Artificial insemination (AI), also known as intrauterine insemination (IUI), is one of the simplest assisted reproduction treatments, so its success rates are not particularly high, especially in the first attempt.
Even so, all women and couples who meet the requirements for artificial insemination have a chance of achieving pregnancy.
In addition, the success rate of AI increases after the first attempt, so that the woman could become pregnant in the second, third, or fourth cycle. This is known as the cumulative success rate.
Provided below is an index with the 9 points we are going to expand on in this article.
- 1.
- 1.1.
- 1.2.
- 2.
- 2.1.
- 2.2.
- 3.
- 4.
- 5.
- 5.1.
- 5.2.
- 5.3.
- 5.4.
- 5.5.
- 5.6.
- 5.7.
- 5.8.
- 5.9.
- 6.
- 7.
- 8.
- 9.
Does artificial insemination work?
The AI treatment is designed to help the natural process of conception since it consists of simply depositing the sperm from the man in the woman's uterus. Nevertheless, the sperm themselves are the ones that have to travel through the Fallopian tubes to reach the egg and fertilize it.
As such, intrauterine insemination is only recommended in mild cases of infertility, when the woman is young and her ovarian reserve is not yet compromised.
Thanks to artificial insemination, 5,565 babies were born in Spain in 2021, with respect to the 3,904 babies born in 2020, according to the latest data published by the Spanish Fertility Society (SEF).
IUI is also usually the first technique indicated when the couple comes to a fertility clinic, whenever it is possible and when there is a chance of success, as it is the simplest and most economical treatment.
Basic requirements
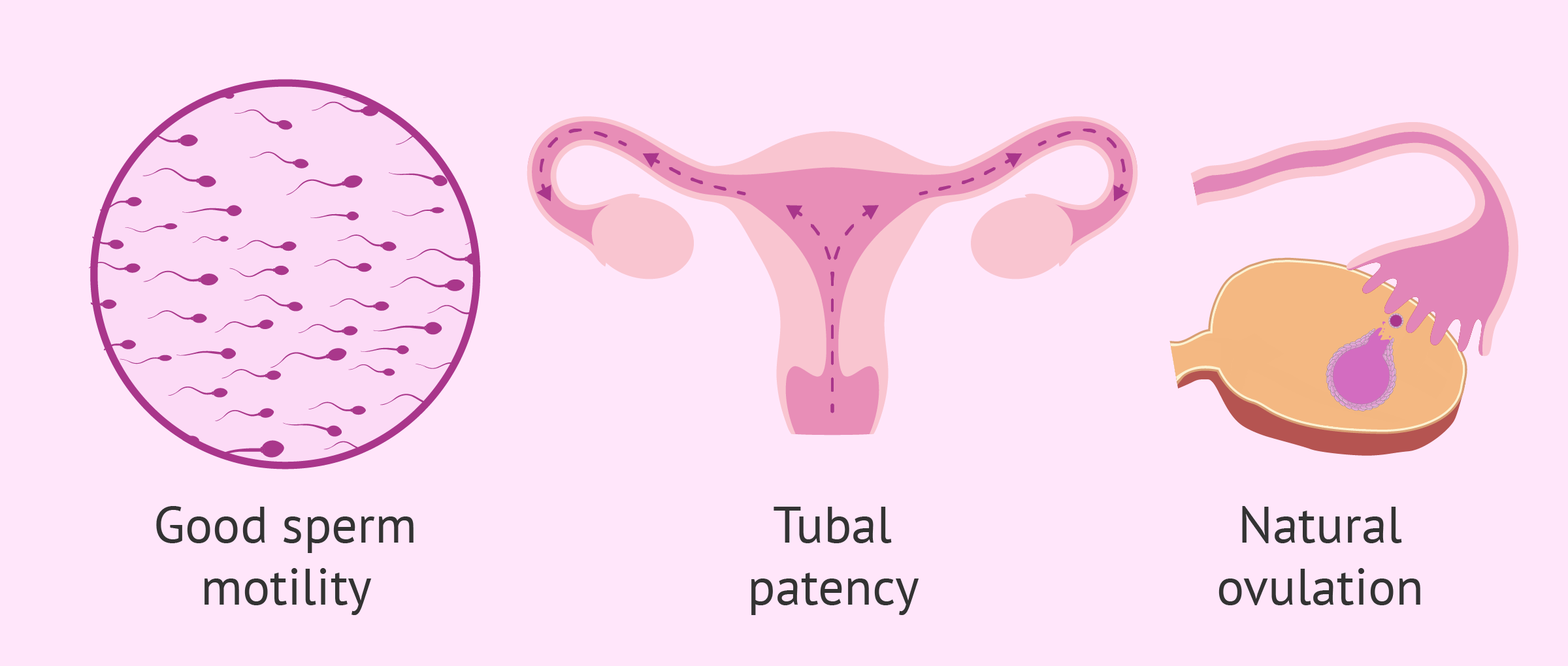
In order to carry out artificial insemination, it is necessary for both the woman and the man to undergo some fertility tests to ensure that they meet the following requirements:
- Good seminal quality. The male has a good amount of motile spermatozoa.
- The woman must be able to ovulate, either spontaneously or induced with hormonal medication.
- The Fallopian tubes must be patent.
If these 3 basic requirements are met, artificial insemination can be the definitive solution to the reproductive problem.
For more detailed information about this, you can continue reading here: Basic requirements for intrauterine artificial insemination.
AI success factors
Despite everything that has been said so far, not all people who meet the AI requirements will be able to get pregnant with this fertility treatment.
The success of artificial insemination depends on many other factors related to the couple or the treatment. We comment on them below:
- Age of the woman
- a woman's reproductive capacity decreases over time until its definitive end in what we know as menopause. As we approach this period, the quantity and quality of the eggs are reduced. That is why, from the age of 35-37, the chances of pregnancy through artificial insemination are low.
- Cause of infertility
- for AI to be successful, the sperm must have sufficient capacity to travel through the female reproductive tract, swim to the egg and penetrate it for fertilization to occur. Therefore, if there are serious fertility problems in women or men, such as severe endometriosis or oligoasthenozoospermia, it will be difficult for natural fertilization to take place.
- Origin of the male gamete
- since donor sperm is of very high quality, women who undergo donor artificial insemination (DAI) will have a higher chance of achieving pregnancy.

- Ovarian stimulation protocol
- It is important to analyze the situation of each woman and personalize the hormonal treatment that she will receive to stimulate ovarian development and ovulation. A very strong stimulation can cause too many follicles to mature, which can be counterproductive since the quality of the ovules could be affected, as well as increasing the probability of a multiple pregnancy.
- Endometrial receptivity
- The endometrium is the layer of the uterus where the implantation of the embryo and the beginning of pregnancy take place. For this to happen, the endometrium must be receptive, that is, in good condition to receive the embryo. It is essential that the endometrium has a trilaminar appearance (three parallel layers are seen on ultrasound) and an approximate thickness of 8-10 mm. If the endometrium does not have the proper qualities for implantation, it will not occur and artificial insemination will fail.

Success rates
It is important to know that there are different ways of expressing the success of an assisted reproduction treatment, as we discuss below:
- Pregnancy rate
- percentage of women with a positive pregnancy test after AI.
- Cumulative pregnancy rate
- percentage of pregnancies after two, three or more attempts. Typically, the AI's cumulative pregnancy rate increases up to 4 attempts.
- Delivery rate
- percentage of women who achieve full-term pregnancy and the birth of one or more babies. In this case, it does not refer to whether the baby is born alive or dead, or with some malformation, pathology or disease.
- Live birth rate
- percentage of women who achieve the birth of a live and healthy baby after AI.

For all this, the live birth rate is the most important. However, the SEF only provides data on the pregnancy rate and the delivery rate for each type of AI, so these are the percentages that we will provide below (National Activity Registry 2021-SEF Registry).
Conjugal artificial insemination
According to the latest report published by the SEF with the results obtained by Spanish centers in 2021, artificial insemination with partner semen (IAC) has the following success rates depending on the age of the woman:
- Women <35 years old
- pregnancy rate of 14.3% and delivery rate of 11.8% per cycle.
- Women 35-39 years old
- pregnancy rate of 13.1% and delivery rate of 9.4% per cycle.
- Women ≥ 40 years old
- pregnancy rate of 6.4% and delivery rate of 3.3% per cycle.

It is very likely that the woman will not get pregnant in the first artificial insemination. However, the cumulative rate of IAC after four attempts reaches up to 60%, so the couple could achieve pregnancy on the second, third or fourth attempt.
Artificial donor insemination
In case of using the semen of an anonymous donor to do the artificial insemination, the probability that the woman has to become pregnant and give birth to a baby depending on her age is the following:
- Women <35 years old
- pregnancy rate of 23.6% and delivery rate of 19.5% per cycle.
- Women 35-39 years old
- pregnancy rate of 18.5% and delivery rate of 13.9% per cycle.
- Women ≥ 40 years old
- pregnancy rate of 19.7% and delivery rate of 5.8% per cycle.

As in the previous case, the IAD has a cumulative pregnancy rate that can reach up to 80% after four attempts.
Statistical data in this article shall not be used to imply or predict an outcome certainty to a specific individual within a population at risk.
Number of AI attempts
As we have pointed out, specialists recommend a maximum number of 4 artificial insemination attempts before moving on to other more complex treatments.
Numerous studies have shown that, after the fourth artificial insemination treatment, the pregnancy rate does not improve and, therefore, it makes no sense to continue applying this method. In this case, it will be necessary to go on to in vitro fertilization (IVF) processes.
However, there is an exception in the case of single women and couples of homosexual women, who may be indicated up to a maximum of 6 IAD attempts.
The reason is that these women, in principle, do not present any infertility problem, only the absence of a male partner.
Did you know that we can help you to choose a fertility clinic for your IUI cycle? All you have to do is get your Fertility Report now. It is an easy-to-use tool that is capable of filtering the best clinics and tailor an individual report exclusively for you with useful tips that will help you make a well informed decision.
Pregnancy test
After about 15 days of beta-waiting, the pregnancy test will make it possible to discover whether or not artificial insemination has been successful. It is based on measuring the beta-hCG hormone, released by the embryo after implantation.
To avoid errors in the result, it is recommended not to do the pregnancy test before 15 days have passed since the AI, since there would be the possibility of obtaining a false negative due to not having enough beta-hCG.

On the other hand, the blood pregnancy test is more specific than the urine test and leads to fewer errors. In any case, we will not have definitive confirmation of the pregnancy until we see the gestational sac and the embryo in the ultrasound at week 6 or 7.
FAQs from users
Is pregnancy possible after artificial insemination if the cervix was somewhat closed?
Pregnancy is possible after AI, even if the cervix is slightly closed. The cannula used for insemination is narrow and is able to pass through the cervix, although it is complicated.
Read more
What can be done after three unsuccessful DAIs?
After having performed three unsuccessful DAI (donor artificial insemination) cycles and having ruled out active tubal and endometrial pathology, constituting an entity without apparent cause, it is advisable to opt for in vitro fertilization (IVF). This reproductive option will provide accurate information on the quality of the eggs, fertilization and embryo evolution.
Are there any concrete symptom indicating that artificial insemination has been successful?
No, the symptoms are the general ones of any pregnancy and usually appear approximately 15 days after insemination. Among the most common are nausea or vomiting, fatigue, sleep ... but do not differ from those produced by a natural pregnancy.
Artificial insemination after 40, does it work?
Age is one of the factors that has the most influence on the success rates of artificial insemination. Not only for the artificial insemination itself or for the number and/or quality of the oocytes (ovarian reserve), but also for the endometrium, since achieving the adequate thickness for the embryo to be able to implant becomes more complicated.
After the age of 35, the ovarian reserve decreases and, therefore, the probability of an egg being fertilized by a sperm is significantly reduced, especially after the age of 40.
Insemination is not recommended after the age of 35-37, since the probability of pregnancy is so low (less than 10%) that it is not worthwhile for the patient to go through the whole process. In these cases, in vitro fertilization is directly recommended.
Read more
I have tubal patency in only one tube. Can I become a mother through IUI?
In the artificial insemination process, fertilization takes place in the Fallopian tubes and, therefore, it is necessary that at least one of them is permeable, that is, it allows the egg and sperm to meet.
If only one of the tubes is functional, achieving pregnancy is more complicated, but not impossible, since fertilization can take place in the other tube.
Does IUI work in women with polycystic ovaries?
Yes, polycystic ovaries can cause infertility problems due to alterations in ovulation. However, with a mild ovarian stimulation cycle, normal menstrual cycles can be recovered and pregnancy achieved, either naturally or by IUI.
Should I move on to IVF after three failed IUI attempts?
Although studies indicate an increase in pregnancy chances after the fourth attempt with artificial insemination, depending on the case, it is possible that, after three failed IUI attempts, your doctor refers you to IVF. This depends on each situation as well as on aspects such as the causes of infertility, the woman's age, the causes that led to failure of previous IUI attempts, etc.
Can I get pregnant through IUI with endometriosis?
It depends on the location and how expanded the endometriosis is. If it is a mild-to-moderate case of endometriosis, then pregnancy could be achieved with this technique.
On the contrary, in the most severe cases, it is likely that the Fallopian tubes are blocked due to this condition, in which case the sperm would not be able to meet the egg. Also, it might have affected the endometrial lining, reducing the embryo's possibilities of attaching to it.
Can you choose the gender of the unborn child with IUI?
No. Since fertilization and subsequent embryo development occur inside the female's body, the embryos cannot be manipulated to examine their genetic content. So, in short, choosing the gender of the baby is not possible.
Recommended readings
Throughout this post, we have seen that the chances of pregnancy vary, amongst other reasons, depending on the type of insemination carried out: whether it is an AIH or an AID. Also, the cost of these types of AI is different, as you can read here: How Much Does Artificial Insemination Cost?
Also, we have made special emphasis on the importance of opting for Intrauterine Insemination (IUI) only in those cases where it is indicated. Otherwise, achieving satisfactory results would be highly unlikely. Want to learn more about the main indications? Click here: Artificial Insemination Indications – Why & When to Use It?
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Berg U, Brucker C, Berg FD. Effect of motile sperm count after swim-up on outcome of intrauterine insemination. Fertil Steril 1997; 67:747–50.
Buxaderas R. (s.f.) Guía 14: Ciclos de inseminación artificial conyugal. Servicio de Medicina de la Reproducción Departamento de Obstetricia, Ginecología y Reproducción Hospital Universitario Quirón Dexeus, Barcelona.
Caballero Peregrín P, Núñez Calonge R, García Enguídanos A. (s.f.) Guía 15: Ciclos de inseminación artificial con semen de donante. Clínica Tambre. Madrid.
DiMarzo SJ, Kennedy JF, Young PE, Hebert SA, Rosenberg DC, Villaneuva B. Effect of controlled ovarian hyperstimulation on pregnancy rates after intrauterine insemination. Am J Obstet Gynecol 1992; 166:1607–13 (View)
Karlstrom P-O, Bergh T, Lundkvist O. A prospective randomized trial of artificial insemination versus intercourse in cycles stimulated with human menopausal gonadotropin or clomiphene citrate. Fertil Steril 1993:59;554–9 (View)
Khan JA, Sunde A, Von During V, Sordal T, Molne K. Intrauterine insemination. Ann NY Acad Sci 1991;626:452–60 (View)
Sociedad Española de Fertilidad. Registro Nacional de Actividad 2021-Registro SEF (View)
Tomlinson MJ, Amissah-Arthur JB, Thompson KA, Kasraie JL, Bentick B. Prognostic indicators for intrauterine insemination (IUI): statistical model for IUI success. Hum Reprod 1996;11:1892–6 (View)
Plosker SM, Jacobson W, Amato P. Predicting and optimizing success in an intrauterine insemination programme. Hum Reprod 1994;9:2014–21 (View)
FAQs from users: 'Is pregnancy possible after artificial insemination if the cervix was somewhat closed?', 'What can be done after three unsuccessful DAIs?', 'Are there any concrete symptom indicating that artificial insemination has been successful?', 'Artificial insemination after 40, does it work?', 'I have tubal patency in only one tube. Can I become a mother through IUI?', 'Does IUI work in women with polycystic ovaries?', 'Should I move on to IVF after three failed IUI attempts?', 'Can I get pregnant through IUI with endometriosis?' and 'Can you choose the gender of the unborn child with IUI?'.
Authors and contributors









More information about Michelle Lorraine Embleton

Hi, My partner has had 4 cycles of IUI now and still we aren´t pregnant. We are a gay female couple and live in the London area, and hoping to get some treatment on the NHS as it is costing us a fortune. Is there any chance of this? Thanks
Hi Queerme
Depending on your age and area, it may be possible for you to get treatment on the NHS after 6 previous attempts. However, it is worth consultingwith your GP as the guidliones are currently changing to make them more accessible and fair to modern family structures. This video may also be useful for you:
Good luck and I hope this answer was helpful.
I want to know what the chances are to get pregnant on the first try doing AI
Hello flow,
AI has different success rates based on the woman´s age, underlying conditions, and if you are using spousal or donated sperm. There is an estimated pregnancy rate of 18% per cycle using donor sperm and that can go up to 80% after 4 cycles.
On the other side, if you use spousal sperm the chances of pregnancy are 13% on the first cycle that can go up to 60% after 4 cycles.
I hope I have helped,
All the best
Hello, I got my tubes tied a couple of years ago, I met another partner and want to have a baby, I know we can’t conceive naturally, but I’m wondering if we could do AI. He doesn’t have any problem with his sperm. Thanks
Hello Alyssa,
You couldn´t perform Artificial Insemination with your tubes tied, for this technique to work the tubes have to be functional because there is where the egg would meet the sperm.
You have a couple of options, you could for IVF, a technique in which you don´t need your tubes to be functional, or a tubal ligation reversal, which consists of a procedure to reverse your initial surgery and give function back to your tubes. It should be noted that this reversal doesn´t have high chances of restoring fertility, therefore, this should be consulted with a professional that can asses your particular case.
I hope I have helped,
All the best.
Hello, I’m in doubt if I will have to repay in case my first artificial insemination cycle is unsuccessful or if it is foreseen when they give you the prices at the beginning until you achieve pregnancy. Thanks!