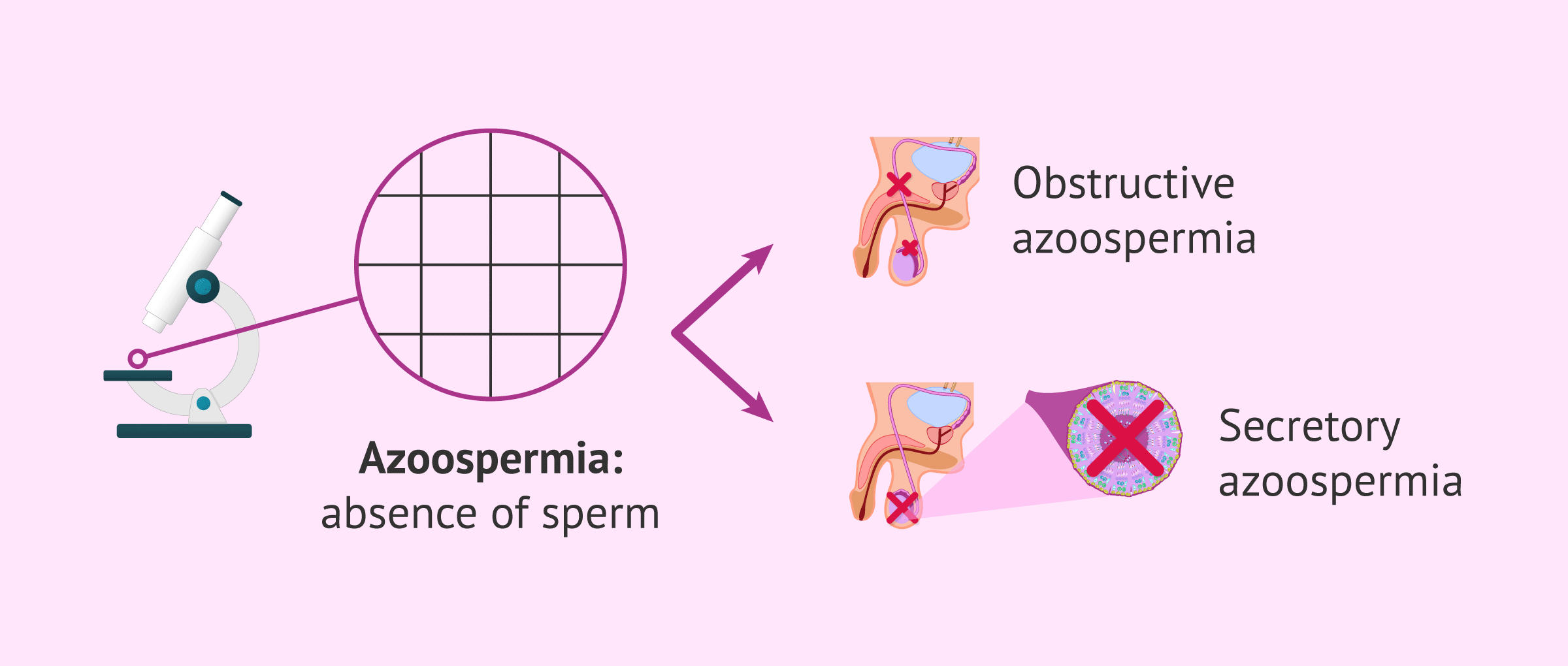
Azoospermia is defined as the total absence of sperm in the ejaculate after a routine microscopic analysis or seminogram (semen analysis).
A natural pregnancy in a woman whose partner has secretory or obstructive azoospermia is not possible because there will be no sperm in the ejaculate. However, when the applied treatments do not resolve the problem, assisted reproduction offers a series of options that allow achieving pregnancy through in vitro fertilization techniques.
Sperm retrieval in men with azoospermia will be performed through a testicular biopsy or sperm aspiration directly from the epididymis and testicle. When neither of these two options is possible, the last resort to achieve a pregnancy will be to use a sperm donor.
Provided below is an index with the 9 points we are going to expand on in this article.
- 1.
- 2.
- 2.1.
- 2.2.
- 2.3.
- 3.
- 4.
- 5.
- 5.1.
- 5.2.
- 5.3.
- 5.4.
- 5.5.
- 6.
- 7.
- 8.
- 9.
Classification of azoospermia
The andrological diagnosis systematically divides azoospermia into two main morphological categories, strictly depending on whether the failure lies in the production of sperm or in their transport to the outside:
- Obstructive azoospermia: it is characterized by presenting functional spermatogenesis inside the testicular seminiferous tubules, meaning there is sperm production. The main problem lies in a physical obstruction or anatomical defect in the seminal ducts, completely preventing the cells from exiting to the outside during ejaculation.
- Secretory (or non-obstructive) azoospermia: the testicular tissue itself presents an intrinsic cellular failure that partially or totally stops the division and formation of male gametes, causing them not to develop and, consequently, not to reach the seminal fluid.
Determining the type of azoospermia the patient suffers from defines the reproductive prognosis and the chances of recovering good quality sperm. To obtain sperm in these situations, there are different procedures detailed below.
Sperm aspiration
Obstructive azoospermia is characterized by an obstruction in the vas deferens, the tubes that communicate the testicle with the exterior. Men diagnosed with obstructive azoospermia do not expel sperm in the ejaculate, but there is sperm production in the testicle.
One of the options is to extract sperm directly from the testicle or epididymis, although little sperm will be obtained. There are several ways to perform sperm extraction and their names come from the acronyms: MESA, PESA and TESA.

ICSI is the ideal IVF procedure because only one sperm is needed for each egg to be fertilized. In addition, it does not require that the spermatozoa have good mobility, since it is the embryologist himself who introduces the spermatozoa into the egg.
MESA
Microsurgical Epididymal Sperm Aspiration (MESA) is used in patients with a blockage in the reproductive tract. Through MESA, a small incision in the epididymis is done to retrieve sperm directly from it.

MESA is a technically challenging procedure, and therefore the costs are elevated. For this reason, although it allows for a greater number of sperm to be collected in comparison to PESA, it is rarely the technique of choice.
PESA
Percutaneous Epididymal Sperm Aspiration (PESA) is less technically challenging and invasive than MESA. Furthermore, the expertise required is not as demanding. It is done under sedation.

A needle attached to a syringe is inserted through the scrotal skin into the epididymis. The main pitfall of PESA is that needle insertion is done blindly. Thus, even though it is not so common, it might happen that no sperm cell is found.
TESA
Testicular Sperm Aspiration (TESA) is done percutaneously as well, as in the case of PESA. The difference between TESA and PESA is that the former is done in the testes instead of the epididymis.

TESA is the option of choice when none of the above are successful (MESA and PESA), and in cases where the problem is related to an absent or blocked epididymis.
Testicular biopsy
Testicular biopsy, also called Testicular Sperm Extraction (TESE), is done using a local anesthetic and involves the following steps:
- Using a scalpel, the specialist opens the different testicular layers until he or she reaches the testicle, where small pieces will be retrieved. On average, between 2 to 3 cm of testicular layers are opened, which will be closed with one or two points of a suture.
- Once the biopsy is done or simultaneously, the tissue retrieved is examined microscopically to find spermatozoa, which will be used later for ICSI technique.

Although it is indicated for patients with obstructive azoospermia, it can be used in cases of non-obstructive azoospermia as well. In many cases, even if no sperm are produced in the testicles, still sources of spermatogenesis could be found. In other words, if the search is done thoroughly, sooner or later sperm are found.
In any case, the chances of achieving a pregnancy with ICSI with the sperm or few sperms found after a testicular biopsy in patients with non-obstructive azoospermia are low.
One should not forget that a testicular biopsy is not only the option of choice to achieve pregnancy, but also a diagnostic test that allows us to distinguish between non-obstructive and obstructive azoospermia.
Sperm donation
The procedures mentioned above can be effective in cases of obstructive azoospermia but are useless in males with non-obstructive/secretory azoospermia. In the latter group, if spermatogenesis is not recovered with different treatment options, using donor sperm recommended.
It involves doing an Intrauterine Insemination (IUI) or In Vitro Fertilization (IVF) with sperm donated by a young, healthy man. Sperm donors are medically and psychologically pre-screened to verify their state of health and confirm that their sample is in optimum conditions for being used.
Choosing between IUI or IVF depends on the characteristics of the female partner, including age, tubal patency, etc.
The success rates with donor sperm are considerably high. However, on the other side of the coin, it presents a major disadvantage: the intended father will not share his DNA with the child. Children conceived with donor sperm inherit the genetic material of the donor.
Do you need donor sperm for your fertility treatment cycle? Then we recommend that you get your Fertility Report now to find the most suitable clinic for you. Our thorough selection criteria when it comes to recommending clinics plus your particular needs equal the best fertility center for you. You will receive in your inbox a detailed report with the clinics that we recommend for your particular treatment, as well as the conditions that they offer for each program.
FAQs from users
Is it possible to be a father with secretory azoospermia?
Yes, it is possible. Secretory azoospermia is the absence of spermatozoa in the ejaculate. When we refer to secretory azoospermia it is when this absence is due to the lack of sperm production in the testicles (spermatogenesis). This sperm alteration can be reversible or irreversible.
In the case of obstruction of the vas deferens it is possible to recover spermatozoa by testicular biopsy so that the male germ cells can be rescued and an ICSI (Intracytoplasmic Sperm Injection) can be performed.
Is sperm donation the only option to have children if husband has non-obstructive azoospermia?
If it is a case of untreatable or irreversible non-obstructive/secretory azoospermia, then the answer is yes.
In the most severe cases of non-obstructive azoospermia, obtaining viable sperm is highly unlikely. For this reason, the only option to have children with this sperm disorder is sperm donation.
Is it biologically possible to achieve a natural pregnancy with azoospermia?
No. Spontaneous gestation in a natural way is not viable in cases of azoospermia since there are no sperm in the ejaculate.
For natural fertilization to occur, the arrival of a minimum volume of motile sperm to the fallopian tubes to fertilize the egg is essential. If there are no sperm in the ejaculate, the encounter with the egg for its fertilization cannot take place.
Can sperm be found with a testicular biopsy if husband had a vasectomy 11 years ago?
A testicular biopsy (Testicular Sperm Extraction or TESE) allows for sperm to be directly collected from the testicle, where sperm production takes place. However, after such a long period of time with a voluntary obstruction, it is likely that the organism has decreased the number of sperm it produces. The good news is that, since ICSI technique could work with just a single sperm, a woman could get pregnant with only few sperm retrieved after TESE.
In any case, one should bear in mind that it is possible that zero sperm are found in the sample after a testicular biopsy.
Is sperm aspiration possible after vasectomy to achieve pregnancy?
Yes, it is possible to retrieve sperm by aspiration of the epididymis or testicle after vasectomy. However, it may happen that no sperm are obtained.
Therefore, it is usually recommended to freeze a semen sample before undergoing this method of male sterilization. The frozen semen sample can then be used in the future if gestation is desired through artificial insemination (AI) or in vitro fertilization (IVF).
Suggested for you
Throughout this article, we have read about the options an azoospermic man has to conceive in spite of this sperm disorder. Want to learn more about the different treatment options available? Click here: Treatment of Azoospermia.
On the other hand, we have made several references to testicular biopsy as a diagnostic test to detecting azoospermia. To learn more about the diagnostic tests used before rendering a diagnosis of azoospermia, read: How Is Azoospermia Diagnosed?
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Bernie AM, Mata DA, Ramasamy R, Schlegel PN. Comparison of microdissection testicular sperm extraction, conventional testicular sperm extraction, and testicular sperm aspiration for nonobstructive azoospermia: a systematic review and meta-analysis. Fertil Steril. 2015 Nov;104(5):1099-103.e1-3 (View)
Deruyver Y, Vanderschueren D, Van der Aa F.Outcome of microdissection TESE compared with conventional TESE in non-obstructive azoospermia: a systematic review. Andrology. 2014 Jan;2(1):20-4 (View)
Dineen T, Waterstone J, Cullen I. Non-Obstructive Azoospermia and the Impact of MicroTESE. Ir Med J. 2016 Sep 9;109(8):447 (View)
Dohle GR, Elzanaty S, van Casteren NJ. Testicular biopsy: clinical practice and interpretation. Asian J Androl. 2012 Jan;14(1):88-93 (View)
Faure A, Bouty A, O'Brien M, Thorup J, Hutson J, Heloury Y. Testicular biopsy in prepubertal boys: a worthwhile minor surgical procedure? Nat Rev Urol. 2016 Mar;13(3):141-50 (View)
Franco G, Scarselli F, Casciani V, De Nunzio C, Dente D, Leonardo C, Greco PF, Greco A, Minasi MG, Greco E. A novel stepwise micro-TESE approach in non obstructive azoospermia. BMC Urol. 2016 May 12;16(1):20 (View)
Hao L, Li ZG, He HG, Zhang ZG, Zhang JJ, Dong Y, Li ZB, Han CH. Application of percutaneous epididymal sperm aspiration in azoospermia. Eur Rev Med Pharmacol Sci. 2017 Mar;21(5):1032-1035 (View)
Morita T, Komatsubara M, Kameda T, Morikawa A, Kubo T, Fujisaki A, Kurokawa S, Kawata H, Tanaka A. A new simple technique of epididymal sperm collection for obstructive azoospermia. Asian J Androl. 2016 Jan-Feb;18(1):149-50 (View)
Văduva CC, Constantinescu C, Radu MM, Văduva AR, Pănuş A, Ţenovici M, DiŢescu D, Albu DF. Pregnancy resulting from IMSI after testicular biopsy in a patient with obstructive azoospermia. Rom J Morphol Embryol. 2016;57(2 Suppl):879-883 (View)
van Wely M, Barbey N, Meissner A, Repping S, Silber SJ. Live birth rates after MESA or TESE in men with obstructive azoospermia: is there a difference? Hum Reprod. 2015 Apr;30(4):761-6 (View)
Vloeberghs V, Verheyen G, Haentjens P, Goossens A, Polyzos NP, Tournaye H. How successful is TESE-ICSI in couples with non-obstructive azoospermia? Hum Reprod. 2015 Aug;30(8):1790-6 (View)
FAQs from users: 'Is pregnancy with azoospermia possible?', 'Is it possible to be a father with secretory azoospermia?', 'Is sperm donation the only option to have children if husband has non-obstructive azoospermia?', 'Is it biologically possible to achieve a natural pregnancy with azoospermia?', 'Can sperm be found with a testicular biopsy if husband had a vasectomy 11 years ago?' and 'Is sperm aspiration possible after vasectomy to achieve pregnancy?'.
Authors and contributors




