Ovarian hyperstimulation syndrome (OHSS) is a complication that can occur after ovarian stimulation treatments in assisted reproduction techniques.
Specifically, OHSS is related to chorionic gonadotropin (hCG), the hormone administered to trigger ovulation about 36 hours before follicular puncture in in vitro fertilization (IVF) cycles.
Normally, OHSS is mild but can lead to serious complications requiring hospitalization of the patient.
Provided below is an index with the 8 points we are going to expand on in this article.
- 1.
- 2.
- 2.1.
- 3.
- 3.1.
- 3.2.
- 4.
- 4.1.
- 4.2.
- 4.3.
- 5.
- 6.
- 7.
- 8.
When does OHSS occur?
OHSS can occur after ovarian stimulation is performed in assisted reproduction treatments.
The hCG hormone is typically administered in IVF cycles to induce final follicle maturation and ovulation following controlled ovarian stimulation. However, hCG is the main trigger for OHSS, as it is associated with the increased vascular permeability and outflow of fluid into the intercellular space characteristic of OHSS.
Considering undergoing a fertility treatment? By getting your individual Fertility Report your will see different clinics especially selected for you out of the pool of clinics that meet our strict quality criteria. Moreover, it will offer you a comparison between the fees and conditions each clinic offers in order for you to make a well informed choice.
Because of this, there is early OHSS that can appear around one week after hCG administration. In contrast, late OHSS appears after 10 days after hCG injection and is related to the increase in hCG produced by the embryo if implantation has occurred.
OHSS Prevention
The first preventive measure to be taken against OHSS is to identify patients who have a higher risk of developing this syndrome after ovarian stimulation. To do this, it is necessary to evaluate in each patient the risk factors for OHSS, among which are:
- Young age, especially under 30 years old.
- Low BMI.
- Polycystic ovary syndrome (PCOS).
- High antral follicle count.
- Previous OHSS.
- Elevated estradiol level (>2500 pg/ml on the day of hCG administration), or rising rapidly during stimulation.

Therefore, with these higher risk patients, special care must be taken with ovarian stimulation, personalizing the protocol and the dose for stimulation in each one of them, and carrying out exhaustive control through analyses and ultrasound scans.
However, this follow-up should be performed on all patients during ovarian stimulation, regardless of their risk, to assess their hormone levels and their response to stimulation. In this way, the specialist would be able to quickly detect an excessive ovarian response in the patient.
Strategies to prevent OHSS
One option to prevent OHSS, within the customization of stimulation protocols, is to perform ovarian stimulation with GnRH antagonists and ovulation induction with a GnRH agonist. This avoids administering hCG to induce ovulation and effectively reduces the risk of OHSS.
In patients with polycystic ovarian syndrome (PCOS), in vitro maturation (IVM) of oocytes can be performed. This technique does not require ovarian stimulation or is administered at low doses. However, IVM is not incorporated into the routine of most fertility clinics and has not been shown to have better results than conventional IVF.
As an alternative to prevent worsening of OHSS that would entail gestation and late OHSS, embryos obtained in the cycle can be vitrified and transferred in a subsequent cycle when the OHSS has completely subsided.
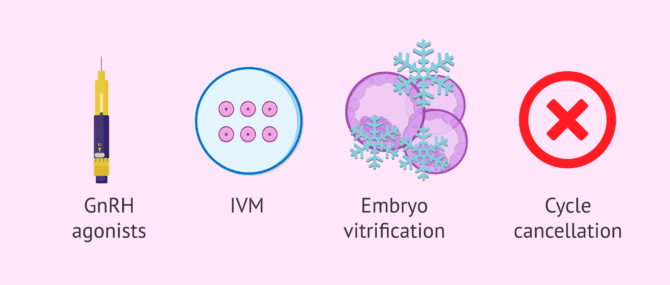
In addition, the specialist may choose on certain occasions to cancel the cycle to avoid greater risk to the patient.
OHSS Degrees
In cases where OHSS occurs after ovarian stimulation, it is most often mild. The patient will have enlarged ovaries and elevated blood estradiol levels. In addition, the woman may experience symptoms such as nausea, vomiting, and mild abdominal distention.
Although most cases of OHSS are mild, there are 4% where the OHSS is moderate. In addition to the above symptoms, ascites (accumulation of fluid in the abdomen) cause increased abdominal distention and discomfort in the patient's abdominal area.
However, the clinical picture may progress to a more severe manifestation of OHSS. Increased vascular permeability can make the blood more viscous, so there will be more risk of thrombotic phenomena. OHS can also lead to liver and kidney problems and pleural effusion (accumulation of fluid in the pleura lining the lungs and chest cavity).
Furthermore, complications such as ovarian torsion or rupture of an ovarian cyst can occur, although this is not common.
OHSS monitoring
It is very important to monitor the evolution of the OHSS, even if it is mild, in order to quickly detect a worsening that may compromise the patient's life.
For this reason, women should pay attention to aspects such as the following:
- Sudden changes in your weight or waist size.
- Decrease in urine volume.
- Difficulty breathing.
- Pain, especially in the legs.

In addition, in moderate cases of OHSS, frequent ultrasounds and tests are performed to monitor the evolution of the OHSS and its possible complications.
Mild OHSS usually remits after 48-72 hours if there is no gestation and complete remission occurs with the onset of menstruation. If gestation has occurred, OHSS may be prolonged and worsen the clinical picture.
Treatment of OHSS
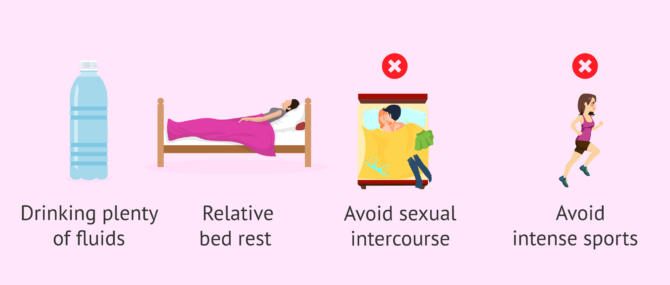
When the patient presents mild or moderate OHS, it is recommended:
- Drink plenty of fluids.
- Relative rest.
- Do not practice intense exercise.
- Do not have sexual relations.
The specialist may also advise the administration of certain analgesics or other medications to alleviate discomfort.
In the most severe cases of OHSS, the patient may need to be hospitalized. In this way, the woman will be more closely monitored and intravenous fluids can be administered, as well as any medications that the physician deems appropriate.
In addition, interventions such as a paracentesis may be performed in the hospital to remove fluid accumulated in the abdomen if necessary, and complications such as rupture of an ovarian cyst or renal and/or pulmonary problems may be addressed.
FAQs from users
What risk do I have if I get pregnant with Ovarian Hyperstimulation Syndrome (OHSS)?
Ovarian hyperstimulation syndrome (OHSS) can occur in women who have been under hormonal treatment for assisted reproduction.
Usually, OHSS goes away within a few days after treatment, but if a woman becomes pregnant it can get worse and last longer, becoming severe OHSS.
However, OHSS is very rare nowadays, since if the patient is at risk of suffering it, it is decided not to transfer the embryos and frozen for later cycles where there is no risk.
Read more
Will I have ovarian hyperstimulation syndrome (OHSS) if I undergo ovarian stimulation and I am under 30 years old?
You do not have to suffer from ovarian hyperstimulation syndrome, even if you are younger than 30 years old. Age is indeed a risk factor for OHSS, but not all young patients who undergo ovarian stimulation develop OHSS.
Fortunately, there are several strategies to avoid OHSS and, in the event of OHSS, one would choose to vitrify the embryos to avoid gestation in the same cycle, since pregnancy would worsen the OHSS.
Can I do sports if I have mild ovarian hyperstimulation syndrome?
No, it is recommended that you avoid sports and sexual intercourse, even if the ovarian hyperstimulation syndrome is mild. In fact, sports should be avoided after any IVF treatment, even if there is no OHSS.
The reason is that the ovaries are enlarged and may increase the risk of ovarian torsion, i.e. the ovaries rotate their position.
Recommended readings
If you want to continue reading more in-depth about ovarian stimulation, we recommend you to visit the following link: What is ovarian stimulation - Process, medications, and symptoms.
On the other hand, if you want to learn more about polycystic ovary syndrome, you can read the following article: Polycystic ovary syndrome (PCOS): causes, symptoms, and treatment.
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Blumenfeld Z. The Ovarian Hyperstimulation Syndrome. Vitam Horm. 2018;107:423-451.
Nastri CO, Teixeira DM, Moroni RM, Leitão VM, Martins WP. Ovarian hyperstimulation syndrome: pathophysiology, staging, prediction and prevention. Ultrasound Obstet Gynecol. 2015 Apr;45(4):377-93.
Nelson SM. Prevention and management of ovarian hyperstimulation syndrome. Thromb Res. 2017 Mar;151 Suppl 1:S61-S64.
Petrenko AP, Castelo-Branco C, Marshalov DV, Salov IA, Shifman EM. Ovarian hyperstimulation syndrome. A new look at an old problem. Gynecol Endocrinol. 2019 Aug;35(8):651-656.
Practice Committee of the American Society for Reproductive Medicine. Prevention treatment of moderate and severe ovarian hyperstimulation syndrome: a guideline. Fertil Steril. 2016 Dec;106(7):1634-1647.
Timmons D, Montrief T, Koyfman A, Long B. Ovarian hyperstimulation syndrome: A review for emergency clinicians. Am J Emerg Med. 2019 Aug;37(8):1577-1584.
FAQs from users: 'What risk do I have if I get pregnant with Ovarian Hyperstimulation Syndrome (OHSS)?', 'Will I have ovarian hyperstimulation syndrome (OHSS) if I undergo ovarian stimulation and I am under 30 years old?' and 'Can I do sports if I have mild ovarian hyperstimulation syndrome?'.
Authors and contributors



More information about Cristina Algarra Goosman

More information about Michelle Lorraine Embleton

I have developed mild OHSS and the embryos have been frozen. I don’t know if this is the best thing to do as it is a mild case.
Hi Belinda
Cryo-preserving the embryos instead of transferring them in the same cycle is a strategy that is performed even if the OHSS is mild. In this way, a possible gestation in that cycle is avoided, since it would worsen the OHSS due to the hCG that the embryo would produce.
I hope this helps
Best regards.
How do I know if I have OHSS?
Hello kimberly,
There are different symptoms that can be indicative of ovarian hyperstimulation, for example, changes in weight, leg pain, or shortness of breath.
If you identify any of these symptoms or your doctor has informed you of the possibility of developing them, I recommend that you go to him so that he can monitor and treat them if necessary.
I hope I have helped you.
Best regards.
Hi, I have PCOS and I have been told that before my IVF it is very likely that I will develop OHSS, the truth is that I am a little scared and I do not know what the consequences of having it would be.
Hello Natasha,
There are different levels of OHSS, the probability of developing it or not will depend on different factors to be studied by your doctor. If he/she has considered that you are at risk of developing ovarian hyperstimulation with IVF stimulation, the doctors will be more aware of your results and symptoms in order to be able to control it in case it happens.
If ovarian hyperstimulation occurs, the most normal thing to do is to stop the cycle and start again in the next cycle.
I hope I have helped you,
Best regards