In recent decades, the probability of multiple pregnancy has increased considerably due to delayed childbearing and the use of assisted reproductive techniques. While in the past the rate of spontaneous multiple pregnancy was between 1-2%, today this rate has risen to 1 in 45 pregnancies.
Multiple pregnancies are considered high-risk pregnancies for both the mother and the babies due to the various changes that the body undergoes throughout gestation and the limited space in the uterus.
For these reasons, people who are going to undergo fertility treatments in order to become parents should be aware of all these risks before making any decisions.
Provided below is an index with the 8 points we are going to expand on in this article.
- 1.
- 1.1.
- 1.2.
- 1.3.
- 2.
- 2.1.
- 2.2.
- 2.3.
- 3.
- 3.1.
- 3.2.
- 4.
- 4.1.
- 4.2.
- 4.3.
- 4.4.
- 4.5.
- 4.6.
- 5.
- 6.
- 7.
- 8.
Risks of multiple pregnancy for the pregnant woman
Multiple pregnancies are complicated by the large volume involved in carrying more than one baby.
The uterus bears an excess of weight and may distend, putting more pressure on the rest of the organs. Giving birth to two or more babies also means a larger placenta and increased hormone levels in the blood.
In short, multiple pregnancies place greater demands on a woman's body and can increase the number of complications experienced in a normal pregnancy. We will now discuss the most common ones.
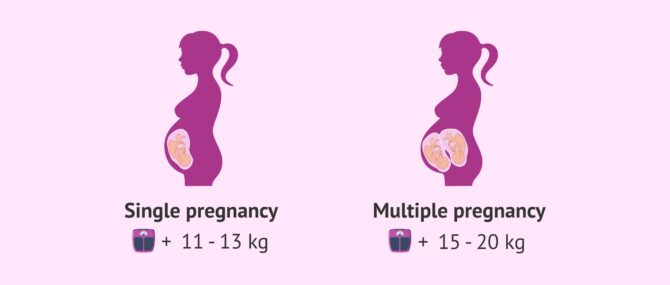
Weight gain.
While it is normal to gain about 11-13 kg in a single pregnancy, the gestation of twins involves an increase of about 15-20 kg in the mother-to-be. This weight gain means greater discomfort for the woman, who may have limited ability to move, difficulty sleeping, increased fatigue, etc.
It is very important the mother to control her weight throughout their pregnancy, as being overweight could lead to major problems.
Preeclampsia
Preeclampsia or pregnancy-induced arterial hypertension occurs in 15-20% of women with multiple gestations. This is three to five times more frequent than in a single pregnancy.
In addition, preeclampsia tends to appear earlier in multiple pregnancies and is also more difficult to control.
More symptoms
Due to the increased hormone production in multiple pregnancy, it is normal for women to experience increased uncomfortable symptoms during the first trimester, such as nausea, vomiting, heartburn, anemia, tiredness and fatigue.
It is also more common for women to suffer from hyperemesis gravidarum, a condition characterized by excessive, intense and persistent vomiting during pregnancy.
Another complication of a multiple pregnancy for the pregnant woman is that she may be moderately or severely iron deficient, i.e. the mother will be anaemic.
You can read more about this syndrome in pregnant women in the following article: What is hyperemesis gravidarum and what are its symptoms?
Complications in the foetus
Fetal and newborn complications in multiple pregnancies are associated with prematurity and low birth weight, since the greater the number of fetuses, the shorter the duration of gestation and the lower the birth weight.
We will now discuss the risks of multiple gestation for twins in the mother's uterus.
Vanishing twin syndrome
This is the loss of one of the fetuses during the first weeks of pregnancy, which is quite common in multiple pregnancies.
In a first ultrasound, two or more fetuses with a heartbeat are observed, but when the ultrasound is repeated after a few weeks, one of the fetuses has disappeared.
What happens is that this fetus is not able to continue growing, stops its development and is finally reabsorbed by the maternal tissues or by the placenta, without giving rise to any complications.
In fact, vanishing twin syndrome poses no risk to the developing baby. Moreover, it is believed to be a natural defense mechanism against what could be a high-risk multiple pregnancy.
Twin-to-twin transfusion syndrome
This is a disorder of the placenta that develops only in identical twins who share the placenta, i.e. in monochorionic gestations.
Both fetuses share their blood vessels and it may happen that one of them receives an excess of blood while the other suffers a significant deficiency.
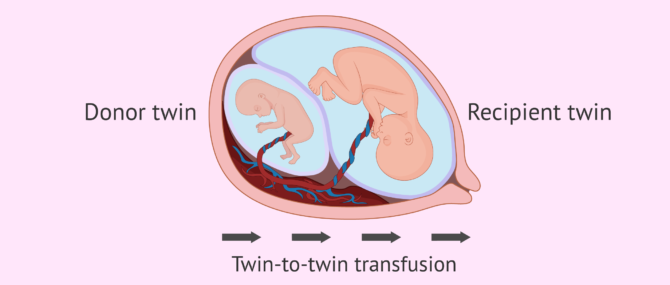
In the worst case, feto-fetal transfusion syndrome can even cause intrauterine fetal death, although fortunately there are several techniques to solve it. The most important thing is to be able to make an early diagnosis in time.
Congenital malformations and Delayed growth
Babies born from multiple pregnancies have twice the risk of congenital anomalies such as the following:
- Neural tube defects such as spina bifida
- Gastrointestinal malformations.
- Cardiac defects
If placental conditions are not adequate, babies may suffer from intrauterine growth retardation (IUGR). This occurs in one of the fetuses in 30% of the cases and in both fetuses in 15% of the cases. In addition, many of the babies of a twin pregnancy are born with a lower birth weight than normal.
Risks of multiple birth
Preterm delivery, before 37 weeks of pregnancy, occurs in more than 50% of twin deliveries, 90% of triplet deliveries and all quadruplet pregnancies.
Below, we will discuss some complications related to the moment of giving birth. These tend to be more frequent in the case of multiple pregnancies.
Placenta previa.
Due to the presence of more than one placenta or a larger placenta, its position may not be correct and it may be placed in the lower part of the uterus.
This abnormality, known as placenta previa, occludes the opening of the cervix, resulting in vaginal bleeding and increasing the risk of premature delivery.
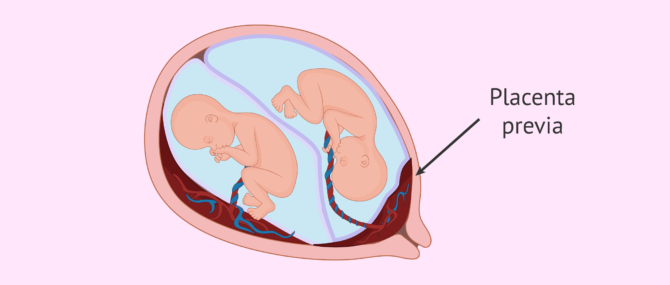
You can read more about this in the following article: What is placenta previa?
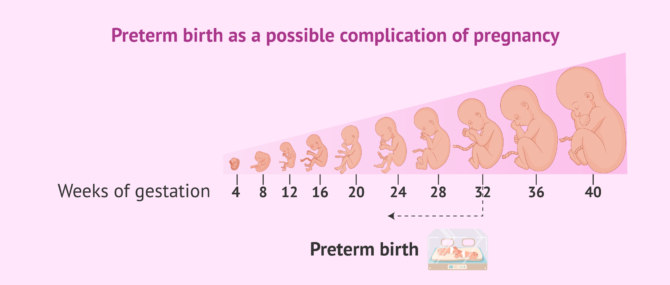
Premature delivery
The average duration of a twin pregnancy is 36 weeks, i.e. before term. This can lead to complications in the fetus as it is not fully developed.
In the most severe cases of prematurity, when babies are born before 32 weeks or weighing less than 1,500 grams, there is an increased risk of:
- Respiratory distress syndrome (RDS).
- Intracranial hemorrhage
- Cerebral palsy
- Blindness.
- Neonatal mortality (during the first month of life).
If you would like to know more about this topic, you can visit the following article: What Is Preterm Birth? - Signs, Causes & Treatment.
FAQs from users
Which specific risks or dangers are involved in a multiple pregnancy?
Although the potential risks for the fetuses and the mother are becoming increasingly controlled and less frequent, it is precisely in cases of multiple births where problems for the mother may raise, such as high blood pressure, diabetes, prematurity, problems at the time of delivery, etc.
As for the baby, the potential dangers are those related to prematurity, most of them considered as mild and transitional, although some may become a serious health issue.
Is a preterm birth more likely with twins?
According to the World Health Organization (WHO), a preterm birth occurs when the child is born before the week 37 of pregnancy. Some of the most common causes of preterm birth are:
- Overdistention of the uterus: loss of tone in the uterine musculature that prevents this organ to recover its normal size.
- Infection or uterine inflammation: certain bacteria can damage fetal membranes by causing its rupture and triggering a preterm birth. An infection that affects the uterus directly may lead to preterm birth as well.
- Decidual bleeding: a type of vaginal bleeding that may occur while a woman is pregnant.
There exist many risk factors that can lead to premature birth, including obesity, high blood pressure, etc. A multiple pregnancy is one of these factors.
What are the particular characteristics of twin births?
First of all, it is important to note that approximately half of twin deliveries occur by cesarean section. The key factor that will lead to one type of delivery or the other is the position of both babies. As there are two of them, it is more complex for both to be well positioned so that vaginal delivery can occur without complications and, for this reason, cesarean delivery is more common than in cases of single birth.
On the other hand, if it is a monochorionic monoamniotic pregnancy, a cesarean section will necessarily have to be performed. Since both babies are in the same placenta and the same amniotic sac, their umbilical cords are more likely to intertwine and lead to complications in vaginal delivery. Therefore, in these cases, cesarean section is usually performed.
What is the usual weight gain for a woman pregnant with twins?
In a single pregnancy, it is recommended not to gain more than one kilogram per month of gestation, although it is usual to gain approximately 10-12 kilos. In the case of multiple pregnancies, the average weight gained by the pregnant woman is between 12 and 17 kilos.
In any case, it will depend on each woman and each situation. It is important to listen to advice from a doctor and specialists in gestational nutrition to avoid excessive weight gain that can lead to complications during pregnancy and childbirth.
What happens when one of the twins dies in utero?
First of all, you have to assess the situation and act in such a way that the other baby is not in danger. It all depends on the length of the pregnancy and whether or not the twins share the placenta.
Generally, it is not advisable to induce labor unless it is strictly necessary. If it is still too early to give birth, it is best to continue with the pregnancy so that the living baby has more time and can develop well. When the time comes, both babies will be born at the same time.
Is there an increased risk of caesarean section in a multiple pregnancy?
Yes, in 50-80% of multiple pregnancies, delivery is by caesarean section. Because there is less space available for the babies, they may adopt abnormal postures rather than the usual cephalic posture. This would increase the need for delivery by caesarean section.
Recommended reading
If you want to continue reading about multiple pregnancies, we recommend the following post: What differs in pregnancy with fraternal twins or identical twins?
If you need more information about childbirth, both natural and cesarean, you can continue reading in the following article: Childbirth: preparation, types and possible complications.
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Embarazo múltiple (395-400). En Matorras R, Hernández J (eds): Estudio y tratamiento de la pareja estéril: Recomendaciones de la Sociedad Española de Fertilidad, con la colaboración de la Asociación Española para el Estudio de la Biología de la Reproducción, de la Asociación Española de Andrología y de la Sociedad Española de Contracepción. Adalia, Madrid 2007. (view)
Ryan GL, Zhang S, Dokras A, Van Voorhis BJ. The desire of infertility patients for multiple gestations - do they know the risks? Fertil Steril 2002; 78 Suppl 1, S67.
Mugford M, Henderson J. Resource implications of multiple births. In: Ward HR, Whittle M, editors. Multiple Pregnancy. London: RCOG Press; 1995; 334-45.
Glinianaia SV, RankinJ, Wright C. Congenital anomalies in twins: a register-based study. Hum Reprod 2008; 23:1306-11.
FAQs from users: 'Which specific risks or dangers are involved in a multiple pregnancy?', 'Is a preterm birth more likely with twins?', 'What are the particular characteristics of twin births?', 'What is the usual weight gain for a woman pregnant with twins?', 'What happens when one of the twins dies in utero?' and 'Is there an increased risk of caesarean section in a multiple pregnancy?'.
Authors and contributors





More information about Michelle Lorraine Embleton

Hi, I´m pregnant with twins (IVF-ICSI) and I am putting on weight fast! I am 39 so not such a young mother to be and I am terrified I won´t be able to get the weight off afterwards. I am, or was, a runner and love my sport. I’ve stopped running for the time being – I couldn´t if I tried as I am permanently exhasuted! Will I be able to exercise as my pregnancy advances? (I´m at 11 weeks now). How easy is it to lose the weight afterwards?
Thanks in advance
Hi Layla
Congratulations on your twins and I can imagine how tired you are feeling at 11 weeks with a mutliple pregnancy!
I would urge you not to panic about the weight gain – if your BMI was in the normal range before pregnany then the recommended pregnancy weight gain for twins is between 20 – 54 pounds. You can read about pregnancy weight gain in our article here.
If you are concerned in any way that you are putting on weight too quickly then do consult your specialist. The same goes for any advice on what exercises you can do to keep healthy and fit.
In pregnancy, many runners turn to walking and pregnancy yoga or pilates, which help both body and mind and can leave you energised.
With regards to losing the extra pounds afterwards, you will be able to return to exercise when your doctor gives you the go ahead. I personally recommend making the time trying to fit some running in again – it will make you feel like yourself again and give you personal space. (I´m also a mom and a runner!). There are also many excellent buggies for running if you can’t get time away then take the babies with you!
Breastfeeding also use the fat deposits laid down in pregnancy, and having 2 babies will mean lots of feeds!
I hope this answers your questions. Good luck with the pregnancy and let us know how you get on.