Ovarian hyperstimulation syndrome (OHSS) is a complication that can occur in assisted reproduction treatments. It is characterized by an abnormally high response of the ovary to the medication administered, especially in in vitro fertilization (IVF).
The mechanisms by which this exaggerated response to drugs is triggered remain unknown. However, there is no doubt that OHSS has its origin in the administration of human chorionic gonadotropin (hCG) used in ovarian stimulation cycles.
The identification of the risks that favor the appearance of this syndrome is as important as the ultrasound and hormonal follow-ups that will allow the doctor to prevent and/or manage this alteration.
If the patient manages to become pregnant during treatment, OHSS may become severe and have serious consequences.
Provided below is an index with the 14 points we are going to expand on in this article.
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 6.1.
- 7.
- 7.1.
- 7.2.
- 7.3.
- 7.4.
- 7.5.
- 8.
- 8.1.
- 8.2.
- 9.
- 10.
- 10.1.
- 10.2.
- 10.3.
- 10.4.
- 10.5.
- 10.6.
- 11.
- 12.
- 13.
- 14.
What is OHSS and when does it occur?
Ovarian hyperstimulation syndrome is an alteration that can arise in assisted reproduction treatments and can make the process of assisted reproduction more difficult.
The syndrome appears more often in in vitro fertilization (IVF) treatments, compared to artificial insemination (AI). This is because the hormone doses administered in IVF are higher than those of AI.
During IVF, the patient is given hormonal medication. These injections are intended to increase the number of follicles that will reach maturity. In this way, more than one egg matures, which is what happens monthly in a woman's natural cycle.
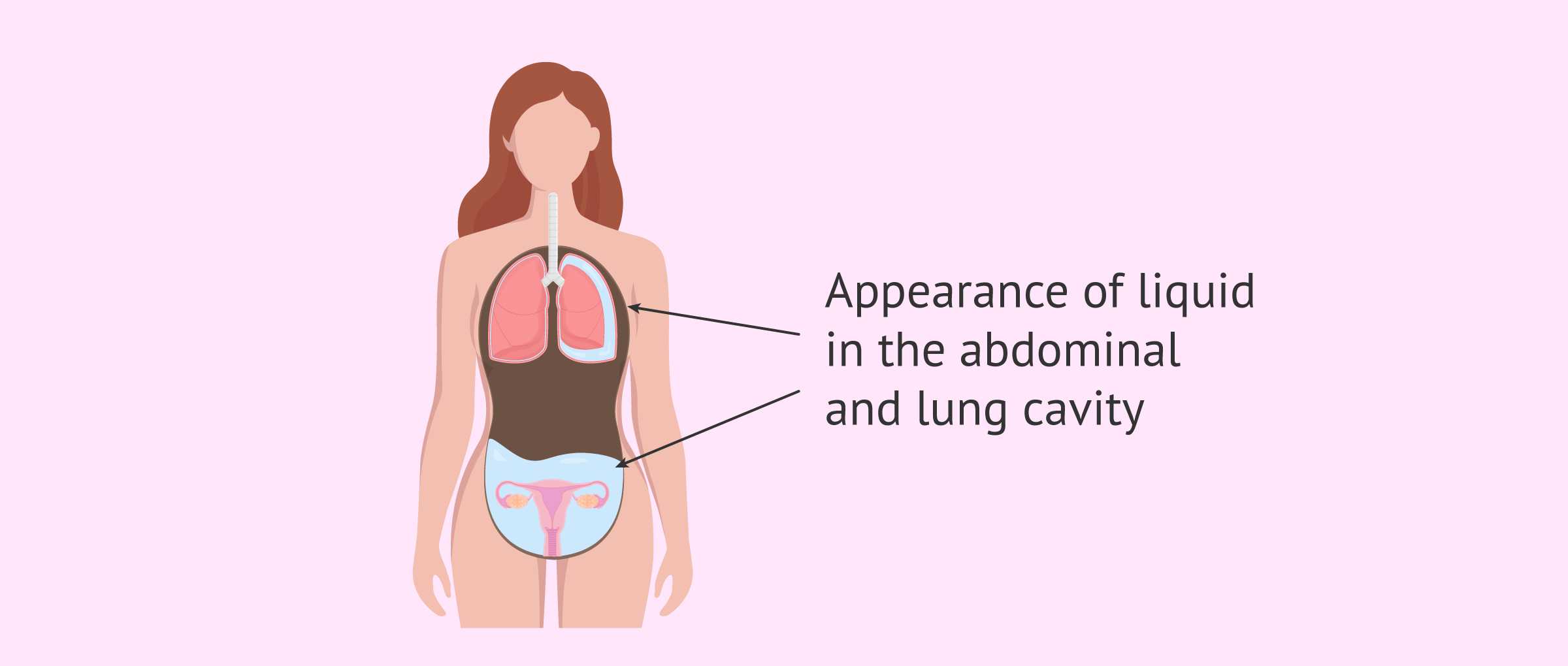
When this medication stimulates the ovary more strongly than expected, it may cause the ovaries to overgrow and become filled with fluid.
During fertility treatments, the human chorionic hormone hCG will be administered hours before the follicular puncture. It is known that, in certain patients, hCG is the source of OHSS.
The most significant consequence of OHS is the release of an abnormal volume of fluid into the abdominal and lung cavity. This fact is the trigger that can unbalance the hemostasis of the woman's body and lead to different alterations that we will see in this article.
OHSS is a very short-lived syndrome because it disappears with menstruation, when the hormone levels of the woman's cycle are restored. In any case, it must be controlled by a doctor who follows the patient by means of transvaginal ultrasound and hormonal analysis of estradiol, in case it leads to other more serious complications.
At present, serious OHSS cases are rare, as the types of ovarian stimulation protocols used and the follow-up during follicular development make it possible to avoid OHSS.
Causes of the Syndrome
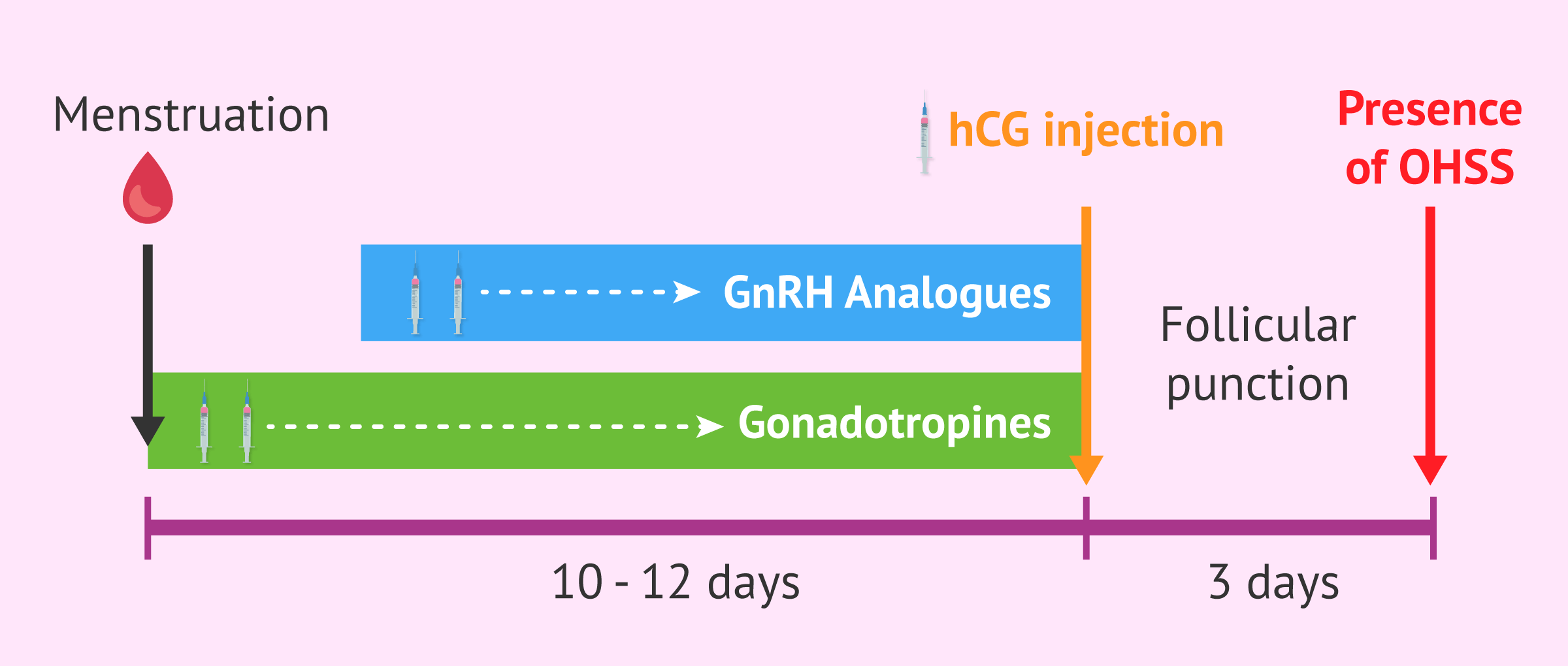
The causes of this reaction to hormone stimulation are not known. However, it is known that OHSS is only triggered in the luteal phase of controlled ovarian stimulation cycles, after the administration of hCG. Only in the presence of this hormone occurs the excessive response that causes this syndrome.
The administration of hCG is the last step in ovarian stimulation and the introduction to follicular puncture. This application, also known as a trigger, is performed 36 hours before the punction.
The purpose of this hormone is to produce changes in the structure of the follicles and the maturation of the eggs so that they are optimal for fertilization. However, in patients at risk for OHSS, hCG will be the trigger for this syndrome.
The trigger also promotes the release of certain substances that increase the permeability of the blood vessels. This causes the excessive release of fluids out of the bloodstream. In this way, the function of the hepatic, haematological, renal and respiratory systems can be compromised.
The syndrome will not occur immediately after the administration of hCG, but the patient will start noticing its symptoms days or weeks after the administration of hCG.
Classification of ovarian hyperstimulation syndrome
The original OHSS classification has undergone several changes and modifications, but we can now speak of 3 types according to the level of severity:
- Mild: characterized by elevated estradiol and progesterone levels and slightly enlarged ovaries.
- Moderate: in addition to the hormonal changes and the increase in the size of the ovary, the patient presents discomfort and enlargement of the abdominal area.
- Severe: characterized by an exaggeratedly large diameter of the ovary and totally altered hormone levels. In addition, the patient's daily weight gain is remarkable due to the excess fluid in her abdominal and thoracic cavity. All of which can cause a woman to have kidney, liver and thrombotic problems.

We can also classify OHSS according to the time it takes for the syndrome to manifest itself. Depending on how long it takes for the syndrome to debut we will be able to distinguish between:
- Early OHSS: appears 3-7 days after administration of hCG, after ovarian puncture.
- Late OHSS: it appears 12 and 17 days after the injection of hCG. This type of OHSS usually occurs when there is gestation because the embryonic sac produces hCG.
Symptoms of OHSS
OHSS appears in 0.6-10% of women who undergo ovarian stimulation cycles. Below, we will look at the symptoms related to this syndrome depending on the severity of the syndrome.
Most women who have mild or moderate OHSS show symptoms such as:
- Swelling and mild pain in the abdomen
- Weight gain
- Nausea or vomiting
- Diarrhea
- Mild to moderate abdominal pain
Although rare, serious cases only have an incidence of 0.5-2%, and are attended by very characteristic symptoms:
- Faster weight gain: over 4.5 kg in 3-5 days
- Ascites- fluid accumulation in the abdomen
- Hypotension and tachycardia - increased heart rate
- Difficulty breathing
- Urinating less frequently
- Alteration of the values of the tests that evaluate vital functions, such as the renal and hepatic function

Early diagnosis of OHSS is very important to avoid possible complications that may arise, as they could endanger the patient's life. Therefore, it is very important to monitor the patient's symptoms closely.
Complications of the Syndrome
The most significant consequence of OHSS is the release of an abnormal volume of fluid into the abdominal and lung cavity. The most common complications are:
- Fluid accumulation around the lungs - which can lead to breathing problems
- Ovarian torsion: the high amount of abdominal fluid can cause the ovary to float in the fluid and turn over
- Electrolyte imbalance: due to the high amount of fluid leaving the bloodstream can alter salt levels
- Decreased frequency and volume of urinations: as much of the fluid is released into the abdominal cavity, a decrease in urine volume and frequency of urination can occur, leading to kidney failure

There are also other risks to be considered, since if an ovarian cyst ruptures, internal bleeding can occur that can endanger the woman. In addition, it should be noted that if a woman becomes pregnant, a miscarriage may occur due to complications from OHSS.
Risk factors for OHSS
Although any woman undergoing ovarian hyperstimulation treatment is susceptible to suffering OHS, a number of risk factors have been described that favor the manifestation of OHSS. The risk factors that predispose to the manifestation of OHSS are:
- Age: the ovaries of young women (under 30 years old) have a greater number of receptors for gonadotropic hormones or a greater number of follicles that make them more susceptible to this syndrome.
- A low muscle mass index: this syndrome has been described in greater proportion in thin women. However, on this point there is some discrepancy, as many authors have not found the relationship between thinness and OHSS.
- Polycystic ovary syndrome (PCOS): there is a clear association between PCOS and OHSS. Women with PCOS are more likely to develop OHSS when they are hyperstimulated.
- The woman has been pregnant before: those women who have been pregnant before are more likely to have OHSS than those who have never been pregnant.
- Multiple pregnancy: hCG, the hormone that promotes the appearance of OHSS, will double if the patient becomes pregnant with twins, worsening the evolution of the syndrome.

What are the signs of a possible OHSS?
OHSS is not easy to predict during ovarian stimulation. However, there are certain signs and signals that may indicate to the doctor that the patient may be at risk for OHSS, such as:
- Elevated serum estradiol: during the process of ovarian stimulation, the woman must come every 2 days for ultrasound controls to see the evolution of her follicles. In these controls, the concentration of estradiol in the blood is also checked. This hormone is secreted by the ovarian follicles. Levels greater than 25000pg/ml or a rapid increase in a short time can put the doctor on alert for the possible triggering of OHS.
- The ultrasound image of the necklace sign: women with OHSS have a very characteristic ultrasound image, as the follicles are distributed around the ovary in a way that resembles the beads of a necklace.
- Possible previous episodes of OHSS: A previous OHSS may alert the doctor that this patient is susceptible to the treatment hormones. So she must change the hormone dose to avoid a new OHSS.

In case of gestation, hCG levels will increase. Therefore, OHSS will get worse and can put both the evolution of the pregnancy and the life of the pregnant woman at risk. Therefore, in case of suspicion that the syndrome may develop, implantation in the same cycle as the ovarian stimulation will be avoided.
How can OHSS be prevented?
There are several action protocols that can prevent the patient from having OHSS, or from making it worse. Depending on the tests and ultrasounds performed on the woman, the doctor may choose different alternatives. The choice of the procedure to avoid or reduce the symptoms of OHS will be assessed by the physician.
Considering undergoing a fertility treatment? By getting your individual Fertility Report your will see different clinics especially selected for you out of the pool of clinics that meet our strict quality criteria. Moreover, it will offer you a comparison between the fees and conditions each clinic offers in order for you to make a well informed choice.
Below we will explain in more detail some of the most commonly used strategies to avoid that OHSS will occurr.
Lower doses of gonadotropins
Patients who are given high doses of gonadotropins are more likely to develop OHSS because there is a greater ovarian response.
Therefore, in those women who have a high risk of developing OHSS because of their characteristics, such as being young, having PCOS or a very low body mass index, it will be advisable to start stimulation with low doses of gonadotropins and evaluate how they respond.

If you want to know more information about gonadotropins, we recommend you to continue reading this article: Gonadotropins: What are they and what are their functions?
Ovulation induction with GnRH agonists
One of the most efficient ways to avoid the appearance of OHSS is by substituting hCG with a drug that stops the maturation of the eggs in the woman, such as GnRH agonists.
The main advantage offered by this type of drug is that it prevents the syndrome while inducing ovulation. GnRH agonists trigger a hormonal reaction that aims to increase the LH hormone, the hormone that causes ovulation.
Most studies and reviews have shown that this measure reduces the risk of OHS, but decreases the rate of implantation and pregnancy because it causes a luteal phase deficit.
Cycle cancellation
Suspending the injection of hCG and cancelling the cycle is one of the strategies that effectively prevents the appearance of OHSS. In cases where follicular development is observed too rapidly or blood estradiol levels are excessively high, it might be considered to cancel the cycle.
However, the partner should be advised not to have sexual intercourse. This is because spontaneous ovulation can occur and lead in multiple pregnancy and/or late OHSS.
Embryo Cryopreservation
In cases where it is suspected that OHSS may develop, one of the options for not making the situation worse is to vitrify all the embryos for transfer in a subsequent cycle.
In doing so, OHSS won’t be prevented, but it hinders the aggravation that would result from pregnancy, since endogenous hCG would be produced.

Lowering the dose of hCG
Since there is a direct relationship between hCG levels and the severity of the syndrome, another approach to avoid the development of OHSS is to reduce the dose given to induce ovulation.
However, this measure does not completely eliminate the possibility of OHSS.
Treatment of ovarian hyperstimulation syndrome
The treatment indicated for each patient will depend on the severity of OHSS. In the mildest cases, no hospitalization will be necessary. However, in those cases where the patient's integrity is at risk, the patient should be admitted to a hospital:
Treatment of mild and moderate OHSS
To reduce the discomfort caused, it is recommended:
- Drink plenty of fluids, especially beverages rich in electrolytes (minerals)
- Rest with legs up to avoid thrombotic processes
- Avoiding alcohol and caffeine
- Avoiding intense exercise to prevent ovarian torsion
- Not having sex
- Taking pain medication to relieve pain

It will also be necessary to evaluate the evolution of OHSS in the woman to avoid complications.
Treatment in severe OHSS
In serious cases of OHSS, hospitalization of the patient will be necessary in order to thoroughly control her evolution. In addition, fluids will be given intravenously. In the most severe cases, a paracentesis, a surgical puncture to remove the accumulated fluid, may be necessary.
In serious cases of OHSS, it is extremely imporant to monitor:
- Liver functions
- Anticoagulant factors
- The hydroelectrolytic balance
- Kidney function
- Lung complications
Finally, you should consider those complications that may require surgery, such as rupture of a cyst that releases a large amount of blood, ovarian torsion, or ectopic pregnancy.
Video about ovarian hyperstimulation syndrome
In the following video, Michelle Emblenton, a biochemist at inviTRA, tells us all the details about ovarian hyperstimulation syndrome (OHSS):
Ovarian hypers stimulation syndrome or OHSS is something that can occur during an assisted reproduction treatment following ovarian stimulation. Specifically, OHSS is related to the hormone chorionic gonadotropin or HCG. This is used after ovarian stimulation to induce ovulation.
FAQs from users
Is sex recommended if I have suffered from ovarian hyperstimulation syndrome?
Ovarian hyperstimulation syndrome is a possible complication of in vitro fertilization that is triggered after administration of the chorionic gonadotropin hormone (hCG).
Ovarian hyperstimulation is characterized by an increase in the size of the ovaries. In the most severe cases there may be sudden changes in body fluids, with fluid leaking out of the blood vessels into, for example, the abdominal cavity.
In this type of situation, it is always recommended to avoid physical exercise and sexual relations. The main reason will be to avoid possible ovarian torsion. This consists of a complete or partial rotation of the ovary on its supporting elements, with the consequent loss of its blood supply. The fact that the ovary is larger than usual is a risk factor for this type of incident.
In fact, after carrying out an in vitro fertilization, even if there is no ovarian hyperstimulation syndrome, sexual relations are not recommended until some time has passed, as to a greater or lesser extent, the ovaries will always be larger than usual due to the growth of multiple follicles, and therefore, an increased risk of ovarian torsion.
Is it advisable to perform ovarian puncture with hyperstimulation?
It should be clarified that ovarian hyperstimulation syndrome occurs after ovulation, usually after the administration of HCG. For this reason, punctures are never performed in hyperstimulation, but rather at the risk of hyperstimulation.
When a patient is at risk of hyperstimulation, it is possible to perform different strategies:
- Lowering or stopping the administration of gonadotropins
- will decrease the ovarian quality, but the probability of hyperstimulation is reduced.
- Avoid administering HCG (Ovitrelle)
- reduces hyperstimulation to practically zero. It is the most widely used strategy today.
- Follicular punction
- reduces ovarian volume, the discomfort associated with hyperstimulation, and may reduce the number of active granulosa cells, thus helping to prevent the syndrome.

What risk do I have if I get pregnant with Ovarian Hyperstimulation Syndrome (OHSS)?
Ovarian hyperstimulation syndrome (OHSS) can occur in women who have been under hormonal treatment for assisted reproduction.
Usually, OHSS goes away within a few days after treatment, but if a woman becomes pregnant it can get worse and last longer, becoming severe OHSS.
However, OHSS is very rare nowadays, since if the patient is at risk of suffering it, it is decided not to transfer the embryos and frozen for later cycles where there is no risk.
Read more
How long do the symptoms of ovarian hyperstimulation syndrome (OHSS) last?
OHSS doesn't last long, as it usually disappears when the first menstruation begins after treatment with ovarian stimulation.
If pregnancy has occurred, the symptoms will last up to 70 days and may become more severe. Therefore, it will be necessary to carry out an exhaustive follow-up of the patient's evolution.
How long do I have to wait for the embryo transfer after ovarian hyperstimulation?
It is necessary to wait at least until the first menstruation after the OHSS, that is, until the next cycle.
After that, it will be the specialists who will have to assess the situation and, depending on the endometrial preparation protocol chosen and the patient's condition, decide when it is advisable to perform the thawing and transfer of the vitrified embryos.
Does lowering hCG doses prevent OHSS?
Since there is a direct relationship between hCG levels and the severity of OHSS, one might think that reducing hCG levels would be a solution to prevent the syndrome. However, it should be stressed that this measure does not completely eliminate the possibility of OHSS in a woman.
Suggested for you
As we have seen, OHSS can have different degrees of severity and symptoms. If you want to know more about the course of this alteration, we recommend that you read: Natural evolution of the ovarian hyperstimulation syndrom (OHSS).
On the other hand, one of the strategies we have explained that exist to avoid aggravating the symptoms of OHSS is to vitrify all the embryos for transfer in subsequent cycles. In this article we tell you how the transfer will be done in this case: How does the frozen embryo transfer procedure work?
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Adrija Kumar Datta, Abha Maheshwari, Nirmal Felix, Stuart Campbell, Geeta Nargund. Mild versus conventional ovarian stimulation for IVF in poor, normal and hyper-responders: a systematic review and meta-analysis. Hum Reprod Update. 2021 Feb 19;27(2):229-253 (View)
Bo Sun, Yujia Ma, Lu Li, Linli Hu, Fang Wang, Yile Zhang, Shanjun Dai, Yingpu Sun. Factors Associated with Ovarian Hyperstimulation Syndrome (OHSS) Severity in Women With Polycystic Ovary Syndrome Undergoing IVF/ICSI. Front Endocrinol (Lausanne). 2021 Jan 19:11:615957. doi: 10.3389/fendo.2020.615957 (View)
Cerillo Martínez M, Pellicer Martínez A. (2010). Síndrome de hiperestimulación ovárica. En Garcia Velasco JA, Callejo Olmos J Estimulación ovárica en técnicas de reproducción asistida (pp.67-81). Barcelona. Editorial Glosa, S.L
Douglas Timmons, Tim Montrief, Alex Koyfman 3, Brit Long. Ovarian hyperstimulation syndrome: A review for emergency clinicians. Am J Emerg Med. 2019 Aug;37(8):1577-1584. doi: 10.1016/j.ajem.2019.05.018 (View)
Practice Committee of the American Society for Reproductive Medicine, Practice Committee of the American Society for Reproductive Medicine. Prevention treatment of moderate and severe ovarian hyperstimulation syndrome: a guideline. Fertil Steril. 2016 Dec;106(7):1634-1647. doi: 10.1016/j.fertnstert.2016.08.048. Epub 2016 Sep 24.
Scott M Nelson. Prevention and management of ovarian hyperstimulation syndrome. Thromb Res. 2017 Mar:151 Suppl 1:S61-S64. doi: 10.1016/S0049-3848(17)30070-1 (View)
FAQs from users: 'Is sex recommended if I have suffered from ovarian hyperstimulation syndrome?', 'Is it advisable to perform ovarian puncture with hyperstimulation?', 'What risk do I have if I get pregnant with Ovarian Hyperstimulation Syndrome (OHSS)?', 'How long do the symptoms of ovarian hyperstimulation syndrome (OHSS) last?', 'When does ovarian hyperstimulation syndrome (OHSS) occur?', 'How long do I have to wait for the embryo transfer after ovarian hyperstimulation?', 'How can ovarian hyperstimulation syndrome (OHSS) be prevented?', 'What are the different degrees of ovarian hyperstimulation syndrome (OHSS)?', 'How is ovarian hyperstimulation syndrome (OHSS) treated?', 'I am under 30, am I at risk of ovarian hyperstimulation syndrome (OHSS)?', 'Can I do sports with mild ovarian hyperstimulation syndrome (OHSS)?' and 'Does lowering hCG doses prevent OHSS?'.
Authors and contributors









More information about Michelle Lorraine Embleton
