Oligoasthenoteratospermia (OAT) is the name of a sperm disorder in which three different sperm parameters are affected at the same time: sperm count, sperm motility, and sperm morphology. It is also known as oligoasthenoteratozoospermia.
For a couple in which the male partner suffers from oligoasthenoteratospermia, achieving a natural pregnancy can be complicated. Therefore, it is most likely that the couple will have turn to in vitro fertilization techniques in order to get pregnant and become parents.
Provided below is an index with the 8 points we are going to expand on in this article.
- 1.
- 2.
- 3.
- 3.1.
- 3.2.
- 4.
- 4.1.
- 4.2.
- 4.3.
- 4.4.
- 4.5.
- 4.6.
- 4.7.
- 5.
- 6.
- 7.
- 8.
Definition of the condition
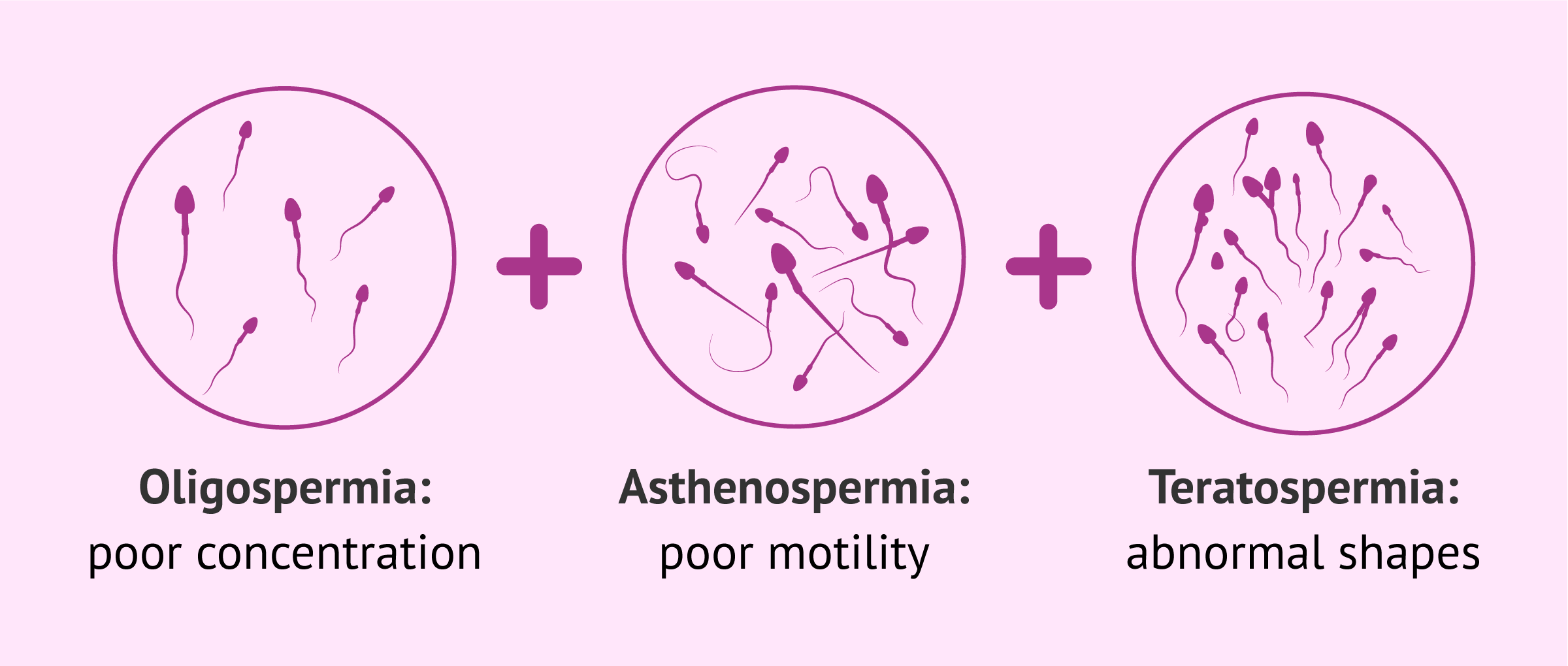
The term oligoasthenozoospermia is result of combining three different sperm abnormailities:
- Oligospermia
- low sperm concentration in the ejaculate, less than 15 million/ml.
- Asthenospermia
- poor sperm motility, more than 60 percent are immotile or less than 32% have progressive motility
- Teratospermia
- abnormal sperm morphology, over 96 percent haveing an abnormal shape.
Oligoasthenoteratozoospermia is, therefore, a cause of male infertility, as the combination of the sperm abnormalities prevents the sperm from being able to meet the egg and fertilize it.
This doesn´t mean that natural conception is impossible, especially if the results of the semen analysis are only slightly below the reference values. However, the chances of achieving pregnancy diminish dramatically with worsening sperm quality.
Causes
Determining the specific causes leading to oligoasthenoteratospermia is hard, mainly because it can be the result of a combination between different factors. Defects in the sperm production process (spermatogenesis), or disorders in the male reproductive system can diminish the sperm quality and potential fertility of the male.
It takes about 3 months to complete the process of spermatogenesis, which involves the sucessive division of the stem cells in the seminiferous tubules. Throughout the process, the cells go through different structural changes until they become sperm cells.
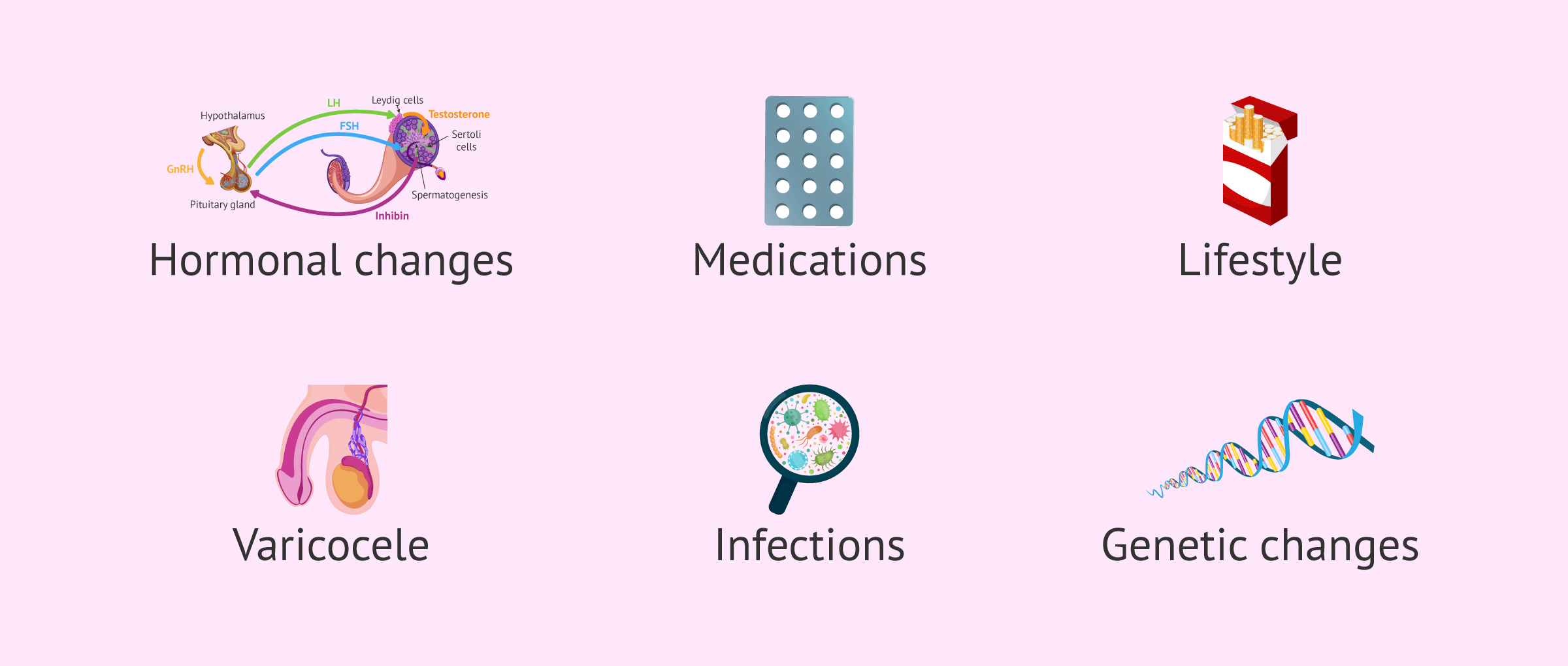
The following are some of the most common causes associated with oligoasthenoteratospermia in males:
- Hormonal alterations affecting spermatogenesis
- Consumption of certain medications, including anabolic steroids, antidepressants, and chemotherapy
- Lifestyle: poor diet, alcohol, smoking etc.
- Testicular birth defects
- Testicular disorders, such as varicocele
- Infections in the seminal ducts, like prostatitis
- Genetic problems that affect sperm production
To try to recover male fertility and improve oligoasthenoteratozoospermia, one can try to correct any hormonal alterations with medication or even correct the testicular problems by surgery. In contrast, if the cause is an infection, antibiotics will be prescribed.
However, for the vast majority of patients with severe oligoasthenoteratozoospermia there is no alternative but to resort to Assisted Reproductive Technology (ART) to become parents.
How to achieve pregnancy
The treatment of OAT will be determined according to the factor or factors that are causing it. If it is due to an easily diagnoised disorder like varicocele, your physician may consider surgery as the best treatment option.
If the problem is a blockage due to an infection, a course of antibiotics is required. In the same fashion, hormonal medication would be used to treat hormone imbalances.

When oligoasthenoteratosoermia is due to idiopathic causes, that is to say an unkown cause, the most appropriate option would be a fertility treatment. Some patients, however, prefer to give a natural remedies a chance before moving on to ART.
Natural remedies
The first thing a man should do after obtaining an OAT diagnosis is to consider changing his lifestyle habits for better general health. Easting a balanced diet, taking moderate exercise and quitting unhealthy habits are all steps that can improve the quality of the sperm in a few months.
Some vitamin supplements and natural remedies can be helpful as well. For example, maca root is a common natural remedy among men that may help to improve sperm quality.
Oxidative stress can have a highly negative impact on sperms due to the influence of reactive oxygen species (ROS), which compromise their functionality. For this reason, adding antioxidants such as vitamin E, vitamin C, and glutathione to your diet can help reduce the impact of sperm damage caused by oxidative stress.

It is important to stress that natural remedies and dietarty supplements should be taken under the guidance of a specialist.
Assisted Reproductive Technology (ART)
If pregnancy is not achieved after one year trying to conceive (or 6 months if the woman is older than 35 - 38 years old), or in cases of severe oligoasthenoteratospermia, fertility treatment may be required in order to become parents.
In cases of severe OAT, the technique of choice is IVF with ICSI (Intracytoplasmic Sperm Injection). Once the semen sample is collected, embryologists study the sample under a microscope and select the sperm cells with the best motility and morphology. These best sperm are then injected directly into the egg cells, with only one sperm cell needed per egg.
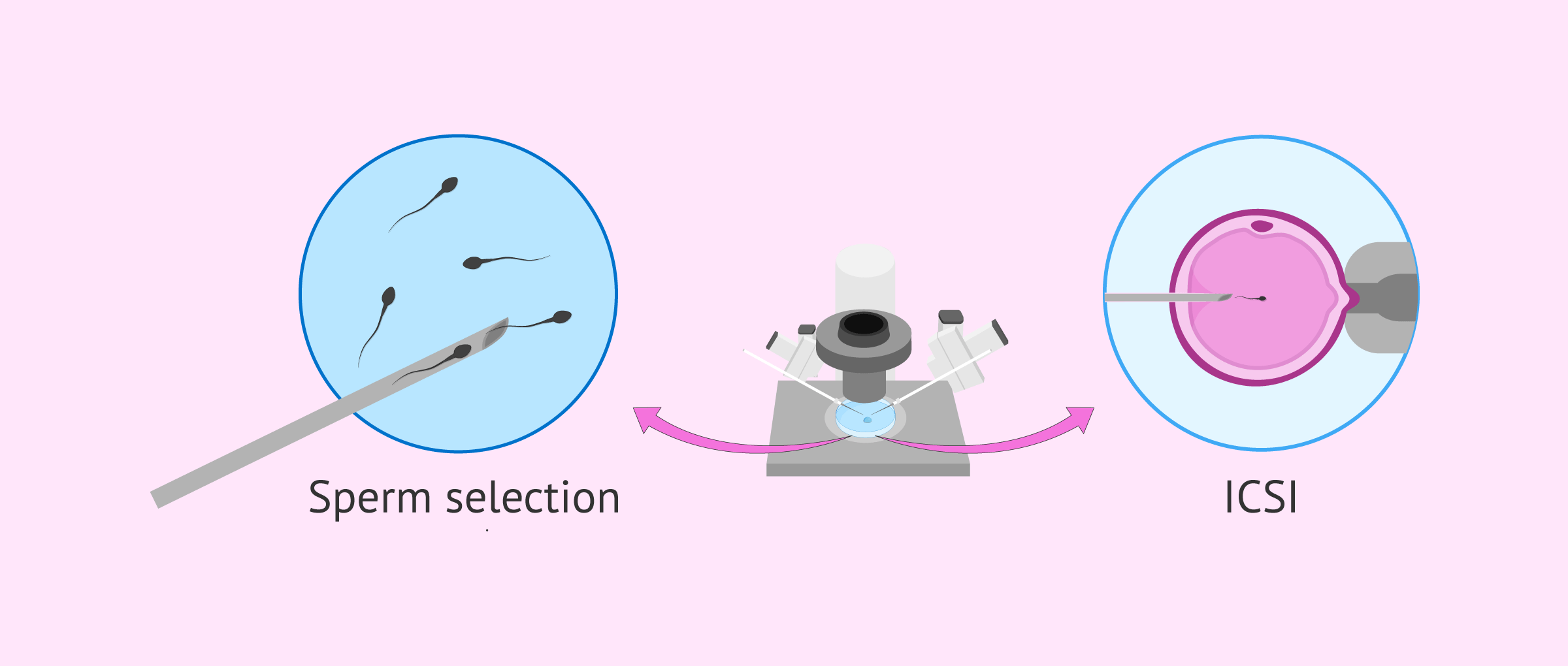
With ICSI, embryologists can to make sure that egg fertilization has taken place and evaluate if it has resulted in viable embryos. The best quality embryo(s) will then be transferred to the uterus of the prospective mother with the aim of implantation and initiating the pregnancy.
If you need to undergo IVF to become a mother, we recommend that you generate your Fertility Report now. In 3 simple steps, it will show you a list of clinics that fit your preferences and meet our strict quality criteria. Moreover, you will receive a report via email with useful tips to visit a fertility clinic for the first time.
FAQs from users
What reproductive options are available for oligoasthenozoospermia?
The clinical picture of oligoasthenozoospermia refers to a combination of several factors. Specifically, it refers to a decrease in the quantity, motility and morphological alterations of spermatozoa.
For this reason, the best option for treatment and achieving pregnancy would be in vitro fertilisation with optimal sperm selection, i.e. IVF-ICSI.
Can oligoastenoteratozoospermia be cured?
Oligoastenothermalospermia may be cured depending on its cause. For example, varicocele can be treated with surgery or hypogonadotropic hypogonadism with hormonal drugs.
In cases where the exact cause of oligoastenatozoospermia is not known, empirical treatment with antioxidants or antiestrogens may be used. These treatments must last at least three months and their effectiveness has not been proven.
Therefore, there are only a few patients with oligoastenothermia who can benefit from a specific treatment, the rest of patients could use empirical treatments and try to lead a healthy lifestyle. In most cases, assisted reproduction is the only treatment for them.
Read more
What is the best treatment for a case of severe oligoasthenoteratozoospermia?
When a man presents a seminogram with these 3 parameters severely affected, that is to say, he has very few spermatozoa with poor movement and morphology, the reproductive options for having children are limited. The assisted reproduction treatment that offers the greatest guarantee of achieving pregnancy is ICSI, since the sperm are individually selected and injected into the egg. With this, embryologists ensure that the eggs are fertilized.
Artificial insemination is not a viable option in a case of oligoasthenoteratozoospermia.
Can you do IUI with oligoasthenoteratospermia?
The pregnancy success rates of IUI in patients with OAT is very low. For an artificial insemination to be effective there needs to be an adequate concentration of sperm with good mobility and movement.
Can oligoasthenoteraozoospermia cause miscarriages?
Oligoastenothermalospermia is not directly related to abortion. However, it is possible that the sperm of these infertile males also possess genetic or chromosomal alterations that impede embryonic development once the embryo has already implanted.
What is mild oligoasthenoteratozoospermia?
Discrete, or mild oligoasthenoteratozoospermia refers to the fact that the affected parameters are not far below the minimum quality values. It is a less severe form of the condition.
How is oligoasthenoteratozoospermia diagnosed?
Oligoastenothermospermia does not have any symptoms in men that might make them suspect that they suffer from male infertility. In order to make a diagnosis, it is necessary for the man to have a seminogram and to evaluate the parameters of concentration, mobility and morphology. Oligoastenatozoospermia is considered to exist when there are less than 15 million spermatozoa per millilitre, a mobility of less than 40% and a percentage of normal spermatozoa of less than 4%.
Recommended reading
The male fertility test that is able to detect sperm abnormalities is the semen analysis or seminogram. Read this post to learn how to interpret the results and the different aspects evaluated: What is a basic semen analysis?.
ICSI is the assisted reproductive technique that is most appropriate for fertility patients with oligoasthenoteratospermia. If you would like to read more about this subject then please visit the following link: Intracytoplasmic sperm injection: What is ICSO and how much is it?
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Auger J, Jouannet P, Eustache F. Another look at human sperm morphology. Hum Reprod. 2016 Jan;31(1):10-23. (View)
Cavallini G. Male idiopathic oligoasthenoteratozoospermia. Asian J Androl. 2006 Mar;8(2):143-57. (View)
Colpi GM, Francavilla S, Haidl G, Link K, Behre HM, Goulis DG, Krausz C, Giwercman A. European Academy of Andrology guideline Management of oligo-astheno-teratozoospermia. Andrology. 2018 Jul;6(4):513-524. (View)
Concepción-Zavaleta M, Paz Ibarra JL, Ramos-Yataco A, Coronado-Arroyo J, Concepción-Urteaga L, Roseboom PJ, Williams CA. Assessment of hormonal status in male infertility. An update. Diabetes Metab Syndr. 2022 Mar;16(3):102447. (View)
Esteves SC. Who cares about oligozoospermia when we have ICSI. Reprod Biomed Online. 2022 May;44(5):769-775. (View)
Hologlu D, Gunes S, Asci R, Henkel R, Guvenc T. Association among sperm chromatin condensation, sperm DNA fragmentation and 8-OHdG in seminal plasma and semen parameters in infertile men with oligoasthenoteratozoospermia. Andrologia. 2022 Feb;54(1):e14268. (View)
Ma J, Wu L, Zhou Y, Zhang H, Xiong C, Peng Z, Bao W, Meng T, Liu Y. Association between BMI and semen quality: an observational study of 3966 sperm donors. Hum Reprod. 2019 Jan 1;34(1):155-162. (View)
WHO laboratory manual for the examination and processing of human semen, 5th ed. Geneva: World Health Organization; 2010. (View)
WHO laboratory manual for the examination and processing of human semen, sixth edition. Geneva: World Health Organization; 2021. (View)
FAQs from users: 'What reproductive options are available for oligoasthenozoospermia?', 'Can oligoastenoteratozoospermia be cured?', 'What is the best treatment for a case of severe oligoasthenoteratozoospermia?', 'Can you do IUI with oligoasthenoteratospermia?', 'What is the miscarriage rate with oligoasthenoteratospermia?', 'Can oligoasthenoteraozoospermia cause miscarriages?', 'What is mild oligoasthenoteratozoospermia?' and 'How is oligoasthenoteratozoospermia diagnosed?'.
Authors and contributors





More information about Michelle Lorraine Embleton

Good evening. I went for a sperm analysis because my partner and I want to be parents but I have now been diagnosed with oligoasthenoteratozoospermia and I am really worried. Are there any natural ways I can cure it?
We have been told that the best way forward is to go for IVF but is this really true? Where can I go to get more information and ideas for treatment? Thanks
Hi James
When a man suffers from oligoasthenoteratozoospermia the best option for getting pregnant is IVF. This is because the concentration, motility and morphology of the sperm are all altered, and as such, it makes is very difficult for the sperm to reach the egg and fertilize it.
Generally, leading a healthy lifestyle with a balanced diet, regular moderate exercise and no smoking can help to improve sperm quality but on many occasions this is not enough.
The best option is to visit a fertility clinic so that they can do the tests needed to work out the best treatment plan for your particular case. For this, we recommend using our Fertility Report, a totally free online tool, from which you will receive a personalized list of the clinics in your area. Furthermore, you´ll get information on prices, services, detailed explanation of treatments etc.
I hope this has helped you.
Best wishes