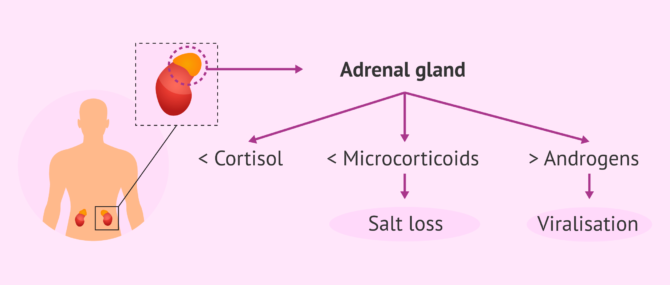
Congenital adrenal hyperplasia or CAH is a group of disorders of the adrenal glands, glands located on top of the kidneys that produce steroid hormones such as testosterone and sex hormones such as cortisol and aldosterone.
This pathology causes an imbalance in the amount of hormones produced by the body, causing a decrease in cortisol and aldosterone levels, as well as an increase in androgens.
Cortisol levels in people with CAH are decreased, which causes an increase in the hormone ACTH. As a consequence, adrenal androgen secretion is increased and gonadotropin secretion is inhibited. For this reason, women with CAH may have fertility problems in adulthood.
Provided below is an index with the 9 points we are going to expand on in this article.
- 1.
- 1.1.
- 2.
- 3.
- 4.
- 5.
- 5.1.
- 5.2.
- 5.3.
- 6.
- 7.
- 8.
- 9.
What is congenital adrenal hyperplasia?
Congenital adrenal hyperplasia (CAH) is a disease of genetic origin and autosomal recessive inheritance that can occur in both girls and boys. It is an involvement of the adrenal glands, which are responsible for the production of cortisol, mineralocorticoids and androgens.
CAH can have different forms and degrees of severity. In all cases, early detection is essential for a better management of the disease. There are two main types of congenital adrenal hyperplasia:
- Classic form
- is the least frequent and most severe. The classic form of adrenal hyperplasia is usually detected at birth and involves complete deficiency of hormone synthesis regulatory enzymes.
- Classic form
- this is the most common type of adrenal hyperplasia and is less severe than the classic form, since the enzymatic deficit is not total but partial.
However, adrenal hyperplasia can also be classified according to the type of enzyme deficit that occurs. In this case, up to 7 clinical forms of CAH could be distinguished, the most common being 21-hydroxylase deficiency. About 90-95% of cases of adrenal hyperplasia are of this type and it is caused by mutation of the CYP21A2 gene located on chromosome 6.
What are the symptoms of CAH?
Girls with congenital adrenal hyperplasia suffer masculinization of their genitalia. There are internal female reproductive organs such as the uterus, fallopian tubes and ovaries, but they show an ambiguous shape and it is complicated to identify the gender.
As the years go by, other types of signs appear, such as the appearance of hair at an early age and in greater quantity than normal. There is also a worsening of the voice and imbalances in menstruation or amenorrhea.

In children, HSCO is not as easily detected at birth. However, symptoms appear as time goes by that could be indicative of this disease. Some of the clinical manifestations of CSH in children are penile enlargement that does not correspond to the size of the small testicles or early hair appearance.
Another of the most evident symptoms when diagnosing the disease is the loss of sodium in the urine, especially during the first months of life. This decrease in sodium levels leads to other problems such as dehydration, vomiting or even cardiac arrhythmias. All this can lead to what is known as adrenal insufficiency adrenal insufficiency.
Diagnosis of adrenal hyperplasia
The way to diagnose congenital adrenal hyperplasia is by evaluating the levels of progesterone, aldosterone, cortisol and sodium in both blood and urine. In addition, a bone x-ray is recommended. Since adrenal hyperplasia has a genetic origin, it would also be necessary to perform various genetic tests.

In congenital adrenal hyperplasia, prenatal diagnosis is of vital importance, especially if there is a history of congenital adrenal hyperplasia. This prenatal diagnosis will be performed by chorionic villus sampling, a non-invasive method performed in the first trimester of pregnancy. In the newborn, it can be detected by heel prick.
is there a treatment for CAH?
Congenital adrenal hyperplasia has no cure, but there are different forms of treatment so that patients can lead a normal life. Each of the therapeutic options is detailed below:
- Glucocorticoid replacement therapy
- is the most common treatment for congenital adrenal hyperplasia due to 21-hydroxylase deficiency. Glucocorticoids block ACTH (corticotrophin-stimulating hormone) secretion and decrease the amount of sex steroids.
- Mineralocorticoid replacement therapy
- used in patients with saline leakage. Normally, 9-α-fluorhydrocortisone supplemented with sodium chloride is used as a mineralocorticoid.
- Surgical treatment
- in the case of girls, surgery may be necessary to correct and repair genital function.

It should be noted that any type of treatment is performed under medical prescription. In addition, psychological support is sometimes necessary to improve the child's emotional health.
Congenital adrenal hyperplasia and fertility
When a deficit of the enzyme 21 hydroxylase occurs, there is an increase in adrenal androgens, which causes a decrease in the secretion of GnRH hormone.
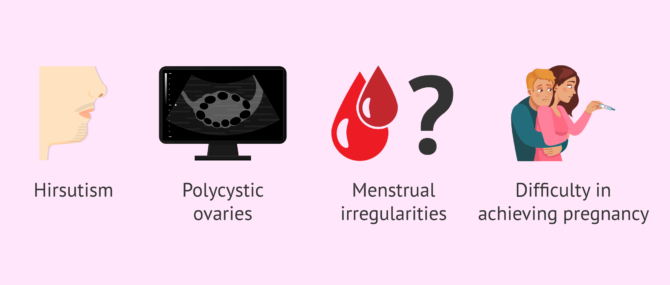
Women with CAH often have hirsutism, polycystic ovaries, menstrual irregularities and, therefore, difficulty becoming pregnant. However, fertility problems are greater in women with classical form of CAH. In contrast, men with congenital adrenal hyperplasia usually have normal fertility. Their gonadal axis is less affected compared to women with CAH.
In the case of males with classical forms of CAH, testicular nodules may appear, which could hinder their reproductive capacity. These nodules could compress the seminiferous tubules and, therefore, sperm production would not be possible.
In any case, if there is a diagnosis of congenital adrenal hyperplasia and you want to have a baby, it is vitally important to see a specialist doctor.
FAQs from users
Can congenital adrenal hyperplasia be prevented?
There is no way to prevent congenital adrenal hyperplasia (CAH). However, if parents are aware of risk factors for CAH or have a family history of CAH, it is best to seek genetic counseling before seeking pregnancy.
How should one proceed if a woman with CAH becomes pregnant and it is a girl?
When a woman with congenital adrenal hyperplasia (CAH) becomes pregnant, she should follow all of her physician's instructions. Most commonly, a chorionic villus biopsy is performed in the 10th week of pregnancy or an amniocentesis in the 16th week to evaluate for mutations of the gene that causes CAH.
If the fetus is affected and is female, then the woman should be treated with dexamethasone throughout the pregnancy. On the other hand, this treatment would not be indicated if the fetus is male or if the fetus is female but does not have the mutation.
What is cryptic congenital adrenal hyperplasia?
This is an asymptomatic form of congenital adrenal hyperplasia (CAH), i.e. it does not cause clinical manifestations. The only way to detect cryptic CAH is by hormone testing and comparing hormone levels with those of patients with symptomatic CAH.
Suggested for you
If you are interested in the baby's development, then we invite you to continue reading here: How is the baby's development month by month - Special care.
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Alessandro Prete, Richard J Auchus, Richard J Ross. Clinical advances in the pharmacotherapy of congenital adrenal hyperplasia. Eur J Endocrinol. 2021 Nov 30;186(1):R1-R14. doi: 10.1530/EJE-21-0794 (View)
Ashwini Mallappa, Deborah P Merke. Management challenges and therapeutic advances in congenital adrenal hyperplasia. Nat Rev Endocrinol. 2022 Jun;18(6):337-352. doi: 10.1038/s41574-022-00655-w (View)
Hedi L Claahsen-van der Grinten, Phyllis W Speiser, S Faisal Ahmed, Wiebke Arlt, Richard J Auchus, Henrik Falhammar, Christa E Flück, Leonardo Guasti, Angela Huebner, Barbara B M Kortmann, Nils Krone, Deborah P Merke, Walter L Miller, Anna Nordenström, Nicole Reisch, David E Sandberg, Nike M M L Stikkelbroeck, Philippe Touraine, Agustini Utari, Stefan A Wudy, Perrin C White. Congenital Adrenal Hyperplasia-Current Insights in Pathophysiology, Diagnostics, and Management. Endocr Rev. 2022 Jan 12;43(1):91-159. doi: 10.1210/endrev/bnab016 (View)
Ifeanyi I. Momodu, Brian Lee, Gurdeep Singh. Congenital Adrenal Hyperplasia. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan. 2023 Jan 1 (View)
Gianluca Cera, Pietro Locantore, Roberto Novizio, Ettore Maggio, Vittoria Ramunno, Andrea Corsello, Caterina Policola, Paola Concolino, Rosa Maria Paragliola, Alfredo Pontecorvi. Pregnancy and Prenatal Management of Congenital Adrenal Hyperplasia. J Clin Med. 2022 Oct 19;11(20):6156. doi: 10.3390/jcm11206156 (View)
Phyllis W Speiser, Wiebke Arlt, Richard J Auchus, Laurence S Baskin, Gerard S Conway, Deborah P Merke, Heino F L Meyer-Bahlburg, Walter L Miller, M Hassan Murad, Sharon E Oberfield, Perrin C White. Congenital Adrenal Hyperplasia Due to Steroid 21-Hydroxylase Deficiency: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2018 Nov 1;103(11):4043-4088 (View)
Smita Jha, Adina F Turcu. Nonclassic Congenital Adrenal Hyperplasia: What Do Endocrinologists Need to Know? Endocrinol Metab Clin North Am. 2021 Mar;50(1):151-165 (View)
Sze May Ng, Karolina M Stepien, Ashma Krishan. Glucocorticoid replacement regimens for treating congenital adrenal hyperplasia. Cochrane Database Syst Rev. 2020 Mar 19;3(3):CD012517 (View)
FAQs from users: 'Can congenital adrenal hyperplasia be prevented?', 'How should one proceed if a woman with CAH becomes pregnant and it is a girl?' and 'What is cryptic congenital adrenal hyperplasia?'.


