Oligozoospermia or oligospermia is a sperm pathology that leads to male infertility. It affects the sperm count, which appears diminished on a semen analysis report in comparison with the results of males with normal sperm count.
Oligospermia can be mild, moderate, or severe depending on the sperm count, that is, the number of sperms present in the ejaculate.
A semen sample is considered poor in terms of quality when the sperm count is too low or there are other pathologies such as poor sperm motility (asthenozoospermia), or sperm morphology defects (teratospermia).
Provided below is an index with the 11 points we are going to expand on in this article.
- 1.
- 2.
- 3.
- 3.1.
- 3.2.
- 3.3.
- 4.
- 5.
- 6.
- 6.1.
- 7.
- 7.1.
- 7.2.
- 7.3.
- 7.4.
- 7.5.
- 7.6.
- 7.7.
- 7.8.
- 7.9.
- 8.
- 9.
- 10.
- 11.
Definition
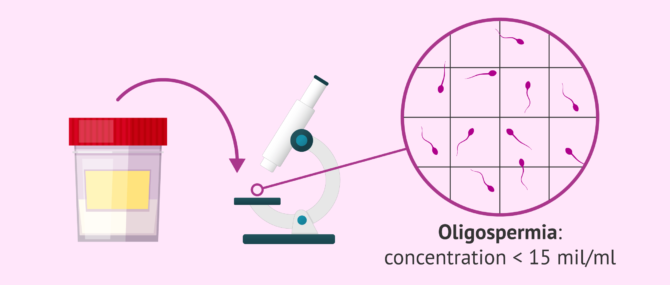
Oligospermia, also called oligozoospermia, is defined as having a low sperm count in the ejaculate.
Oligospermic semen samples are considered of poor quality, and males diagnosed with oligospermia are likely to experience trouble conceiving due to the low amount of sperms able to reach the egg. A poor sperm count reduces the chances for spermatozoa to meet the egg cell inside the female reproductive tract and fertilize it.
According to the World Health Organization (WHO), oligospermia is diagnosed when the total sperm count is lower than 15 million spermatozoa per milliliter of ejaculate.
To learn more about the different ways to evaluate the quality of a semen sample at the laboratory and the reference values taken into consideration, we recommend that you visit the following guide: Measurement of Sperm Quality.
Diagnosis of oligospermia
Oligospermia doesn't have physical symptoms. Men with oligospermia are able to have sexual relations without problems and ejaculate normally. It is when they wish to have a child that, after failing to do so, tests are carried out and this alteration is found.
For the study of semen quality, a test called seminogram is performed to evaluate several semen parameters. One of these parameters is the sperm concentration which, as mentioned above, must be less than 15 million spermatozoa per milliliter to be considered oligospermia.
However, all the semen parameters analyzed in the semen analysis must be evaluated as a whole and taken into account in order to correctly estimate the quality of a semen sample.
Although the World Health Organization (WHO) has published an update of the Laboratory Manual for Semen Examination and Processing in 2021 (the sixth edition), the most common practice is to continue to follow the criteria of the fifth edition (2010).
In order to perform the semen analysis, semen samples must be collected by masturbation after 2 to 5 days of sexual abstinence. If this period of abstinence is not observed, the semen quality may be affected, and the diagnosis may not be correct.
You can find more detailed information about the diagnosis of this condition in this article: How is oligozoospermia diagnosed?
Causes
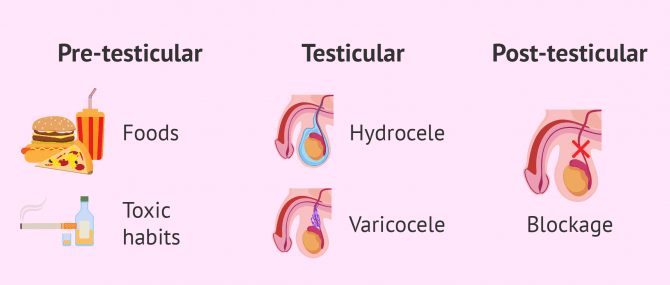
The causes of oligospermia are varied and can be classified into pre-testicular, testicular, and post-testicular factors.
Sometimes, finding the exact cause behind low sperm count is considerably complicated, since oligospermia can occur as a temporary alteration.
Pre-testicular causes
These are those related to problems with the endocrine, hormone system that regulates sperm production and spermatogenesis. This can occur due to hormonal levels that regulate the formation of spermatozoa, or due to external factors that act on our bodies.

Diet, tobacco and alcohol consumption, exposure to environmental toxins or stress are some of the external pretesticular factors that may influence low sperm production.
Testicular causes
When oligospermia derives from a testicular cause, it refers to alterations in the testicles. Among the most frequent testicular alterations are the following:
- Cryptorchidism
- anomaly from birth in the male characterized by incomplete descent of one or both testicles.
- Hydrocele
- accumulation of a large amount of fluid in the spermatic cord.
- Varicocele
- dilatation of the veins of the spermatic cord due to impaired blood circulation.

Some genetic alterations, such as microdeletions in the Y chromosome or trauma, also affect testicular function.
If you want to know about other sperm alterations that cause infertility in men, you can consult the following article: Male infertility due to sperm factor: causes and treatments.
Post-testicular causes
The low concentration of spermatozoa in the ejaculate due to a postesticular cause refers to problems in the expulsion of the spermatozoa to the exterior. Therefore, in this case there is sperm production, but the sperm do not leave the body.
The following are some of the postesticular causes that can lead to oligozoospermia:
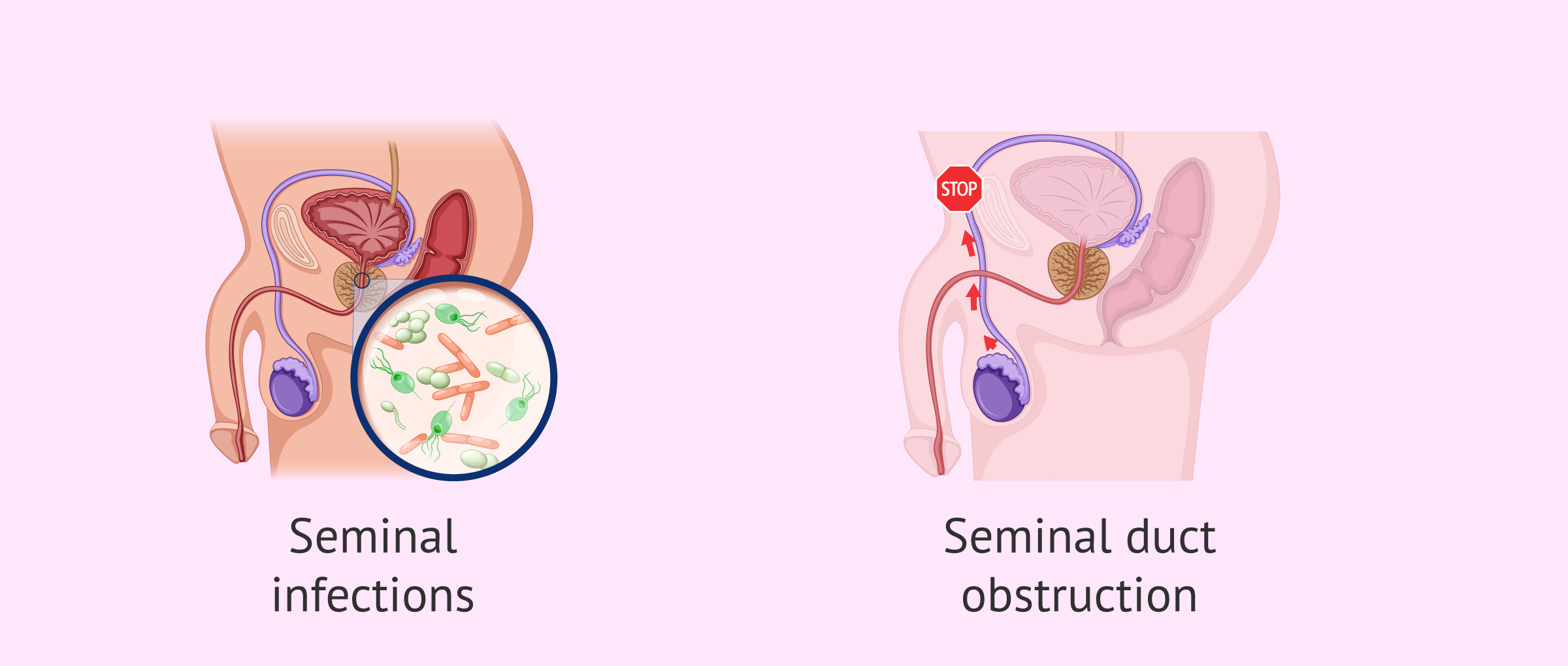
- Obstruction of the spermatic ducts
- due to trauma or infection in the adjacent areas, which prevents the passage of spermatozoa.
- Seminal infections
- either in the prostate, epididymis, vas deferens or urethra.
If you want to learn more about this topic, we recommend you continue reading here: What are the possible causes of oligozoospermia?
Types of oligospermia
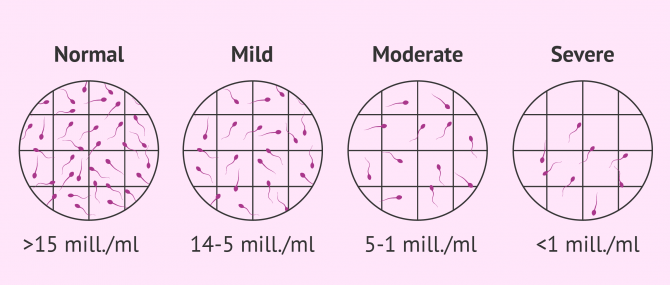
The type of oligospermia can be mild, moderate or severe, depending on whether the concentration of sperm in the ejaculated semen is higher or lower.
- Mild oligospermia
- when the number of spermatozoa found in the semen sample ranges between 14 and 5 million sperm per milliliter.
- Moderate oligospermia
- the sample contains between 5 and 1 million sperm/ml. Great improvements can be achieved in these cases following the proper treatment and a healthy lifestyle for a few months. The semen analysis would be repeated after a few months.
- Severe oligospermia
- Less than 1 million sperm/ml are found. Assisted Reproductive Technology (ART) is recommended to try for a baby.
For the diagnosis to be accurate, the specialist needs to evaluate several semen analyses done in different weeks. This helps to dismiss the possibility that low sperm count is associated with long abstinence periods or a temporary problem.
To learn more about the types of oligospermia you can access this article: Oligospermia types - mild, moderate and severe.
Treatment
First of all, for the treatment of oligospermia, it is important to differentiate whether the cause that is producing this alteration is known. If the cause is known, the treatment will vary according to the specific cause and can range from antibiotics to corrective surgery.
Alternatively, if the exact cause that is not known, the best treatment for oligspermia is to maintain healthy lifestyle habits: eat a balanced diet, reduce or eliminate the consumption of alcohol, tobacco and drugs and protect yourself from toxic substances related to the environment or work.
As natural or "home" treatment we can find some herbs such as Mucuna pruriens (velvet bean),Tribulus terrestris, Korean ginseng or Peruvian maca. However, more well-designed studies are needed to show the effectiveness of all these remedies.

As for the use of drugs, there are vitamin complexes that, although they are not treatments of proven reliability, can help improve sperm production. In addition, hormonal treatments are useful for those patients who suffer from imbalances in the hormones that act on sperm production.
Finally, if sperm production cannot be improved, assisted reproductive treatment should be used to achieve pregnancy.
We discuss in further detail the different treatment options that exist for oligozoospermia in this article: What treatment options exist for oligospermia?
How to get pregnant
Although oligospermia is a major cause of male infertility, men with low sperm count are still able to produce sperm and expel them with ejaculation. In other words, natural conception is still possible. The chances, however, diminish eventually as the sperm count lowers.
For this reason, a fertility treatment could be the best option for those couples who find themselves in this situation. We discuss this in the following section.
Assisted Reproduction Techniques (ART)
Depending on the severity of the oligospermia and/or if sperm alterations are present, pregnancy can be achieved with the help of the diverse techniques of assisted reproduction. The specialist will recommend one technique or another depending on the possibilities.
With mild oligospermia, artificial insemination (AI) is a simple and inexpensive technique that offers good results, provided that it is possible to recover 3-5 million progressive motile spermatozoa after sperm capacitation. In addition, it is also recommended that the woman is under 35 years of age and does not suffer from infertility problems.
If you need to undergo IVF to become a mother, we recommend that you generate your Fertility Report now. In 3 simple steps, it will show you a list of clinics that fit your preferences and meet our strict quality criteria. Moreover, you will receive a report via email with useful tips to visit a fertility clinic for the first time.
If artifical insemination faile, or in the face of moderate or severe oligospermia, the recommendation is to try the technique known as IVF, whether it be by conventional in vitro fertilization or by ICSI.
However, in cases of severe oligospermia, ICSI is more effective, since only one live spermatozoon is needed in the ejaculate for each egg obtained, to microinject it directly into the egg and fertilize it.
You can read about the trying to achieve pregnancy with oligospermia in the following article: Chances of achieving pregnancy with oligospermia.
FAQs from users
Is there any treatment to achieve natural pregnancy with oligozoospermia?
Decreased sperm concentration (Oligozoospermia) could be one of the reasons why pregnancy cannot be achieved in a natural way.
In the clinic we always request a sperm capacitation apart from a semen analysis. In this way we can decide if this sample is suitable for intrauterine insemination (IUI), in vitro fertilization (IVF) or ICSI cycles.
If I have mild oligozoospermia, can I give artificial insemination a try?
Yes, as long as the number of mobile spermatozoa (REM) is greater than 5x106 spermatozoa/ml, but it will also depend on other factors such as the age of the woman or the time of sterility.
Why is oligozoospermia a cause of infertility?
Men with alterations in seminal parameters suffer from male infertility due to the inability to conceive.
In the case of oligozoospermia, as there is a lower number of sperm in the ejaculate, there is less chance that these can ascend through the female reproductive tract to the uterus and fallopian tubes, and reach the egg to achieve a natural pregnancy.
Is 'oligospermia' the same as 'azoospermia'?
No, although oligospermia refers to the low concentration of spermatozoa, they are present in the ejaculate. Azoospermia is the absence of spermatozoa in the ejaculated semen, and invasive techniques are necessary for their recovery, such as epididymal aspiration, testicular puncture or biopsy.
Is oligospermia reversible?
Oligozoospermia is a low sperm count in the ejaculate. This semen disorder is not usually reversible, but it will depend on the patient's case.
Read more
What are the symptoms of oligospermia?
Oligospermia does not have any kind of symptoms such as pain that a man can perceive. A man can have oligospermia and never realize it, unless he wants to have a child and does not succeed. If the oligospermia is due to a pathology such as cryptorchidism or varicocele, these can be seen with the naked eye.
Can oligospermia be treated?
Since it is difficult to know the exact cause of oligospermia, it is also difficult to apply a specific treatment.
It is recommended to maintain a healthy lifestyle, since there are cases in which oligospermia is temporary and sperm production can be restored in a few months.
If the cause of oligospermia is an endocrine defect, a hormonal treatment could be followed.
Is there any oligospermia prevention treatment?
The best way to maintain good seminal quality and the male's fertile potential is to practice healthy lifestyle habits, eat a healthy and balanced diet, not consume drugs, alcohol and tobacco, practice sports to keep in shape, etc.
Is ICSI always performed if the male has oligospermia?
No, it does not have to be the case. If the motile sperm count (REM) after capacitation of the semen sample with oligospermia is higher than 3-5 million, it would even be possible to perform intrauterine insemination (IUI). For this, it is also necessary to take into account the characteristics of the woman, who must be under 35-38 years of age and have no fertility problems.
On the other hand, conventional in vitro fertilization (IVF) could also be performed, but, especially in cases of severe or severe oligospermia, the most indicated technique would be ICSI.
Recommended reading
In this article we have mentioned the seminogram as a test to evaluate the quality of the sperm. If you want to know what this involves, we recommend reading this article: What is a basic semen analysis and how is it done?
If, however, you would like to go into more depth about the techniques available to combat oligospermia and other types of male infertility, we recommend this link: What treatments are available for male infertility?
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Abarikwu SO, Onuah CL, Singh SK. Plants in the management of male infertility. Andrologia. 2020 Apr;52(3):e13509. (View)
Adamopoulos DA. Medical treatment of idiopathic oligozoospermia and male factor subfertility. Asian J Androl. 2000 Mar;2(1):25-32. Erratum in: Asian J Androl 2000 Jun;2(2):158. (View)
Guzick DS, Overstreet JW, Factor-Litvak P, Brazil CK, Nakajima ST, Coutifaris C, Carson SA, Cisneros P, Steinkampf MP, Hill JA, Xu D, Vogel DL; National Cooperative Reproductive Medicine Network. Sperm morphology, motility, and concentration in fertile and infertile men. N Engl J Med. 2001 Nov 8;345(19):1388-93. (View)
Kirby EW, Wiener LE, Rajanahally S, Crowell K, Coward RM. Undergoing varicocele repair before assisted reproduction improves pregnancy rate and live birth rate in azoospermic and oligospermic men with a varicocele: a systematic review and meta-analysis. Fertil Steril. 2016 Nov;106(6):1338-1343. (View)
McLachlan RI. Approach to the patient with oligozoospermia. J Clin Endocrinol Metab. 2013 Mar;98(3):873-80. (View)
Meistrich ML. Effects of chemotherapy and radiotherapy on spermatogenesis in humans. Fertil Steril. 2013 Nov;100(5):1180-6. (View)
Santos HO, Howell S, Teixeira FJ. Beyond tribulus (Tribulus terrestris L.): The effects of phytotherapics on testosterone, sperm and prostate parameters. J Ethnopharmacol. 2019 May 10;235:392-405. (View)
Sermondade N, Faure C, Fezeu L, Lévy R, Czernichow S; Obesity-Fertility Collaborative Group. Obesity and increased risk for oligozoospermia and azoospermia. Arch Intern Med. 2012 Mar 12;172(5):440-442. (View)
Sermondade N, Faure C, Fezeu L, Shayeb AG, Bonde JP, Jensen TK, Van Wely M, Cao J, Martini AC, Eskandar M, Chavarro JE, Koloszar S, Twigt JM, Ramlau-Hansen CH, Borges E Jr, Lotti F, Steegers-Theunissen RP, Zorn B, Polotsky AJ, La Vignera S, Eskenazi B, Tremellen K, Magnusdottir EV, Fejes I, Hercberg S, Lévy R, Czernichow S. BMI in relation to sperm count: an updated systematic review and collaborative meta-analysis. Hum Reprod Update. 2013 May-Jun;19(3):221-31. (View)
Sirotkin AV, Kolesárová A. Puncture vine (Tribulus Terrestris L.) in control of health and reproduction. Physiol Res. 2021 Dec 30;70(Suppl4):S657-S667. (View)
WHO laboratory manual for the examination and processing of human semen, 5th ed. Geneva: World Health Organization ; 2010. (View)
WHO laboratory manual for the examination and processing of human semen, sixth edition. Geneva: World Health Organization; 2021. (View)
FAQs from users: 'Is there any treatment to achieve natural pregnancy with oligozoospermia?', 'If I have mild oligozoospermia, can I give artificial insemination a try?', 'Why is oligozoospermia a cause of infertility?', 'How often should you have intercourse with low sperm count?', 'Is 'oligospermia' the same as 'azoospermia'?', 'Is oligospermia reversible?', 'Is having low sperm count hereditary?', 'What are the symptoms of oligospermia?', 'Can oligospermia be treated?', 'Can low sperm count lead to miscarriage?', 'Is there any oligospermia prevention treatment?', 'When does sperm count decrease with age?', 'How long would it take to get pregnant with low sperm count?', 'Can low sperm count cause quick ejaculation?', 'Is ICSI always performed if the male has oligospermia?' and 'Can low sperm count cause erectile dysfunction?'.
Authors and contributors








More information about Michelle Lorraine Embleton

Hello, can anyone help me? I have had a TMSC semen analysis and was told that I have 1.5 million sperm and that it could not be a natural pregnancy, that it would cost us a lot. What can we do, where can we go? Any help appreciated…
Hi Terry_98,
When the concentration of sperm in the ejaculate is very low, we recommend turning to assisted reproductive techniques to achieve pregnancy. For example, one option for those cases of moderate oligospermia is IVF-ICSI, since only the same number of sperm would be needed as the number of eggs to be fertilized.
In the following article you can get more detailed information about the different reproductive options available: Chances of achieving pregnancy with oligospermia.
If you are looking for fertility clinics, I recommend accessing the Fertility Report. This is a totally free tool with which you will receive a personalized list of the clinics in your area of interest that meet our quality criteria and that best suit your needs. You will get information on prices, services included, detailed explanation of the treatments, useful tips for the first visit, etc.
I hope I have helped you.
Best regards.
When I lift heavy weight or after doing pull ups my sperm count drops.
What should I do to treat it?
What is the treatment of this disease?
Hi there! My husband underwent a seminogram and the result was that he had a low sperm count and his sperm is very slow, Besides, some present abnormal sperm morphology. He is a heavy smoker and I think that’s the cause behind these awful results… Can you tell me if tobacco has indeed an influence on sperm quality? Thanks.
Tobacco consumption affects all parameters of seminal quality, that is to say, morphology, count, and motility. Quitting smoking or at least reducing its consumption together with eating antioxidant-rich foods every day (fruit and vegetables) during at least 3 months in a row may boost his seminal quality.