman experiences vaginal bleeding, she should go to the emergency room as soon as possible.
Recommended readings
Throughout this post, we have discussed the different modes of delivery. If you want to learn more details about this topic, we recommend continuing to read here: Is natural childbirth or cesarean section better? - Advantages and disadvantages.
On the other hand, to learn more about the functioning of the placenta and other associated pathologies, you can visit the following article: How is the placenta and umbilical cord formed?
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Adeyemi Adebola Okunowo, Ephraim Okwudiri Ohazurike, Fatimah Murtazha Habeebu-Adeyemi. Undiagnosed placenta praevia percreta: A rare case report and review of management. Niger Postgrad Med J. 2019 Jan-Mar;26(1):61-64. doi: 10.4103/npmj.npmj_191_18
Eric Jauniaux, Lene Grønbeck, Catey Bunce, Jens Langhoff-Roos, Sally L Collins. Epidemiology of placenta previa accreta: a systematic review and meta-analysis. BMJ Open. 2019 Nov 12;9(11):e031193. doi: 10.1136/bmjopen-2019-031193 (View)
FengXiang Yao, YuBo Shi, HuiQing Ding, Min Yang, YuTing You. Total placenta previa and partial/marginal placenta previa. Taiwan J Obstet Gynecol. 2022 Sep;61(5):913. doi: 10.1016/j.tjog.2022.06.008 (View)
Hee-Sun Park, Hyun-Seok Cho. Management of massive hemorrhage in pregnant women with placenta previa. Anesth Pain Med (Seoul). 2020 Oct 30;15(4):409-416. doi: 10.17085/apm.20076 (View)
Satoru Takeda, Jun Takeda, Yoshihiko Murayama. Placenta Previa Accreta Spectrum: Cesarean Hysterectomy. Surg J (N Y). 2021 May 25;7(Suppl 1):S28-S37. doi: 10.1055/s-0040-1721492. eCollection 2021 Dec (View)
Shinya Matsuzaki, Yoshikazu Nagase, Yutaka Ueda, Mamoru Kakuda, Michihide Maeda, Satoko Matsuzaki, Shoji Kamiura. Placenta Previa Complicated with Endometriosis: Contemporary Clinical Management, Molecular Mechanisms, and Future Research Opportunities. Biomedicines. 2021 Oct 26;9(11):1536. doi: 10.3390/biomedicines9111536 (View)
Xueyin Li, Yun Feng. Complete placenta previa in the second trimester: clinical and sonographic factors associated with its resolution. Ginekol Pol. 2019;90(9):539-543. doi: 10.5603/GP.2019.0093 (View)
FAQs from users: 'What are the signs and symptoms of placenta previa during pregnancy?', 'Is it possible to have a vaginal delivery with placenta previa?', 'What complications can arise in pregnancy with a placenta praevia?', 'What is occlusive placenta previa?' and 'What care should be taken during pregnancy with placenta previa?'.
Authors and contributors



Find the latest news on assisted reproduction in our channels.
