What is the procedure for pre-implantation genetic diagnosis?
Pre-implantation genetic diagnosis (PGD) is a genetic analysis of embryos obtained from in vitro fertilization (IVF) with the aim of selecting healthy embryos with the capacity for implantation.
Furthermore, PGD is the most indicated technique to avoid the transmission of a hereditary genetic disease, since it allows the detection of embryos with mutations in their DNA, which will be discarded for their transfer to the uterus.
PGD must be performed by experts in both embryology and genetics, as it requires very delicate techniques such as blastomere biopsy and molecular genetics techniques.
The different sections of this article have been assembled into the following table of contents.
Contents
- 1.
- 2.
- 2.1.
- 2.2.
- 3.
- 3.1.
- 3.2.
- 4.
- 4.1.
- 4.2.
- 5.
- 6.
- 6.1.
- 6.2.
- 6.3.
- 6.4.
- 6.5.
- 6.6.
- 6.7.
- 7.
- 8.
PGD step by step
IVF with PGD is one of the most laborious treatments in assisted reproduction and therefore has several steps from ovarian stimulation to embryo transfer. Below, we will discuss each of them:
- IVF
- consists of performing ovarian stimulation on the woman, obtaining the eggs by means of follicular puncture and, finally, fertilizing the eggs with the sperm of the male partner or of an anonymous donor.
- Embryonic development
- the characteristics of the embryos in culture are assessed on a daily basis, since in order to perform the biopsy it is necessary for them to have a minimum level of quality to ensure their survival.
- Cellular biopsy
- extraction of one or more blastomeres (cells from the embryo) for subsequent genetic analysis. It can be performed on day 3 embryos or once they have reached the blastocyst stage on day 5. The removed cell is then carefully placed in a tube, a process known as tubing.
- Genetic analysis
- study of the chromosomes and/or genes in the biopsied cells to identify possible alterations in them. Specifically, chromosome analysis is better known as preimplantation genetic screening and, on the other hand, the term PGD is used for the analysis of specific genetic mutations.
- Embryo transfer
- genetically healthy embryos are selected for transfer to the mother's uterus or cryopreservation for future attempts.


It should be noted that the transfer of embryos can be done in a fresh or frozen cycle. This will depend on the time needed to obtain the results of the genetic analysis, and it is quite common for the embryos to have to be frozen.
Embryo biopsy
Embryo biopsy is the process of extracting one or more cells, called blastomeres, in order to analyze the embryos' DNA for any genetic alteration.
The viability of the embryo may be compromised by this biopsy, since the loss of a cell may be too stressful for the embryo to survive. Therefore, it is necessary that this cell extraction be performed by highly specialized and experienced laboratory personnel.
If you need to undergo IVF to become a mother, we recommend that you generate your Fertility Report now. In 3 simple steps, it will show you a list of clinics that fit your preferences and meet our strict quality criteria. Moreover, you will receive a report via email with useful tips to visit a fertility clinic for the first time.
The embryo biopsy can be done on day 3 or day 5. In both cases, it is essential that fertilization takes place through ICSI. In conventional IVF, there are sperm and granulosa cells attached to the zona pellucida of the embryo. This poses a risk of contamination of the extracted blastomeres and therefore the PGD could give an altered result.
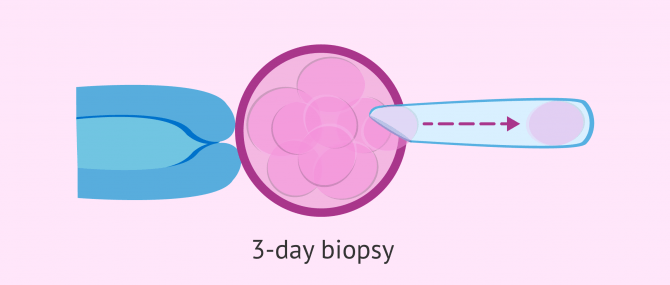
Blastomere biopsy on day 3
On the third day of embryonic development, good quality embryos usually have 8 cells, although they may also have between 6 and 10 cells depending on their rate of division.
Therefore, if the biopsy is done at this precise moment, only one, or at most two, blastomeres will be removed from the embryo in order not to compromise its viability.
During the procedure, a hole is made in the zona pellucida of the embryo by means of laser pulses or chemical agents, such as Tyrodes acid. Once this hole has been made, the blastomere is removed by suction.
After the embryo biopsy, there are two possible options for the embryos:
- Blastocyst culture
- the embryos are left in culture to continue their evolution while waiting for the results of the genetic analysis. Therefore, the embryo transfer will be in the blastocyst stage on day 5.
- Embryo vitrification
- the embryos are frozen after the biopsy for transfer in a later cycle.
If you are interested in reading more about this topic, you can access the following post: Frozen Embryo Transfer Procedure.
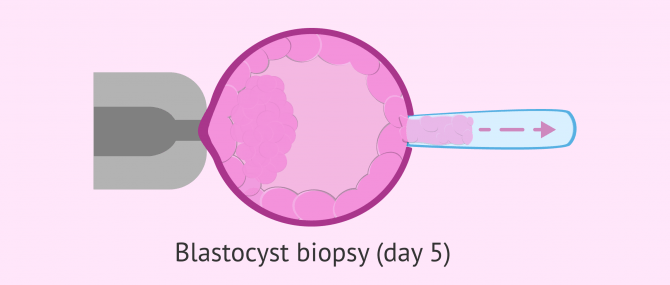
Trophoectoderm biopsy on day 5
By the fifth day of development, the embryo has become what is known as a blastocyst. This is a larger embryo, composed of a multitude of cells and with 3 differentiated parts:
- Internal cellular mass (ICM)
- gives rise to the future fetus.
- Blastocele
- is an internal cavity filled with fluid.
- Trophoectoderm
- outer layer that originates the placenta and other extra-embryonic structures.

Although these are different cell populations, both ICM and trophectoderm cells have the same genetic material. It is, therefore, possible to extract a few cells from this outer layer for analysis with PGD.
The fact that several cells can be extracted from the embryo is an advantage since a more reliable result will be obtained, it will be possible to detect cases of mosaicism and, furthermore, the viability of the embryo will not be so compromised.
When doing the biopsy with a blastocyst, care should be taken to make the hole in a place away from the ICM in order to avoid possible damage.
On the other hand, it is more convenient to use the short pulses of the laser to pierce the zona pellucida than Tyrodes acid since it has greatly reduced its thickness as the blastocyst expands and the use of a chemical agent could damage it.
Then, once a sufficient hole has been made to insert the biopsy pipette, the cells are removed by aspiration. To separate the cells to be removed from those that remain inside the embryo, the laser pulses can help.
In this case, it will be necessary to vitrify the embryos after the biopsy in order to transfer them in a future cycle, since the results of the genetic analysis take several days and it would not be viable to leave the embryos in culture.
Pre-implantation genetic screening
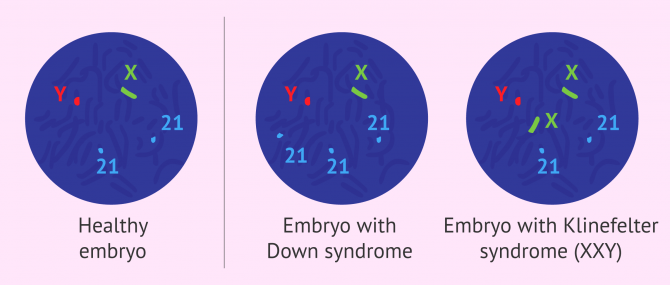
Pre-implantation genetic screening is a type of PGD in which possible aneuploidies in embryos are analyzed. < strong>Aneuploidies are alterations in the number or structure of chromosomes, taking into account that the normal human chromosome endowment is 46 chromosomes. Therefore, the gain or loss of a chromosome, as well as changes in its structure, are abnormalities that can result in non-viable embryos or newborns with chromosome diseases such as Down syndrome.
In some clinics, this type of PGD is also called aneuploidy screeningand the genetic tests used for their detection are those discussed in the following sections.
FISH Study
Fluorescent in-situ hybridization (FISH) is the technique that has traditionally been used in the study of chromosomal abnormalities.
It only allows the analysis of certain regions of 9 chromosomes (13, 15, 16, 17, 18, 21, 22, X and Y). However, these chromosomes are involved in aneuploidies that can lead to repeated miscarriages or the birth of sick children.
The process consists of adding fluorescent probes for specific regions of the chromosomes to be analyzed. It is then possible to visualize the fluorescent signal through a special microscope and to detect whether any of the analyzed regions are missing or, on the contrary, if there are more copies than they should be.
Since the analysis of only a certain number of chromosomes is a limitation, FISH is considered an incomplete analysis and is currently being replaced by other techniques that allow a complete genetic analysis of the embryo.
CGH Arrays
The Comparative Genomic Hybridization Array (A-CGH) is a technique that allows us to carry out a Comprehensive Chromosome Screening (CCS), that is, the 23 pairs of chromosomes are analyzed at the same time in search of regions with some chromosomal alteration.
To carry out this genetic analysis, a control DNA and the DNA sample to be studied from the extracted embryonic cell are used. Both DNA strands are marked with different fluorescent probes and then hybridized in the microarray.
With this methodology, it is possible to compare the DNA of the embryo with that of the reference sample and identify losses (deletions) or gains (duplications) of genetic material, which could lead to embryonic defects.

Although this technique is much more decisive than FISH, it only makes quantitative comparisons, that is, it detects whether there is missing or excess genetic material. Therefore, it does not detect if there are chromosome fragments that are not in the right place, such as inversions or translocations.
PGD for monogenic diseases
Monogenic diseases are those caused by mutations in a single gene, such as cystic fibrosis, hemophilia, or fragile X syndrome.

In addition, they are hereditary diseases that are transmitted from parents to children. Therefore, before doing PGD on the embryos, it is necessary to identify the specific mutation in the parents through an informativity study.
Once the mutation has been located and the type of inheritance determined (dominant, recessive or sex-linked), it is possible to study the embryos with the genetic tools discussed below.
PCR
The polymerase chain reaction (PCR) involves the amplification of specific DNA sequences for further analysis. Thus, it is possible to obtain millions of copies of the gene of interest from a single copy present in the extracted cell.
Once the desired sequence has been amplified, different molecular biology techniques are used to analyze it and locate the possible mutations that give rise to monogenic diseases.
Mass sequencing
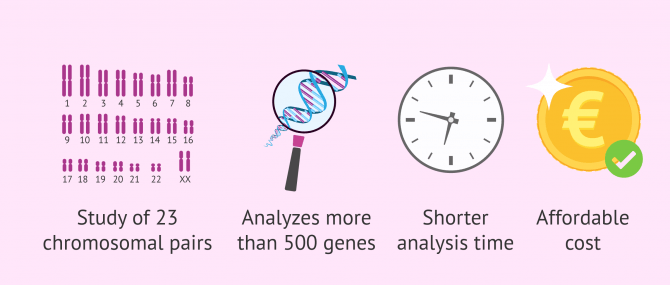
Next-generation sequencing (NGS) is the most advanced technique for genetic studies today.
The advantages it offers over other techniques are as follows:
- It allows the study of all 23 pairs of chromosomes in the same analysis, and with a higher resolution.
- It allows the simultaneous analysis of more than 500 genes associated with hereditary diseases.
- It is possible to study aneuploidies and monogenic diseases separately or simultaneously in a single analysis.
- Reduced analysis time, avoiding the need to freeze the embryos while waiting for the results.
- It allows a high number of samples to be analyzed at the same time, making the cost of analysis more affordable.
Nowadays, more and more clinics are opting for this latest technology both for aneuploidy screening and for the detection of monogenic diseases.
Transfer of healthy embryos
Once the results are obtained, the healthy embryos will be transferred to the mother's uterus or vitrified for future attempts. Embryos with genetic alterations are discarded, even if they apparently have good morphological quality.
If the embryos have been vitrified prior to the results, they will be transferred in a replacement cycle. To do this, the woman will have to make an endometrial preparation with the administration of estrogen and progesterone.

If the results show that there are several embryos free of abnormalities, only the embryo or embryos with the best morphogenetic quality for transfer will be thawed, which will increase the probability of implantation.
FAQs from users
In what kind of cases is PGD being used?
PGD facilitates informed decision making and is increasingly being included as an option in genetic counselling.
The current objective is that it can reach any couple, if they so freely choose, and any hereditary pathology, as long as there is a clinical indication and it is possible to address its diagnosis technically.
For couples with a clinical history of monogenic disease, the main current indications are, among others, cystic fibrosis, spinal muscular atrophy, myotonic dystrophy (Steinert), fragile X syndrome and Huntington's disease.

Regarding chromosomal analysis, the main indication is the embryo study due to the risk of aneuploidy in advanced maternal age, without forgetting the group of patients with a history of recurrent miscarriage and severe male factor.
What is the probability that there will be no embryos left after the PGT?
The probability of having no embryos suitable for transfer depends on several factors such as age, ovarian reserve, DNA fragmentation:
- Decreased Ovarian Reserve: in these patientes fewer oocytes are retrieved. Ovarian reserve and ovarian response are inversely related to maternal age; as maternal age increases, both ovarian reserve and response decrease. Consequently, advanced maternal age affects the number of oocytes retrieved, their quality, and the number of embryos available for biopsy.
- Reduced Embryo Yield: a lower starting number of oocytes translates to fewer embryos reaching the blastocyst stage suitable for biopsy. Is important to understand that biopsy for PGT can only be performed on blastocysts; if embryos arrest earlier, they cannot be analyzed.
- Increased Aneuploidy: oocytes from patients with advanced maternal age have a higher risk of chromosomal abnormalities (aneuploidy), further reducing the percentage of "healthy" embryos available for transfer.


Another factor to consider is the quality of the sperm:
- Male factor: high sperm DNA fragmentation can negatively affect the genetic quality of embryos.
If you (or your partner) are a carrier of a structural rearrangement or a monogenic disease, the risk of not having embryos available after PGT will also depend on the probability, in each individual case, of having embryos free of the mutation, and on whether you choose to have them analysed for aneuploidies as well.
In summary, the greater the number of embryos available for PGT, the higher the chances of obtaining healthy embryos suitable for transfer to the uterus.
Are PGD and PGT the same?
These are the acronyms for the genetic studies that are performed on an embryo before it is transferred to the uterus. On the one hand, PGD refers to preimplantation genetic diagnosis; while PGT stands for Preimplantation Genetic Test.
Currently, the most commonly used term for this complementary technique is PGT.
What are the advantages of doing a PGD?
When PGT (formerly known as PGD) is not performed, embryo selection is based on morphological or morphokinetic parameters (if the embryo has been incubated in a time-lapse system).
PGT has the advantage of allowing the embryo to be transferred to the uterus to be selected based on the results of the genetic analysis performed. By transferring only embryos with a favorable result, embryos with genetic abnormalities that could lead to miscarriage or the birth of a baby with a disease are avoided.

Can extracting one or more cells from the embryo negatively affect its further development?
Yes, the process can compromise the viability of the embryo, since losing some cells can be too stressful for it to survive. Even so, the survival rate is very high, especially when the PGD is done in blastocysts, since these embryos have a greater number of cells than those on day 3 and, therefore, are able to recover more easily after the biopsy.
Is PGD better on day 3 or day 5?
It is now much more common to perform embryo biopsy for preimplantation genetic testing (PGT, formerly known as PGD) on day 5 of embryo development, as the embryo at the blastocyst stage (day 5) has a greater number of cells than on day 3 and, therefore, a small number of cells can be extracted from the trophectoderm (the part of the embryo that will give rise to the placenta).
Is it possible to perform a polar corpuscle biopsy?
Yes, it would be possible to perform a biopsy of the first polar body of the egg for the purpose of genetic analysis. In this case, it would be a preconception genetic study (before the egg is fertilized by the sperm). Therefore, this study of the polar body could provide information on the genetic status of the egg, but it cannot assess whether the future embryo (once fertilization has occurred) will have any genetic abnormalities of paternal origin.
For all these reasons, this technique is not at all common, since it is more common to perform preimplantation genetic testing (PGT) on embryos, performing the biopsy when they are in the blastocyst stage.
Suggested for you
Throughout this article, we have commented that PGD serves to detect genetic and chromosomal abnormalities in embryos. If you want to know what specific diseases occur as a result of these alterations, you can read on here: What genetic or chromosomal diseases can PGD detect?
For information on the success rates of this technique, we encourage you to enter the following article: Pregnancy probability with PGD.
We make a great effort to provide you with the highest quality information.
🙏 Please share this article if you liked it. 💜💜 You help us continue!
References
Anthony Homer H. Preimplantation genetic testing for aneuploidy (PGT-A): The biology, the technology and the clinical outcomes. Aust N Z J Obstet Gynaecol. 2019 Apr;59(2):317-324. doi: 10.1111/ajo.12960. Epub 2019 Feb 27 (View)
Rajesh Parikh F, Sitaram Athalye A, Jagannath Naik N, Jayaram Naik D, Ramesh Sanap R, Fali Madon P. Preimplantation Genetic Testing: Its Evolution, Where Are We Today?J Hum Reprod Sci . Oct-Dec 2018;11(4):306-314. doi: 10.4103/jhrs.JHRS_132_18 (View)
Sciorio R, Anderson R. Fertility preservation and preimplantation genetic assessment for women with breast cancer.Cryobiology. 2020 Feb 1;92:1-8. doi: 10.1016/j.cryobiol.2019.12.001. Epub 2019 Dec 18.
Wilding M, Terribile M, Parisi I, Nargund G. Thaw, biopsy and refreeze strategy for PGT-A on previously cryopreserved embryos. Facts Views Vis Obgyn. 2019 Sep;11(3):223-227 (View)