Multifetal pregnancy reduction is also known as embryo reduction or selective reduction. It is an intervention performed on pregnant women with two or more fetuses in order to reduce the number of fetuses and have a pregnancy without complications.
A multiple pregnancy carries many risks that can endanger the health of the mother and future babies.
Nowadays, assisted reproduction treatments and the high rates of multiple pregnancies achieved have led to an increase in the number of pregnancy fetal reductions. This in turn leads to the development of the technique, which in the past was uncommon.
Provided below is an index with the 8 points we are going to expand on in this article.
- 1.
- 2.
- 3.
- 3.1.
- 3.2.
- 3.3.
- 4.
- 4.1.
- 4.2.
- 4.3.
- 4.4.
- 4.5.
- 5.
- 6.
- 7.
- 8.
What is multifetal pregnancy reduction?
Fetal reduction, also called selective reduction, is the interruption of the development of one or more fetuses during the course of a multiple gestation.
Making this decision is very difficult for prospective parents, especially for those who have achieved pregnancy through fertility treatment and after many years of trying.
However, it is necessary to listen to all the recommendations of the gynecologist so that the pregnancy can evolve favorably and one or two healthy babies can be born.
It is also advisable to seek a second opinion from another physician or psychological assistance so that parents can make sure they are making the right decision.
Reasons for embryo reduction
Usually, embryo reduction is performed when a woman becomes pregnant with triplets, quadruplets or possibly more embryos. However, if the gynecologist considers it to be a high risk pregnancy, it may also be recommended in a twin gestation.
Twin or triplet pregnancies usually have a good prognosis if the mother is in good health. Therefore, embryo reduction is usually only recommended for a quadruplet pregnancy. In all cases, the number of fetusus will be reduced to two.
The risks of a multiple pregnancy that imply the need for fetal reduction are as follows:
- Intrauterine growth retardation
- Intrauterine fetal death
- Premature delivery
- Severe cardiovascular complications
- Uterine rupture and hemorrhage

There is also a psychological and economic component when deciding to perform a fetal reduction, as there are families who do not see themselves able to support all the babies that would be born.
Procedure
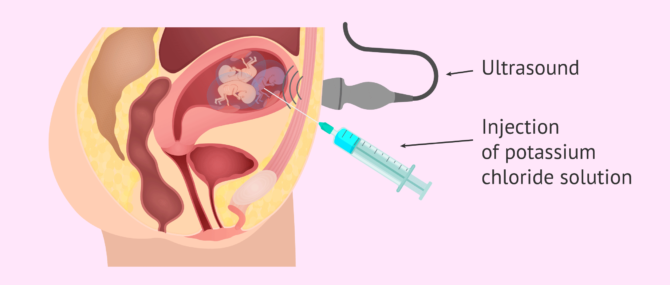
Selective reduction is an operation that can be performed vaginally or abdominally, although the latter is the most frequent.
Under ultrasound guidance, the gynecologist inserts a needle through the woman's abdomen until it reaches the body of the fetus to be removed. Potassium chloride solution is then injected directly into the fetus thorax, which causes the fetus’s cardiac activity to stop immediately.
This procedure is very similar to amniocentesis and is usually performed under local anesthesia.
Within days or weeks of fetal reduction, the fetus or fetuses that have been terminated will be reabsorbed by the tissues of the uterus.
At what moment is selective reduction done?
Embryo reduction is usually performed between 10 and 13 weeks of pregnancy, after the first ultrasound.
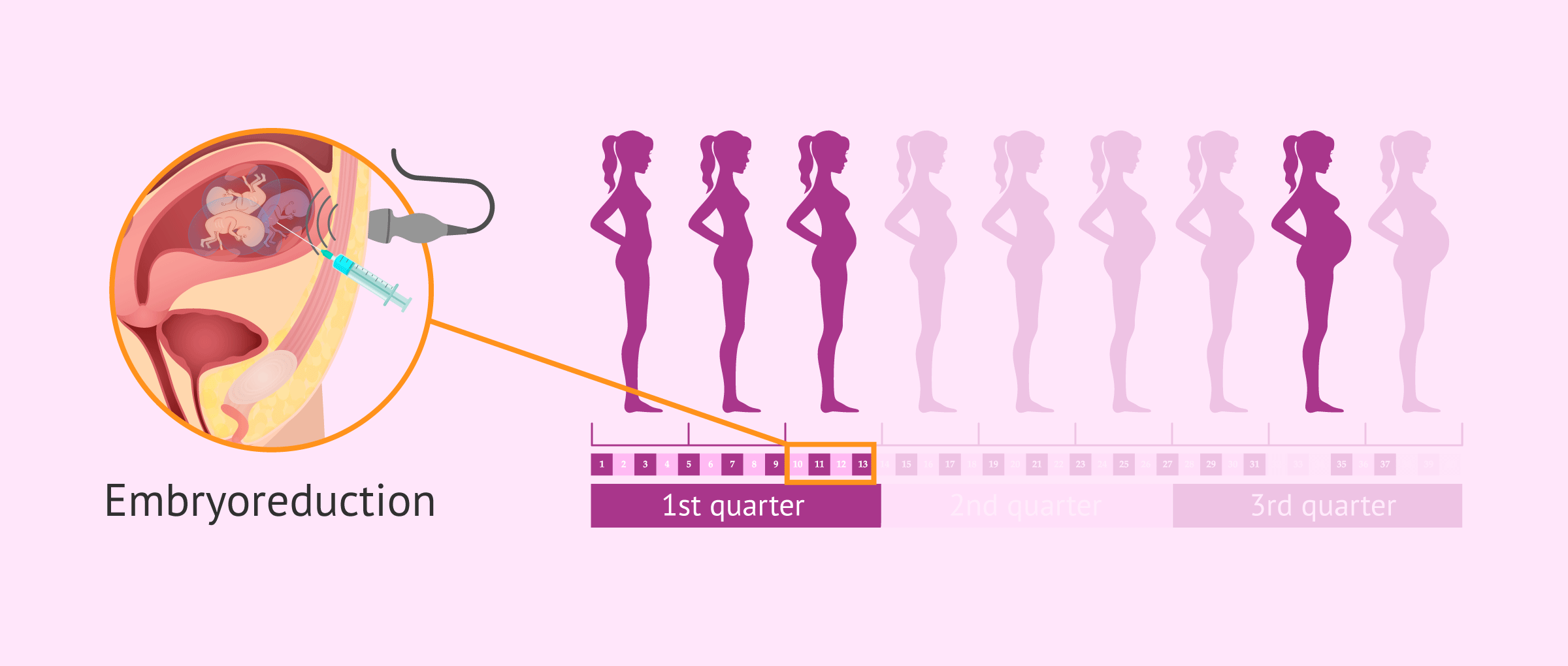
This pregnancy ultrasound reveals certain factors that indicate embryo reduction. Some possible reasons for this include:
- There is a possibility that the embryos may self-reduce naturally during the first trimester of pregnancy.
- At the 12-week ultrasound it is possible to measure certain fetal characteristics, such as the nuchal fold, heart rate or cranio-caudal measurement. These can indicate signs of fetal distress. It is also possible to detect fetal malformations.
- At this time, there is the possibility of non-invasive prenatal testing that provides more information about the fetuses.
- It is necessary to determine whether the pregnancy is monozygotic or dizygotic and, in turn, to know whether the fetuses share a placenta or not.
Thanks to the evaluation of all these factors, the gynecologist can make the best decision as to which fetus or fetuses should be removed so as not to compromise the viability of the rest.
Types of procedure
Depending on how the fetus or fetuses to be removed are chosen, there are the following types of embryo reduction:
- Selective reduction
- when there is evidence that one of the fetuses is less developed or has congenital defects. Evidently, this will be the fetus chosen to stop the development of.
- Non selective reduction
- if none of the signs mentioned above are present, the gynecologist will choose the fetus that is in the most accessible position to introduce the needle.

Possible complications
Embryo reduction increases the probability of survival of the remaining fetuses, as it allows them to develop better and carry to term without problems. Despite this, the technique is not without risks. These are discussed below:
- Spontaneous miscarriage in 6-7% of cases
- Preterm delivery in 75% of cases
- Ovular or intra-amniotic infection
- Hemorrhages
- Psychological consequences

The greater the number of embryos to be reduced and the more advanced the gestation, the greater the risks.
FAQs from users
It is common to have a multifetal rediuction treatment for a multiple pregnancy following a fertility treatment?
Hoy en día los tratamientos de reproducción asistida están encaminados a la transferencia de un embrión único (SET), por lo tanto la posibilidad de embarazo múltiple que precise reducción embrionaria disminuye drásticamente.
Sin embrago, existe la posibilidad de que por diversos factores o preferencias de la pareja se transfieran dos embriones, en ese caso, sí existe más riesgo de embarazo múltiple. La reducción embrionaria va a depender del número de embriones viables en el embarazo, así como del estado de salud de la gestante o los antecedentes personales de la misma (padecimiento de patologías que contraindican gestación múltiple).
What is selective fetal reduction?
Selective feticide consists of the reduction of one or more fetuses of a multiple pregnancy due to genetic anomalies or congenital malformations identified in ultrasounds or tests such as amniocentesis.
The most common cases are those of selective twin feticide, in which the sick fetus is removed and the healthy fetus is allowed to continue its development.
In contrast to embryo reduction, selective fetal reduction is performed later in pregnancy, at the end of the second trimester or beginning of the third trimester, when the parents have obtained the results of all prenatal diagnostic tests. Another difference is the reason for the decision to eliminate the fetus, since in selective feticide the aim is to avoid the birth of a sick baby.
Translated with www.DeepL.com/Translator (free version)
What care is needed after multifetal reduction?
After fetal embryoreduction, it is not necessary for the woman to stay in the hospital, only until the effects of the anesthesia wear off. Once at home, it is recommended that the woman should rest absolutely for the next 48 hours. In the following weeks, it will also be necessary to take relative rest and not to exert herself too much.
About two weeks after the operation, the woman will undergo an ultrasound to check the remaining fetuses have survived.
Why has the incidence of multifetal reduction increased in recent years?
Due to assisted reproductive techniques such as artificial insemination (AI) and in vitro fertilization (IVF), and ovulation-inducing drugs such as clomiphene citrate.
In spite of this, nowadays there is an attempt to make both professionals and patients aware of the risks associated with multiple pregnancy and, for this reason, inseminations with more than two developed follicles and transfers of more than two embryos are not usually performed.
Even so, there is a possibility that one of the embryos may also split, resulting in pregnancies with two identical babies, which may be in the same or different sacs, and one different one.
Is it possible to have a mutlifetal reduction before week 10 of pregnancy?
Yes, it is possible to perform an early embryo reduction around week 7 or 8 of pregnancy. In this case, the procedure will be performed transvaginally, but it will not be possible to evaluate in detail which fetus is to be removed.
Recommended reading
If you want more detailed information on the types of multiple pregnancies, do not miss the following article: Multiple Pregnancies
If you are in the process of an IVF treatment that involves the possibility of having a multiple pregnancy, you may be interested in reading the following post: How many embryos to transfer in IVF
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Ali Javinan, Ramesha Papanna, Tim Van Mieghem, Julie S Moldenhauer, Anthony Johnson, Enrico Lopriore, Amos Grünebaum, Frank A Chervenak, Alireza A Shamshirsaz. Selective termination: a life-saving procedure for complicated monochorionic gestations. J Perinat Med. 2024 Dec 25;53(3):305-310. doi: 10.1515/jpm-2024-0386 (View)
C. Anthoulakis , T. Dagklis , A. Mamopoulos , A. Athanasiadis. Risks of miscarriage or preterm delivery in trichorionic and dichorionic triplet pregnancies with embryo reduction versus expectant management: a systematic review and meta-analysis. Human Reproduction, Volume 32, Issue 6, June 2017, Pages 1351–1359, https://doi.org/10.1093/humrep/dex084 (View)
Sarah Običan, Clifton Brock, Richard Berkowitz, Ronald J Wapner. Multifetal Pregnancy Reduction. Clin Obstet Gynecol. 2015 Sep;58(3):574-84. doi: 10.1097/GRF.0000000000000119 (View)
FAQs from users: 'It is common to have a multifetal rediuction treatment for a multiple pregnancy following a fertility treatment?', 'What is selective fetal reduction?', 'What care is needed after multifetal reduction?', 'Why has the incidence of multifetal reduction increased in recent years?' and 'Is it possible to have a mutlifetal reduction before week 10 of pregnancy?'.
Authors and contributors



More information about Michelle Lorraine Embleton

Hi, I love the idea of having triplets or even quads. Why would I want to reduce my babies to just twins?
Hi TraceyL
There are numerous reasons to opt for multifetal pregnancy reduction, the main ones being the risks involved in a multiple pregnancy to the mother and the babies. If you would like to learn more about these risks you can read this article: Risks of multiple pregnancy.
You should also consider the financial and practical implications of having multiple babies at once.
Having said this, it is the choice of the individual, after receiving medical advice, and counselling may be recommended.
I hope this information is useful!