Azoospermia is defined as the total absence of sperm in the ejaculated semen. Thus, in order to diagnose this sperm disorder, it is necessary to examine the semen sample collected after ejaculation. This study is called semen analysis or seminogram and is the basic test for evaluating male fertility.
Other additional tests such as a hormone analysis, physical exploration and testicular biopsy can be performed in order to determine the type of azoospermia.
Provided below is an index with the 9 points we are going to expand on in this article.
- 1.
- 1.1.
- 2.
- 3.
- 4.
- 5.
- 5.1.
- 5.2.
- 5.3.
- 5.4.
- 5.5.
- 5.6.
- 6.
- 7.
- 8.
- 9.
Semen analysis
A semen analysis (SA) is a test used to examine a semen sample, both macroscopically (color, viscosity, pH...) or microscopically (concentration, motility, morphology...).
In order to render an accurate diagnosis of azoospermia and prevent analytic errors, the World Health Organization (WHO) recommends two semen analysis with a time gap of 2-3 months between each other.
Semen samples are obtained through masturbation after a period of sexual abstinence of between 3 to 5 days approximately. The sample must be collected under the appropriate hygienic conditions in order to avoid interferences with the outcomes and make the analysis easier for specialists.

If you want to read in-depth information about this test, you can visit the following article: What is a basic semen analysis and how is it done step by step?
To evaluate the quantity of spermatozoa in the ejaculate.
To examine the sperm count, the sample is assesses under the microscope using a tool called Makler chamber, although there exists another chamber for counting sperm: the Neubauer chamber. The steps followed with both tools is quite similar, so the choice is up to each clinic.

If the sperm count is zero after the microscopic analysis, the diagnosis is azoospermia. If, on the contrary, few sperms are observed, it is not a case of azoospermia, but a case of oligospermia or oligozoospermia.
Considering seeing a fertility specialist? Don't forget that, in the field of Reproductive Medicine, as in any other medical area, it is crucial that patients rely on the doctors and staff that will help them through their treatment cycle. Logically, conditions vary from clinic to clinic. For this reason, we recommend that you generate your Fertility Report now. It will offer you a list of clinics that have passed our rigorous selection process successfully. Furthermore, the system will make a comparison between the fees and conditions of each clinic so that you can make a better-informed decision.
If the diagnosis of azoospermia is clear, the patient is asked to wait for 2 to 3 months and then the SA is repeated. Specialists do this to make sure that the absence of sperm is not due to factors like stress, unhealthy diet, medication intake, fever, etc.
Should the result of a second SA be zero sperm count as well, the diagnosis of azoospermia can be considered correct. Afterwards, performing other tests such as a testicular biopsy to determine the cause of azoospermia is strongly recommended.
Hormonal analysis
Spermatogenesis or sperm production is regulated by hormones testosterone and FSH (follicle-stimulating hormone). Endocrine disorders affect the levels of these hormones and subsequently spermatogenesis, resulting in the absence of sperm cells in the semen after ejaculation.
Thus, assessing the levels of FSH and testosterone can help us obtain a more accurate diagnosis of azoospermia:
- FSH
- It is produced by the pituitary gland and is responsible of regulating sperm production in the testes. Too elevated FSH levels indicate that the amount of stem cells in the testicle (spermatogonia) is too low, causing the sperm count to be low or non-existent. For this reason, it is common for azoospermic males to have too high FSH levels.
- Testosterone
- This hormone, which is produced by the testis, follows the opposite pattern than FSH. If spermatogenesis doesn't take place, azoospermic males have lower-than-usual testosterone levels.
Simply put, if a hormone analysis shows elevated FSH levels and too low testosterone levels, it is likely that the patient suffers from secretory azoospermia. This means that zero sperm count is due to a lack of sperm production. In other words, it is due to spermatogenesis failure.
If a sperm analysis shows normal hormone levels, the chances are that azoospermia is due to an ejaculatory duct obstruction (EOD), that is, a blockage in the seminal ducts that transport sperm from the testis, where they are produced, to the outside.
Broadly speaking, obstructions typically appear in the epididymis or the vasa deferentia. This type of azoospermia is known as obstructive azoospermia.
Physical exploration
It is recommended that a specialist examines the male reproductive tract while is lying horizontally with the face and torso facing up (supine position) as well as standing up. Moreover, it is important that the room where the exploration is carried out is at an adequate temperature, as cold can cause the layers of the scrotum to contract, making the testicular examination more complicated.
Sometimes, a simple palpation can lead the specialist to think that there may exist some kind of abnormality with spermatogenesis, although rendering a final diagnosis is possible only when the results of the remaining tests are available.
During a physical exploration of male genitalia, your doctor will look for the presence of a varicocele, sexual development, size and testicular position, etc.
Testicular biopsy
Another useful diagnostic test is testicular biopsy. This surgical procedure is simple and involves removing small fragments of the testicle. Then, they are examined in the lab in order to find sperm.
The fragments of testis are examined microscopically. If sperm are found, secretory azoospermia can be dismissed: as long as sperm are found in the testicle, it means that it is capable of producing them.
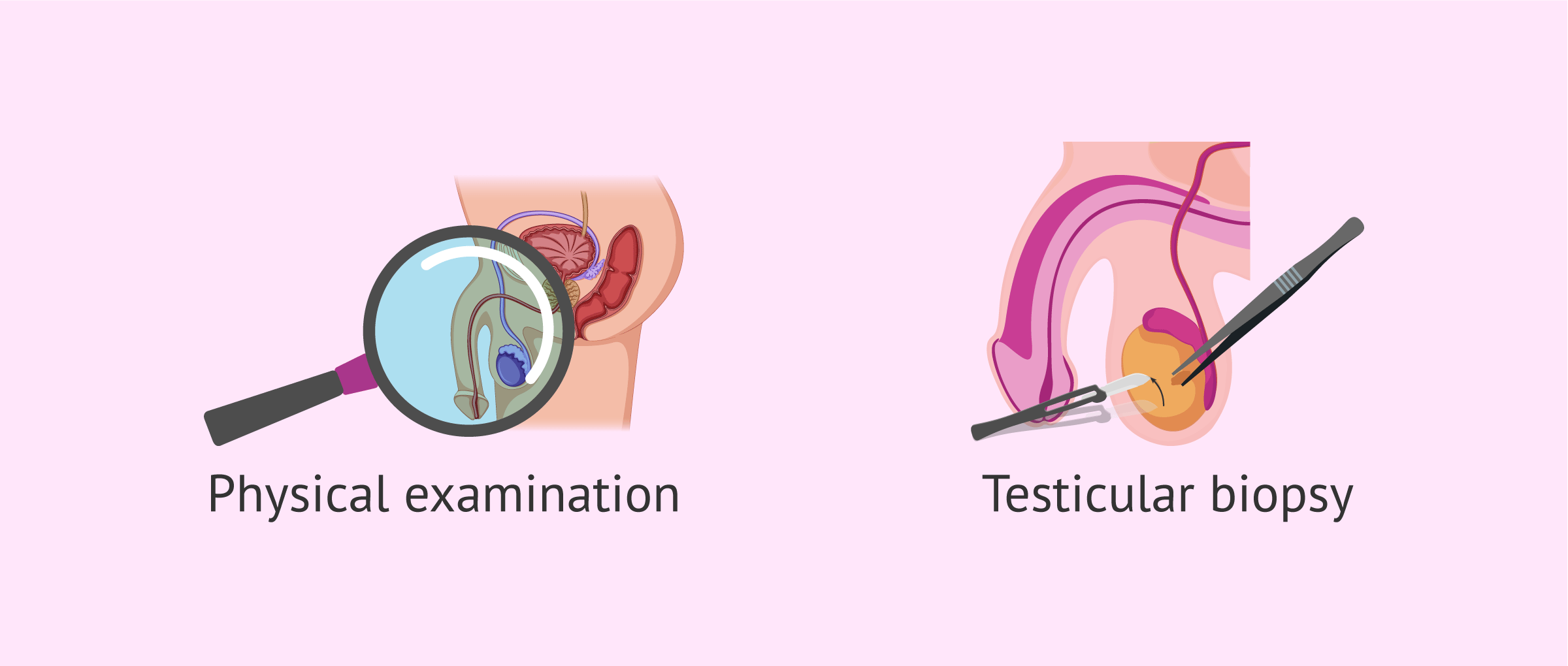
If the sperm found are live, in spite of having low motility, they can be used for Intracytoplasmic Sperm Injection (ICSI), Thus, a testicular biopsy is both a diagnostic test (it helps to confirm a diagnosis of secretory azoospermia) and a treatment (sperm collection for ICSI).
FAQs from users
Are both types of azoospermia diagnosed using the same methods?
Yes, the tests used are the same. In addition to a semen analysis, which indicates the absence of sperm, your doctor may carry out an exploration of your genitalia to verify if there's activity in the testicles.
Also, a hormone check is use to check if it is a case of secretory or obstructive azoospermia.
Another test that can be helpful is a testicular biopsy, which can tell us whether there's sperm production or not.
What tests can diagnose azoospermia?
Azoospermia is defined as the absence of spermatozoa in the ejaculate. The testicle is the organ that produces spermatozoa after they are transported and stored in the seminal vesicle, a contiguous organ in intimate relationship with the prostate. Azoospermia may be due to a lack of production by the testicle or to an obstruction during its transport to the seminal vesicle.
Thus, the basic study for the diagnosis of azoospermia consists of a spermogram and a testicular biopsy.
Is a testicular biopsy painful?
No, it is a surgical procedure that is performed using anesthesia, which prevents pain for the patient. However, it is likely that you feel mild discomfort in the testicular area.
What type of azoospermia does a man with high FSH have?
An elevated FSH in males with absent sperm indicates that the type of azoospermia is secretory. Most likely the stem cell population in the testis has been destroyed by some treatment such as radiation therapy and therefore FSH is not assimilated to carry out its function.
How long does it take for an azoospermia diagnosis to be rendered?
As explained earlier, to get a correct diagnosis of azoospermia, doing at least two semen analysis at different time periods is different. The results of a semen analysis are available within two weeks on average, although it depends on the clinic or center where it is done.
If you undergo other tests such as a testicular biopsy, it make take longer.
My first semen analysis says azoospermia and the second says oligospermia, is it normal?
Yes, it is. For example, it can happen that a particular circumstance in your life (like too high stress levels) caused azoospermia in the first analysis due to changes in hormone levels. However, after another semen analysis (done 4 months after), if the special circumstance has disappeared, it is likely that your hormones have returned to normal levels, and subsequently sperm production is normal again.
Suggested for you
To sum up, throughout this article we have seen the different diagnostic methods used to check if a male has obstructive or non-obstructive azoospermia. To learn the differences between them, click here:
Also, once a patient has obtained a conclusive diagnosis, the best treatment option will be recommended. Learn about the different options available here: Treatment of Azoospermia.
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Cerilli LA, Kuang W, Rogers D. A practical approach to testicular biopsy interpretation for male infertility. Arch Pathol Lab Med. 2010 Aug;134(8):1197-204 (View)
Dohle GR, Elzanaty S, van Casteren NJ. Testicular biopsy: clinical practice and interpretation. Asian J Androl. 2012 Jan;14(1):88-93 (View)
Esteves SC. Clinical management of infertile men with nonobstructive azoospermia. Asian J Androl. 2015 May-Jun;17(3):459-70 (View)
Hessel ML, Ramos L, D'Hauwers KW, Braat DD, Hulsbergen-van de Kaa CA. Beneficial value of testicular sperm extraction-AgarCyto in addition to the standard testicular biopsy for diagnosis of testicular germ cell tumors in nonobstructive azoospermia. Fertil Steril. 2016 Feb;105(2):308-14.e1 (View)
Sigman M, Zini A. (2009). Semen analysis and sperm function assays: what do they mean? Semin Reprod Med; 27: 115-123 (View)
World Health Organization (WHO) (2010). WHO laboratory Manual for the examination of human semen and sperm-cervical mucus interaction. Cambridge Academic Press (View)
FAQs from users: 'Are both types of azoospermia diagnosed using the same methods?', 'What tests can diagnose azoospermia?', 'Is a testicular biopsy painful?', 'What type of azoospermia does a man with high FSH have?', 'How long does it take for an azoospermia diagnosis to be rendered?' and 'My first semen analysis says azoospermia and the second says oligospermia, is it normal?'.






Dear Doctor,
I have azoospermia and my blood report shows a normal testosterone level. The first blood test which I did in the middle of the afternoon showed FSH levels of 6 IU/L which was deemed normal and LH level 4 IU/L, however the second time I did the test in the morning and fasting, it showed a mildly high FSH level. From your opinion what type of azoospermia am I likely to have.
This will be confirmed by a biopsy I know but just if you could tell me your opinion.
Kind regards,
Taz
Sir, i have done a testicular biopsy but sperm was found abnormal (head large, tail long, etc). What can I do???
Dear Mahesh,
When sperm is found morphologically abnormal, the condition is known as “teratospermia” or “teratozoospermia”. You can find detailed info about this sperm pathology here: What Is Teratozoospermia?
I hope this helps,
Best