There are several types of fertility treatments and assisted reproductive techniques that can help infertile men and women achieve pregnancy and fulfill their dream of parenthood.
The most widely used treatments, and therefore the best known in today's society, are artificial insemination (AI) and in vitro fertilization (IVF).
Each of these techniques is indicated for different patients and different fertility problems. Therefore, it is very important to be familiar with them and to know which treatment is the most appropriate to ensure success.
Provided below is an index with the 7 points we are going to expand on in this article.
- 1.
- 2.
- 2.1.
- 2.2.
- 2.3.
- 2.4.
- 3.
- 3.1.
- 3.2.
- 3.3.
- 3.4.
- 3.5.
- 3.6.
- 3.7.
- 4.
- 5.
- 6.
- 7.
Choosing your fertility treatment
All couples who do not achieve pregnancy after one year of unprotected sex should start to see a fertility clinic to have their infertility tested.
The recommended waiting time is reduced to 6 months in women over 36 years. Neither will it be necessary to wait if there are obvious problems of sterility.
Once the results of the fertility tests have been obtained, which include hormone analysis, ultrasound and semen analysis, the specialist assesses which technique is the most suitable for each case. Some of the aspects that are taken into account are the following:
- Woman's age
- Ovarian reserve
- Permeability of the Fallopian tubes
- Semen quality

The specialist will have to explain all this information to its patients and the reasons why one or another technique is recommended such as the procedures, risks, success rates, etc and so on.
However, ìt is the patients themselves who have to accept whether to do an artificial insemination or in vitro fertilization, and sign the appropriate consent forms to start the treatment.
Differences between insemination and IVF
AI is a simpler technique than IVF and, therefore, is the first treatment indicated on many occasions. This reproductive option consists of depositing capacitated sperm, previously obtained in the laboratory, inside the woman's uterus. For this purpose, the patient is subjected to a slight ovarian stimulation.
The sperm swim into the fallopian tubes (where the egg will be) and fertilization takes place naturally. For this, it is necessary for the woman to have permeable fallopian tubes and for the man to have good seminal quality.

On the other hand, IVF is a more complicated technique. After controlled ovarian stimulation, the woman's eggs are removed through a surgical procedure known as follicular puncture.
The retrieved eggs are fertilized in the laboratory with the couple's or a donor's sperm, and then the best quality embryo or embryos are transferred to the woman's uterus for pregnancy to take place.
When to do AI and when IVF?
Artificial insemination is usually indicated when infertility problems are minimal or as a first strategy in the face of sterility of unknown origin.
As we have said, it is necessary to meet certain prerequisites and, therefore, its indications are as follows:
- It is advisable for women under 35-37 years of age.
- Ovulation alterations or ovarian reserve alterations should be minimal.
- Patients must present tubal patency and no evidence of severe male fertility problems.
- As for the male partner, his semen sample must reach the minimum values, with a Motile Sperm Concentration (MSC) of at least 3 million sperm.

When infertility problems are more severe or the woman is older than 37, the most appropriate treatment is IVF. Below, we will comment on its most frequent indications:
- Women with low ovarian reserve.
- Blocked Fallopian tubes or women with tubal ligation.
- Moderate or severe male factor: oligozoospermia, asthenozoospermia, teratozoospermia, etc.
- Previous failures of artificial insemination.

In the most severe cases, it will be necessary to use the ICSI technique (intracytoplasmic sperm injection) to fertilize the eggs during an IVF. If you want to know the indications for this particular technique, you can read more here: When Is ICSI Recommended?
Medication for ovarian stimulation
In both AI and IVF, it is necessary to administer hormonal medication to the woman so that controlled follicular development takes place.
In the case of AI, the dose of gonadotropins (FSH and LH) will be much lower than in IVF, since the aim is to achieve only one or two mature follicles for insemination. If a greater follicular development were obtained, there would be a risk of multiple pregnancies.
In in vitro fertilization, on the other hand, ovarian stimulation is greater to achieve a multiple follicular development which results in the production of a high number of eggs and thus increases the possibility of obtaining good embryos.
It is normal to obtain between 6-10 eggs per IVF cycle. After fertilization and embryo transfer, the remaining embryos are vitrified for use in future attempts or to have a second child.
Whether you need to undergo IUI or IVF to become a mother, we recommend that you get your Fertility Report now. In 3 simple steps, it will show you a list of clinics that fit your preferences and meet our strict quality criteria. Moreover, you will receive a report via email with useful tips to visit a fertility clinic for the first time.
Cost
The cost of a fertility treatment might vary from clinic to clinic. However, whatever the final cost is, there is a significant difference between the cost of artificial insemination and in vitro fertilization.
The cost of artificial insemination may range from $400 to $4,000, whereas in vitro fertilization can reach $12,000 and even $14,000, as it includes surgery, egg fertilization in the laboratory and the subsequent embryo transfer. Given that the entire process requires more involvement of the specialist, it implies a higher overall cost.
Even though fertility medication is not usually included in the overall cost by default, patients are advised to add the cost of medications, as it may vary greatly. For intrauterine insemination, ovulation induction drugs may cost from $600 to $1,000, while in the case of in vitro fertilization it is around $2,000- $6,000.

Related topic: Overview of the Main Costs of Fertility Treatments.
Success rates
Success rates also vary significantly between AI and IVF.
Obviously, with IVF there is a greater chance of achieving pregnancy because the 3 or 5-day old embryo already developed is introduced into the uterus. The only thing that has to occur naturally in the woman is implantation.
Next, we are going to comment on the birth rates achieved in both techniques depending on the age of the woman, according to the latest data published by the Spanish Fertility Society (SEF) for the year 2023.
- Women under <35 years old
- the birth rate for IUI is 14.1%, whereas the birth rate per transfer in IVF-ICSI is 33.7%.
- Women between 35 - 39 years
- the birth rate for IUI is 11.1%, whereas the birth rate per transfer in IVF-ICSI is 25.9%.
- Women ≥40 years old
- the birth rate for IUI is 6.0%, whereas the birth rate per transfer in IVF-ICSI is 12.8%.
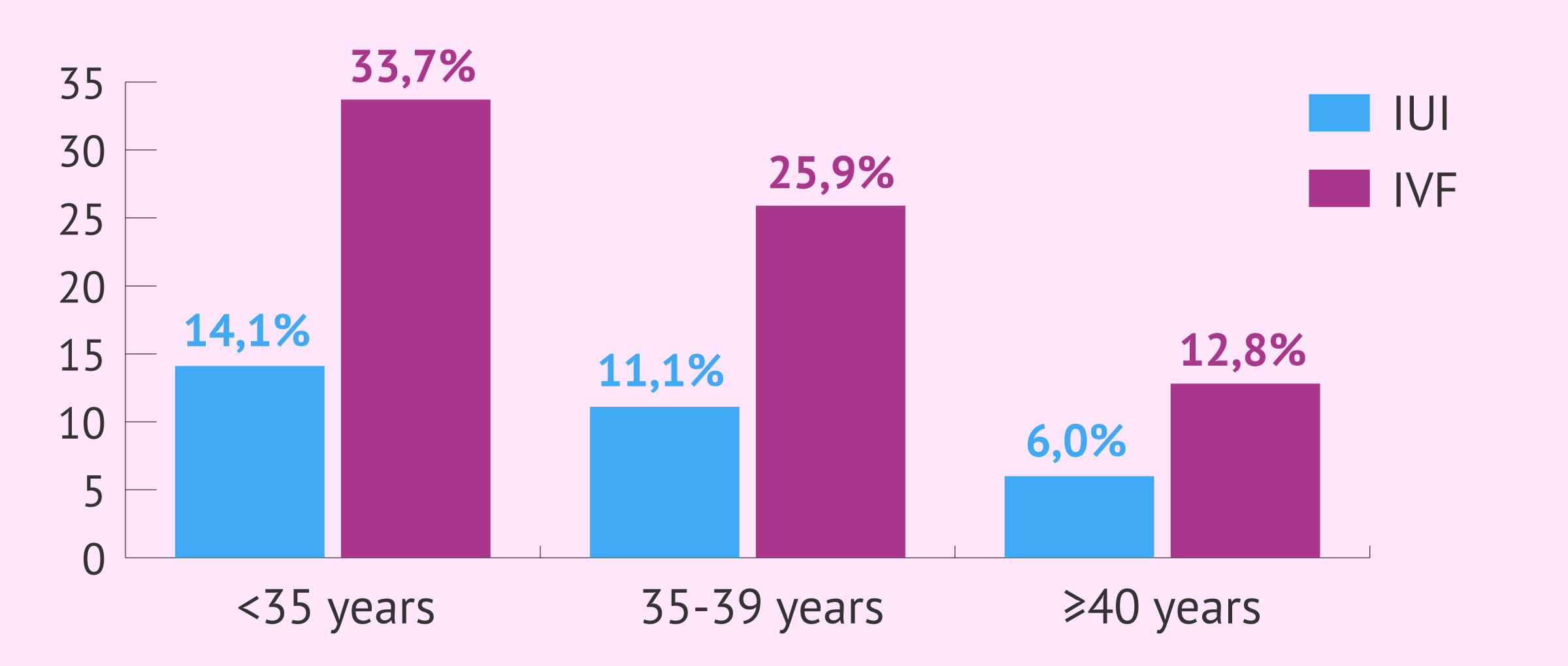
As you can see from the figures, age is a very important factor when deciding on an assisted reproduction technique. However, these values also depend to a great extent on the cause of sterility.
In conclusion, there is no one technique that is better than the other. Each treatment must be adapted to each type of patient and all the procedures must be personalized as much as possible to increase success rates as much as possible.
Statistical data in this article shall not be used to imply or predict an outcome certainty to a specific individual within a population at risk.
FAQs from users
Does it help IVF if artificial insemination attempts have been previously performed?
With Artificial Insemination, success rates of up to 30% (depending on the age of the patient) can be achieved after 3-4 attempts. If pregnancy is not achieved after these attempts, we usually propose a more complex treatment such as in vitro fertilization (IVF).
The fact of having carried out an ovarian stimulation treatment prior to artificial insemination allows us to see how the ovary responds to the medication, even if it is at much lower doses. It also allows us to know how the endometrium is developing and if there are any problems at that level.
We definitely start the cycle with more information than if we had not performed any previous stimulation, although the techniques are usually very different in terms of doses of hormonal medication, the objective with IVF being to recruit a large number of follicles, while with artificial insemination, the maximum is 2.
Does artificial insemination involve the same risks as in vitro fertilization?
All fertility treatment cycles involving ovarian stimulating medication have similar risks but the difference is the degree of severity. For cycles using only oral or injectable fertility medications, the risks of an ectopic pregnancy, ovarian hyperstimulation syndrome and ovarian torsion are less than 5% in both IUI and IVF cycles.
The difference between IUI and IVF are the pregnancy success rates and risk of multiple births. In an IUI cycle using oral medication, the risk of a multiple pregnancy is less than 5% but increase to 10-15% when injectable fertility medications are used.
The unique distinction of IVF is the ultrasound guided vaginal egg retrieval and the ability to transfer a predetermined number of embryos. As a result, the risks with an egg retrieval included intra-abdominal bleeding, injury to the bowel and bladder, and infection. Fortunately, all of complications occur in less than 1% of cycles. Further, the risk of a multiple pregnancy is directly related to the number of embryos transferred: a single embryo transfer has a 1% risk of dividing into a twin pregnancy; a double embryo transfer can increase the risk of a twin pregnancy in up to 40% of cycles.
Is the success rate higher in AI or IVF?
Undoubtedly, in vitro fertilization (IVF) has higher gestation rates than artificial insemination. In fact, artificial insemination is not recommended after 37 years of age.
At present, AI should be reserved for very young women (<35 years) and with less than two years of infertility, for women without a male partner or in homosexual families.
Is AI or IVF more effective?
Because it is a more controlled treatment, IVF is much more effective than AI. Thanks to IVF, we can observe the quality of the oocytes, the evolution of the embryos and select the best embryo for transfer.
IVF makes it possible to detect failures in fertilization or during embryo development and to better diagnose cases of infertility. On the other hand, if the result of an AI is negative, we will not know if the fertilization was performed correctly, since it occurs in the woman's body.
To achieve greater effectiveness of IVF, we can use the technique of Preimplantational Genetic Diagnosis, which will help in the selection of embryos according to their genetics.
How many IUI cycles should you do before moving on to IVF?
In couples with a good prognosis, that is, under the age of 37, with a normal sperm sample, we recommend 4 IUI attempts before moving on to IVF. In the case of single women or donor insemination cycles, up to 6 attempts are recommended. It depends on the clinical history of each patient, though.
Which technique is best for single women or lesbian couples trying to get pregnant - IUI or IVF?
No one assisted reproduction technique is better than another; it depends on each situation and the characteristics of each patient. What is clear is that all women without a male partner who wish to become mothers can fulfill their dream thanks to sperm donation.
In principle, if the woman has no problems, her fallopian tubes are permeable, and she has a good ovarian reserve, she can resort to artificial insemination with donor sperm (AID) to become a mother. However, if the woman is over 36 years old and her ovarian reserve is affected or if her fallopian tubes are not permeable, she will have to resort to in vitro fertilization (IVF) with a sperm donor.
Are in vitro fertilization and artificial insemination the same thing?
The answer is no. These are two different assisted reproduction treatments.
In vitro fertilization (IVF) is a highly complex technique characterized by the fact that fertilization takes place in the laboratory. The eggs are extracted from the woman by ovarian puncture and fertilized with the sperm of the male partner or a donor. The best quality embryos generated in the laboratory are transferred to the woman's uterus so that they can implant and give rise to a pregnancy.
Artificial insemination (AI), on the other hand, is a low complexity reproductive treatment. In this case, the semen sample, previously capacitated, is introduced into the woman's body. Therefore, fertilization occurs inside the woman's body in AI.
Recommended reading
If you want to learn about artificial insemination in more detail, you can continue your reading with this article: What Is Artificial Insemination (AI)? - Process, Cost & Types
Alternatively, if you are interested in the treatment of IVF, you can find more information in this article: What Is In Vitro Fertilization (IVF)? - Process, Cost & Success Rates
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Agarwal S, Mittal S (2004). A randomised prospective trial of intrauterine insemination versus timed intercourse in superovulated cycles with clomiphene. Indian J Med Res; 120: 519– 522.
Goldberg JM, Mascha E, Falcone T, Attaran M (1999). Comparison of intrauterine and intracervical insemination with frozen donor sperm: a meta-analysis. Fertil Steril; 72(5):792-5 (View)
Gomez-Polomares JL, Juliia B, Acevedo-Martin B, Martinez-Burgos M, Hernandez ER, Ricciarelli E (2005). Timing ovulation for intrauterine insemination with a GnRH antagonist. Hum Reprod;20:368 – 372 (View)
The ESHRE Capri Workshop Group (2009). Intrauterine insemination. Human Reproduction Update; 15 (3): 265–277.64 (View)
Sociedad Española de Fertilidad. Registro Nacional de Actividad 2022-Registro SEF (View)
FAQs from users: 'Does it help IVF if artificial insemination attempts have been previously performed?', 'Does artificial insemination involve the same risks as in vitro fertilization?', 'Is the success rate higher in AI or IVF?', 'Is AI or IVF more effective?', 'How many IUI cycles should you do before moving on to IVF?', 'Which technique is best for single women or lesbian couples trying to get pregnant - IUI or IVF?' and 'Are in vitro fertilization and artificial insemination the same thing?'.
Authors and contributors







More information about Michelle Lorraine Embleton

Hi
I´m 37, and will be 38 on Christmas day! We´ve been told that my my husband doesn’t have great quality sperm but that it can be used. Can we do and IUI or it is better to go straight to IVF? Thanks
Hi Katrina
I don’t know if you have done an AMH test check your ovarian reserve, but at your age IVF would most probably be the best option. The birth rate per transfer in IVF for your age group is 25.3%,
whilst for an IUI the success rate is 11.2%
I hope this helps!
Thanks
In our case, based on my problem (PCOS) and that of my hubby (20% sperm DNA fragmentation), doctor told me to give IUI a try but I said ‘no’, we would go straight for an IVF. I was 34 then and my odds of success with IUI were 15%, whilst those of IVF were 40% and the cost difference was not too abysmal… Besides, with IVF you are likely to have spare embryos that can be frozen for second IVF cycle in case the first one doesn’t work. The result was pregnancy!!! My baby is now 1.5 years old 🙂 Besides, IVF is the only way through which one can see whether she’s got high quality eggs or not. I don’t understand why people are advised to undergo IUI in the first place when they’re actually desperate at a psychological level. It’s like wasting their money…