The preimplantation genetic test (PGT), formerly known as preimplantation genetic diagnosis (PGD), is a genetic analysis performed on embryos during in vitro fertilization (IVF) treatment.
Its objective is to discard embryos with alterations in their DNA in order to transfer only those that are genetically viable. This allows you to increase the chance of pregnancy and having a healthy baby.
The latest statistics published by the Spanish Fertility Society (SEF) show that the probability of obtaining a positive result in an IVF cycle is greater when embryos are genetically selected (National Registry of Activity 2022-SEF Registry).
Provided below is an index with the 8 points we are going to expand on in this article.
- 1.
- 1.1.
- 2.
- 2.1.
- 2.2.
- 3.
- 4.
- 4.1.
- 4.2.
- 4.3.
- 4.4.
- 4.5.
- 4.6.
- 5.
- 6.
- 7.
- 8.
Results of PGT
Once the embryonic biopsy has been performed and one or more cells have been sent for analysis, the results of the PGT may take several days depending on the laboratory where it is performed.
During this time, the embryos may remain in culture until they develop to the blastocyst stage or be frozen pending diagnosis.
After obtaining the PGT result report, the embryologist may encounter the following situations:
- Healthy embryo
- both the number and structure of the embryo's chromosomes are normal. This embryo can be transferred.
- Sick embryo
- the embryo has some aneuploidy or genetic mutation. This embryo cannot be transferred.
- Mosaic Embryo
- the embryo has some healthy cells and some sick cells. Depending on the degree of mosaicism and the number of healthy embryos available, the doctor will assess whether to transfer this embryo or not.
- Non-informative embryo
- there was a failure in the genetic analysis and the embryo could not be tested. You don't know if he's healthy or sick. The doctor will have to assess whether to transfer this embryo or not depending on the number of healthy embryos available.

The percentage of healthy embryos after PGT will depend on the specific genetic alteration and the type of inheritance in case of a hereditary disease.
Depending on the number of healthy or possibly viable embryos (mosaic and non-informative), the decision will be made to how many embryos to transfer to achieve pregnancy. If there are more healthy embryos left over, they will be vitrified for future attempts.
Involved factors
The probability of obtaining a positive IVF-PGT cycle, i.e. a positive genetic test result and a viable pregnancy after the embryo transfer, will depend on the following factors:
- Experience of the embryologist to perform the embryo biopsy.
- Number of cells analyzed. With blastocyst biopsy, a greater number of cells are obtained for analysis and the reliability of the result is greater.
- Technique used to analyze the genetic material of the biopsied cells. Mass sequencing is the most reliable technique today.
- Quality of tested embryos. Better quality embryos have a higher survival rate.
- Ability of the embryos to recover from the biopsy. Embryos in the blastocyst stage have a greater capacity for recovery because they have a greater number of cells.
- Transfer of fresh or vitrified embryos.

In the case of hereditary genetic diseases, the probability of obtaining genetically healthy embryos will depend on the type of inheritance: dominant or recessive.
Finally, as in all other assisted reproduction techniques, the most important factor that will determine the success of the treatment is the age of the woman. Younger women are more likely to obtain genetically normal embryos.
Statistics of PGT
PGT is a complementary technique that is being used more and more routinely in all IVF laboratories.
In 2022, 20,502 IVF cycles were initiated for PGT in Spain, 2,674 more than in 2020.
Indications
Not all couples undergoing in vitro fertilization use PGT. The increase in pregnancy and delivery rates is most evident in those couples with an indication.
In 2022, the main causes of indication of IVF with PGT were from more to less:
- Advanced maternal age (59.2%)
- Molecular diseases (7.3%)
- Implantation failures (6.0%)
- Recurrent miscarriage (5.3%)
- Cytogenetic diseases (4.2%)
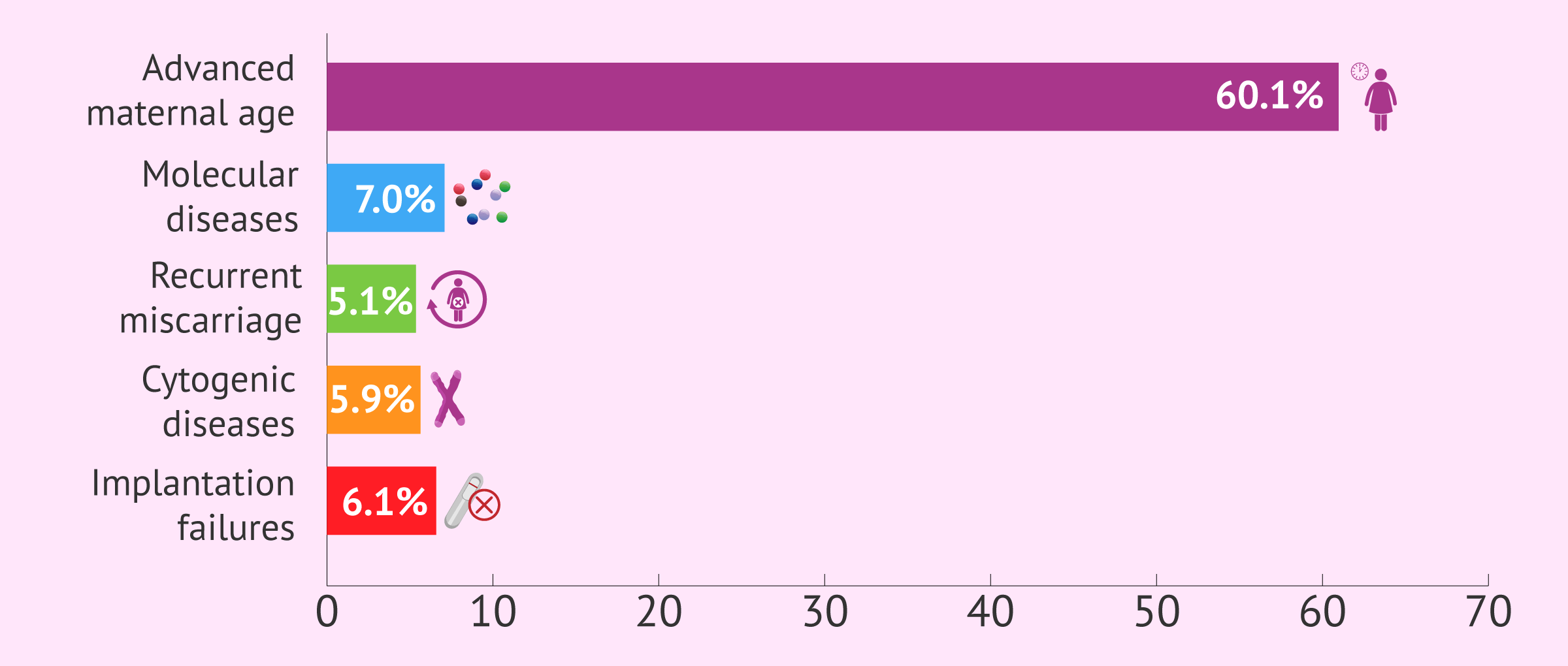
Therefore, 52,0% of the IVF cycles with PGT performed, more than half, were due to advanced maternal age and the presence of chromosomal abnormalities. The remaining percentage is due to other causes.
PGT success rates
There are many ways to represent the success rates of fertility treatments.
Below, we will explain what we consider to be the most important ones based on the latest results of the SEF 2022:
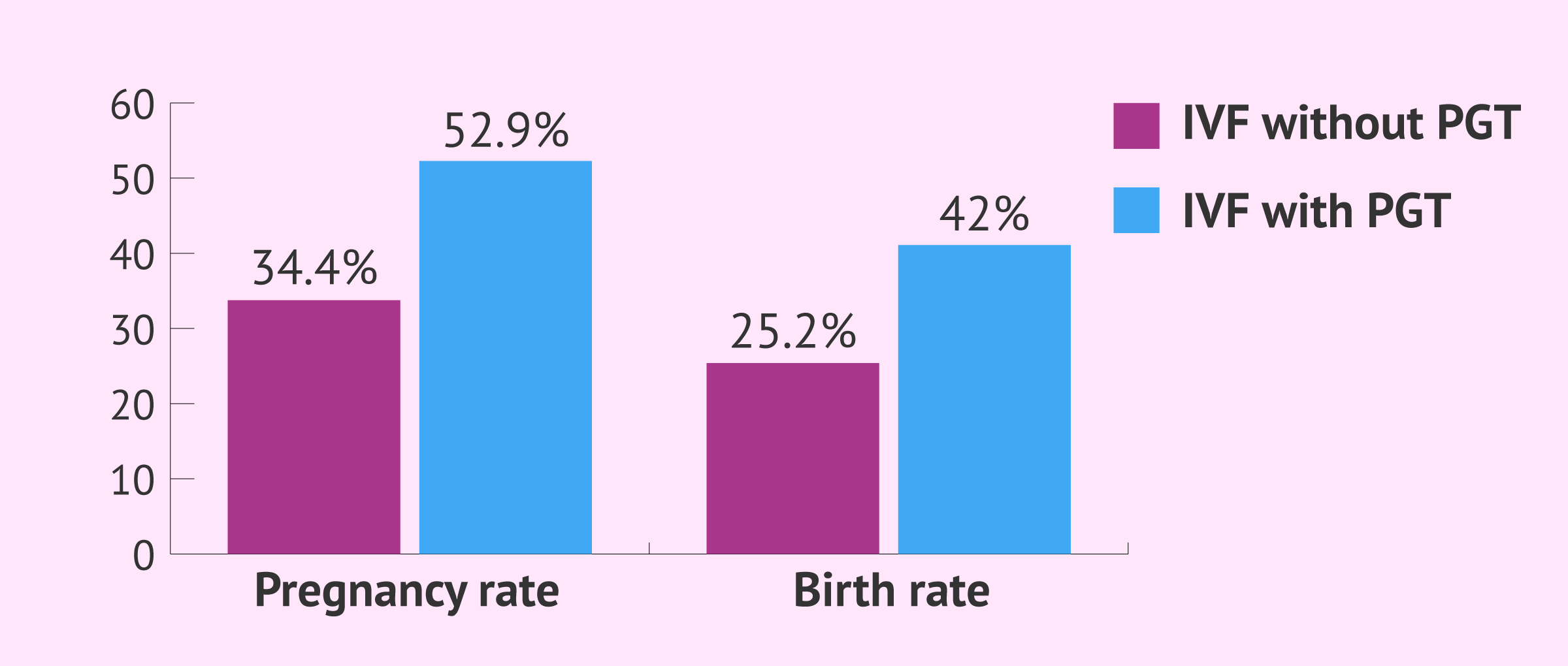
- Pregnancy rate
- 52.0% (pregnancies by embryo transfer)
- Birth rate
- 40.6% (pregnancies by embryo transfer)
- Single birth rate
- 97.3% (single births by number of total births)
- Twin birth rate
- 2.7% (twin births by number of total births)
- Miscarriage rate
- 17.2% (miscarriages by number of pregnancies)
These success rates are higher than those obtained for IVF cycles with own eggs without PGT, which have a pregnancy rate of 34.6% and a delivery rate of 25.0% per transfer.
Finally, it is important to bear in mind that obtaining healthy embryos in the PGT does not guarantee 100% that they will implant and give rise to a gestation, since other factors come into play here, such as the thickness of the endometrium, the rate of embryo division, etc.
Advantages and disadvantages of PGT
Although the most successful assisted reproduction treatment available today in egg donation, genetic analysis of embryos has managed to significantly increase the pregnancy rate per transfer.
This has given women of advanced maternal age the opportunity to become pregnant with their own eggs.
In addition, IVF with PGT has made it possible to reduce the number of embryo transfers destined to failure, which is both a psychological and economic advantage. The downside of all this, however, is that it also increases the number of canceled cycles. Approximately one-third of women who undergo IVF with PGT does not get to transfer any embryos due to aneuploid embryo collection.
Dr. Gorka Barrenetxea says:
The stricter the embryo selection, the more likely it is that we will run out of embryos for transfer.
Let's say we have five blastocysts from a 38-year-old woman. Let's say we do a genetic selection and all five embryos are abnormal. Obviously, the day we break that news is bad news. We have five morphologically perfect blastocysts but they are aneuploid, condemned to non-pregnancy or abortion. Being bad news, it is also good news, since we have just saved 5 transfers, from the administrative and psychological point of view.
FAQs from users
How many embryos are transferred after PGD?
The number of embryos to be transferred to a patient does not depend on the technique that has been practiced on the embryo, but on the day it is found, its quality and the intrinsic characteristics of each patient. The performance of a Preimplantation Genetic Diagnosis is associated in most cases with advanced maternal age (screening of aneuploidies) or the presence of serious genetic pathologies (in many cases present in the woman). In both cases, multiple pregnancy is contraindicated.
For all these circumstances, the medical advice is usually the transfer of a single embryo.
What are the alternatives to using PGD?
The main alternative to the use of PGD is prenatal diagnosis, which, in order to have a truly preventive effect, is necessarily linked to the decision to abort affected fetuses.
Another option involves changing the gametes (egg or sperm) of one or both members of the couple at genetic risk.
Finally, and although today it is no longer necessary in the vast majority of cases, avoiding having children would be a third alternative.
How many eggs must be obtained for the PGD cycle to be successful?
For there to be a reasonable probability of success in the IVF cycle with PGD, it is important to recover a good number of eggs in the follicular puncture. Generally, obtaining 6 or more eggs would be best. On the other hand, if the woman is a low responder, there is little chance that IVF with PGD will be successful.
There is also the option of making cycles of egg accumulation to obtain several embryos from several cycles and to be able to analyze them all together. In this way, the probability of success is increased and the cost of treatment is reduced.
How long does it take to get the results of PGD?
From the time the embryonic biopsy is performed and the cells are sent for analysis, it usually takes about 48 hours until the result is received and the woman or couple is notified.
However, this depends on the clinic and the laboratory making the diagnosis. On occasion, the results may take a week, so it will be necessary to vitrify the embryos in order to transfer them in a next cycle.
What can we do if there is no healthy embryo in the PGD?
There are two options: to repeat a new IVF cycle with PGD or to use egg or sperm donation. The choice will depend on whether any other failed IVF-PGS cycle has already been performed and on the recommendation of the specialists of the reproductive center for the particular case.
Can PGD results be wrong?
Like the vast majority of testing techniques, PGD also has a small error rate, which could lead to false positives and negatives.
This depends mainly on the technique used for the genetic analysis. For example, the FISH technique only allows a maximum of 12 chromosomes to be analyzed, whereas with the latest massive sequencing techniques all chromosomes can be analyzed and a reliability of 96-98% is obtained.
However, it is also necessary to take into account the possible mosaicism (two different types of cell lines) caused by a very early error in embryonic development. Nowadays, thanks to the biopsy of several cells in the blastocyst, it is possible to detect this mosaicism and decrease the probability of PGD error.
Recommended reading
If you aren't sure about how IVF procedure with PGT works, you can find a more detailed explanation in the following post: What is preimplantation genetic diagnosis or PGD?
For more information on the probability of getting pregnant through fertility treatments, you can read on here: An analysis of success rates in assisted reproduction treatments
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Collins SC. Preimplantation genetic diagnosis: technical advances and expanding applications. Curr Opin Obstet Gynecol. 2013;25(3):201-6.
Lee E, Illingworth P, Wilton L, Chambers GM. The clinical effectiveness of preimplantation genetic diagnosis for aneuploidy in all 24 chromosomes (PGD-A): systematic review. Hum Reprod. 2015;30(2):473-83 (View)
Platteau P, Staessen C, Michiels A, Van Steirteghem A, Liebaers I, Devroey P. Preimplantation genetic diagnosis for aneuploidy screening in women older than 37 years. Fertil Steril. 2005;84(2):319-24 (View)
Rubio C, Bellver J, Rodrigo L, Castillón G, Guillén A, Vidal C, Giles J, Ferrando M, Cabanillas S, Remohí J, Pellicer A, Simón C. In vitro fertilization with preimplantation genetic diagnosis for aneuploidies in advanced maternal age: a randomized, controlled study. Fertil Steril. 2017;107(5):1122-1129 (View)
Sociedad Española de Fertilidad. Registro Nacional de Actividad 2022-Registro SEF (View)
FAQs from users: 'How many embryos are transferred after PGD?', 'What are the alternatives to using PGD?', 'How many eggs must be obtained for the PGD cycle to be successful?', 'How long does it take to get the results of PGD?', 'What can we do if there is no healthy embryo in the PGD?' and 'Can PGD results be wrong?'.
Authors and contributors







More information about Michelle Lorraine Embleton


I don’t understand how some clinics can take 2 days to give you the results and others weeks? I had to have all my embryos frozen after thebiopsy and it took them almost 2 weeks to call me back. How can this be?
Hi Lola-jola
In reality, it depends on the clinics themselves and the laboratories where the analysis is performed. In most centers, the biopsied cells have to be sent to external laboratories for analysis, as very complex equipment is needed to perform this.
As a consequence, the results of the analysis may take more than 48 hours and it is common for PGD results to take more than a week.
I hope this helps
Best wishes