What is Episiotomy and How Can It be Prevented?
An episiotomy is an incision or cut made in the female perineum (between the vulva and the anus) to increase the vaginal opening and facilitate delivery, thus avoiding tearing of the tissues during the expulsion of the baby.
Traditionally, episiotomy was a routine or at least fairly common technique in vaginal deliveries. Today, however, the World Health Organization (WHO) generally discourages it and only recommends it in certain situations.
In addition, a woman can help prevent an episiotomy by strengthening the pelvic floor with simple exercises throughout the pregnancy.
The different sections of this article have been assembled into the following table of contents.
Contents
- 1.
- 1.1.
- 2.
- 3.
- 4.
- 4.1.
- 4.2.
- 5.
- 5.1.
- 5.2.
- 5.3.
- 5.4.
- 5.5.
- 6.
- 7.
What is episiotomy?
An episiotomy is a surgical technique performed during vaginal delivery that involves making a cut in the skin and muscles between the vagina and anus, an area known as the perineum.
The goal of an episiotomy is to widen the vagina so that the baby can come out more easily and there is no tearing.
Although the current trend is to reduce the number of episiotomies that are not sorely needed during childbirth, they are still performed mostly on nulliparous women (who have not previously given birth).
In the US, episiotomy is performed in approximately 30% of births, while WHO indicates that it is only necessary in 20%. This means that the episiotomy is performed for no reason in the rest of the cases.
Types
Depending on the orientation of the cut, the episiotomy can be classified as follows:
- Midline
- the cut is made horizontally and perpendicular to the anal direction. This type of episiotomy is very rare today.
- Oblique or mediolateral
- the cut is made at a 45-degree angle from the bottom of the vagina to either side. This form of incision is preferred because it offers less chance of tearing and infection. However, scarring is more complicated and increases the risk of bleeding.
- Vertical
- the cut is made in a straight line from the vagina and without reaching the anus. This type of episiotomy has an increased risk of damage to the anal sphincter and rectum, so it is usually not done despite better healing.


Depending on the type of incision and its length, the episiotomy wound may take more or less time to heal, although healing time is usually between four and six weeks.
Indications
In recent years, the number of routine episiotomies has dropped considerably. Numerous studies have shown that it is not necessary in the vast majority of cases and can also be very traumatic for women, causing pain, bleeding and sexual dysfunction.
Both WHO and ACOG (American Association of Obstetricians and Gynecologists) indicate that episiotomy should only be performed in specific cases such as the following:
- Complicated deliveries of very large babies
- Breech delivery
- Births requiring instruments (forceps, suction cups, etc.)
- fetal distress
- Baby presents with shoulder dystocia
- Poorly healed previous third or fourth degree tears
- There is little vaginovulvoperineal elasticity
- The vagina is very narrow and there is an increased risk of tearing

Despite this, there are still situations in which there is some controversy as to whether the specialist did the right thing when performing an episiotomy or whether it could have been avoided.
How episiotomy can be prevented
In order to avoid having an episiotomy or suffering a tear during childbirth, the mother-to-be should take into account some recommendations and pay close attention to her pelvic floor.
The pelvic floor is the set of muscles and ligaments found around the vagina. Therefore, it is essential to strengthen these muscles during pregnancy to avoid complications in childbirth and postpartum.
In particular, to avoid episiotomy, the woman can perform the following actions:
- See a physiotherapist specializing in pelvic floor to make an assessment and follow his indications.
- Attend childbirth classes
- Practice kegel exercises.
- Perineal massage from 32-34 weeks of pregnancy.
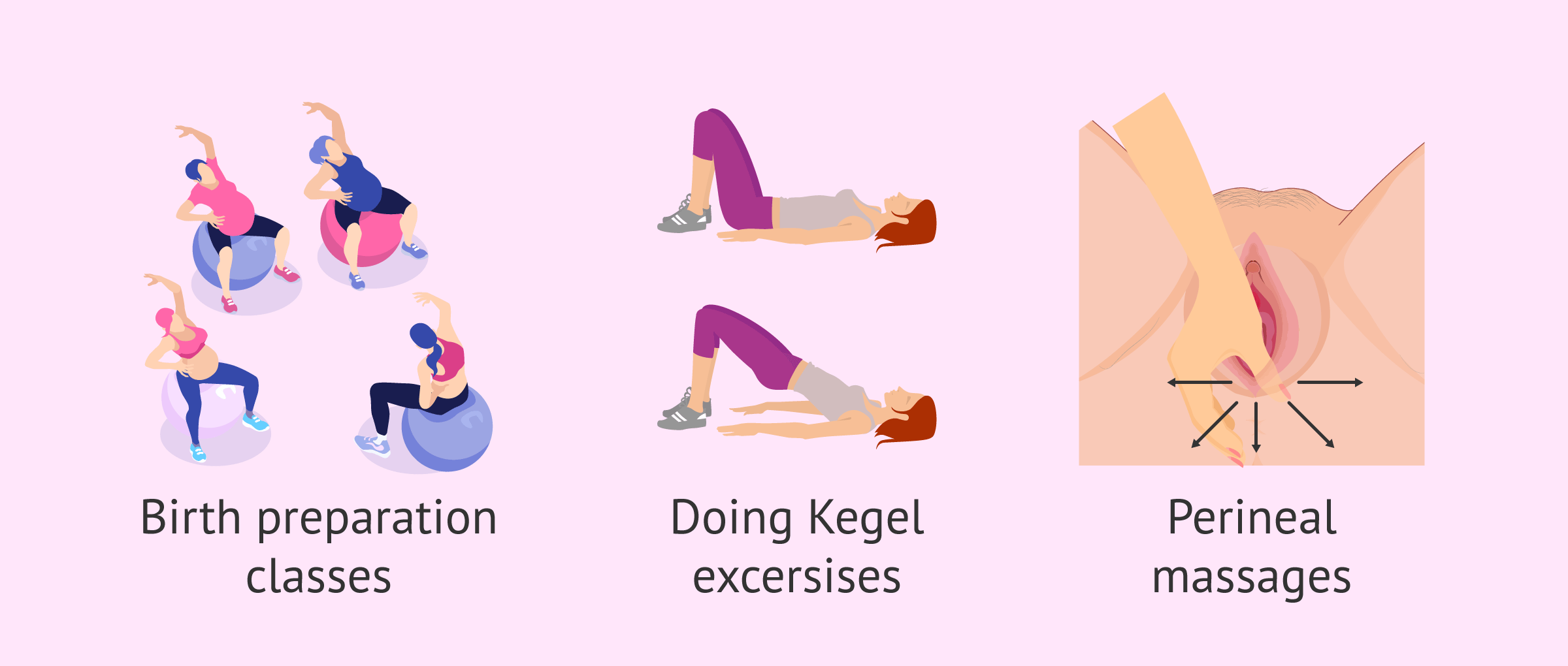
With all this, the pregnant woman will be able to increase the elasticity of the pelvic floor tissues and make them less resistant at the time of delivery.
After the episiotomy
If an episiotomy is performed, the corresponding specialist (gynecologist or midwife) will suture the cut after the baby is born. This process is known as episiorrhaphy.
The stitches used are resorbable, i.e. they do not need to be removed after the wound has closed.
Due to the place where the episiotomy is performed, the healing and recovery of the tissue is somewhat complicated, as it is a humid area and very close to the genitals, which increases the risk of infection.
Complications
Episiotomy can have more or less serious consequences in the woman, especially in her later sexual life.
Some women claim to have experienced the birth of their child as a traumatic experience due to the episiotomy and feel pain even years later.
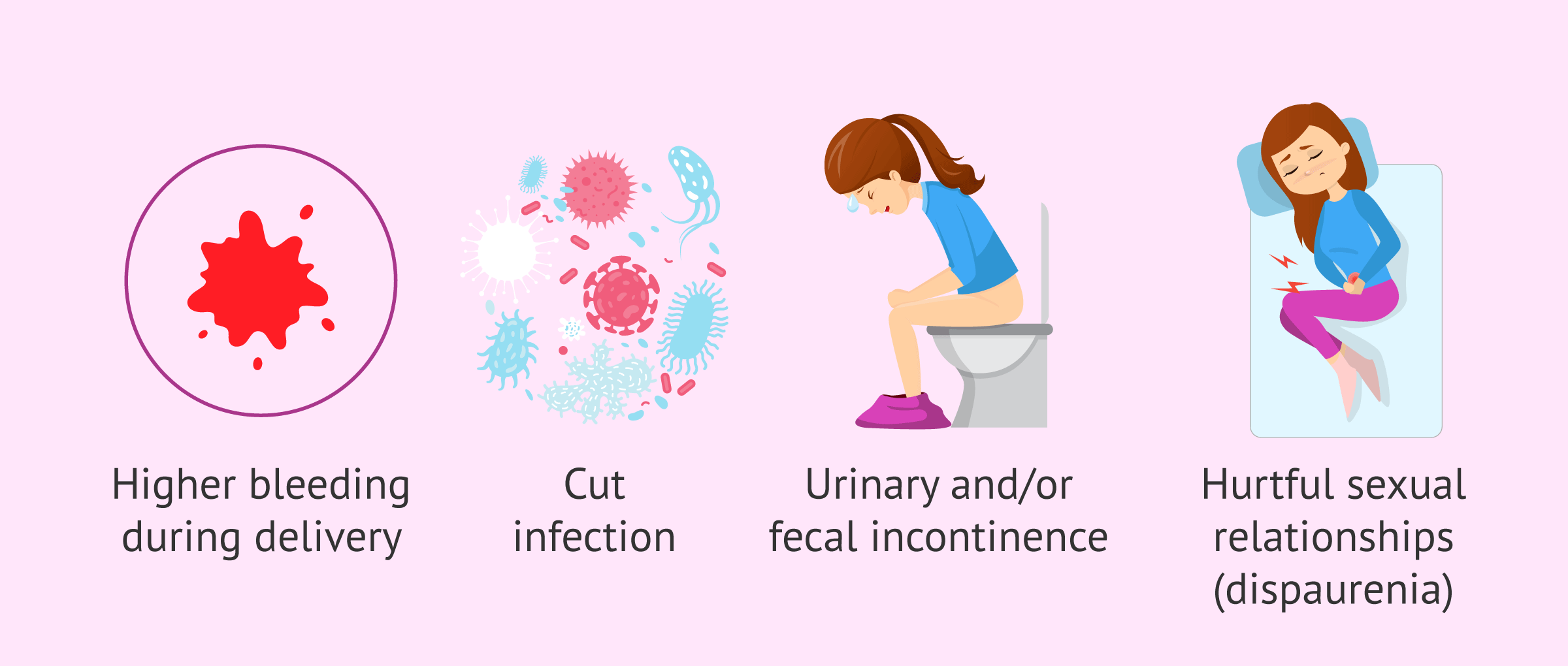
In addition to all this, the possible risks that may arise from this practice are the following:
- Increased bleeding during childbirth
- Infection of the cut and stitches
- Edemas and hematomas
- Fourth-degree tears
- Total or partial urinary and/or fecal incontinence
- Painful or uncomfortable scarring from stitches
- Scar endometriosis and tissue adhesion
- Painful intercourse (dyspareunia)
- Injuries to the fetus with the scalpel or scissors
Postpartum care
To avoid these complications and achieve adequate healing of the episiotomy, it is advisable to follow a series of daily care from day one:
- Maintain a daily hygiene, but always trying to make the genital area as dry as possible.
- Wash the genital area in the shower with neutral pH soap and water. Avoid baths.
- Dry the wound by tapping and avoiding dragging so as not to take any stitches.
- Clean the genital area well after urination and/or defecation, especially if the wound is recent.
- If the pain is severe, the woman can take some pain medicine such as acetaminophen or ibruprofen.
- Wear cotton underwear and avoid tight-fitting garments.
- It is advisable to sit on a cushion to be more comfortable, but not on a float, as it can open the points.
- Follow a diet rich in fiber to facilitate intestinal transit and avoid constipation.
- Use cotton compresses that perspire well and avoid using tampons, at least in the first six weeks after the episiotomy.
- The use of betadine is not recommended.
- Avoid sexual intercourse until the wound is well healed.

Finally, it is recommended that the woman visit a physiotherapist specializing in pelvic floor to have an assessment after postpartum and, if necessary, Kegel exercises and / or hypopressive gymnastics to help recovery.
FAQs from users
What risks or complications could episiotomy involve?
An episiotomy is a minor surgery that may result in the following complications:
- Enlargement of the cut, into the vagina including the anus- rectum.
- Bleeding or bruising.
- Infection, due to the fact that many bacteria live in the genital area.
- Edema.
- Painful cicatrization: the points that are applied for the closure "pull" and bother the patient.
- Dyspareunia: pain during sexual intercourse time after complete healing.
When is sexual intercourse possible after episiotomy?
It is essential not to have sex before the wound left by the cut has healed completely, as this could cause tearing of the area. In addition, the stitches must be completely reabsorbed, as this will prevent possible infections.
The recovery from the episiotomy is usually between four and six weeks, so after this period, there is no need for problems in sexual relations. In any case, it is important to follow the doctor's instructions.
How should I cure episiotomy?
After a vaginal delivery with episiotomy, it is very important that the woman follow all the recommendations of the medical specialist to heal the wound and that it heals properly.
Generally, the woman should maintain daily hygiene and wash the wound with soap and water. For drying, it is advisable to use a towel only for this area and not to drag. The wound should be kept as dry as possible and be in the air, although always when the woman is inside the house.
You can find more episiotomy care recommendations in this article
What are the advantages and disadvantages of episiotomy?
The main benefit of episiotomy is to facilitate the delivery of the baby, especially if there is a risk of tearing or signs of fetal distress.
However, this incision sometimes has many more drawbacks than advantages, so it should not be made in a generalized manner. In particular, episiotomy can cause a lot of pain when defecating or having sex if it does not heal properly. It can also cause bleeding, urinary and/or fecal incontinence, etc.
Are sexual intercourse painful after an episiotomy?
Yes, due to alterations in the healing process. For this reason, it is recommended to follow proper care immediately after the episiotomy, as well as to perform zig-zag massages on both sides of the scar, among other measures.
Suggested for you
One of the indications for episiotomy is to avoid a tear in the third stage of labour. If you want to know what this is all about, you can read on here: Perineal lesions during childbirth
On the other hand, if you want to continue to be informed about childbirth, how it unfolds and what it may entail, we recommend you access the following article: Childbirth: preparation, types and possible complications
We make a great effort to provide you with the highest quality information.
🙏 Please share this article if you liked it. 💜💜 You help us continue!
References
Aasheim V, Nilsen ABV, Reinar LM, Lukasse M. Perineal techniques during the second stage of labour for reducing perineal trauma. Cochrane Database Syst Rev. 2017 Jun 13;6:CD006672 (View)
ACOG Practice Bulletin No. 198 Summary: Prevention and Management of Obstetric Lacerations at Vaginal Delivery. Obstet Gynecol. 2018 Sep;132(3):795-797
Frenette P, Crawford S, Schulz J, Ospina MB. Impact of Episiotomy During Operative Vaginal Delivery on Obstetrical Anal Sphincter Injuries. J Obstet Gynaecol Can. 2019 Apr 16. pii: S1701-2163(19)30091-X (View)
Guillermo Carroli, Luciano Mignini. Episiotomy for vaginal birth. Cochrane Database Syst Rev. 2009 Jan 21;(1):CD000081.
Mário Dias Corrêa Junior, Renato Passini Júnior. Selective Episiotomy: Indications, Techinique, and Association with Severe Perineal Lacerations. Rev Bras Ginecol Obstet. 2016 Jun;38(6):301-7. doi: 10.1055/s-0036-1584942 (View)
Perineal Massage in Pregnancy. J Midwifery Womens Health. 2016 Jan-Feb;61(1):143-4 (View)