Polycystic Ovary Syndrome (PCOS) is a chronic disorder which treatment is based on achieving the following goals:
- To cure the infertility problems caused by it
- To reduce the side effects derived from hyperandrogenism
Given that there exists a wide range of symptoms associated with PCOS, there exist no particular therapy to treat this syndrome. Instead, the treatment to follow is dependent on the clinical signs each woman presents.
Provided below is an index with the 9 points we are going to expand on in this article.
- 1.
- 2.
- 3.
- 3.1.
- 3.2.
- 3.3.
- 3.4.
- 4.
- 4.1.
- 4.2.
- 5.
- 5.1.
- 5.2.
- 5.3.
- 5.4.
- 5.5.
- 6.
- 7.
- 8.
- 9.
Changing your habits
It is estimated that almost 50 percent of PCOS patients have overweight, that is, their Body Mass Index (BMI) is above 35. Obesity is not only a metabolic disorder, but it is scientifically proven that it affects the quantity and quality of the eggs the woman produces.
Due to all these reasons, if the woman has overweight in addition from PCOS, she is recommended to start a weight loss plan that includes the following measures:
- Exercise.
- Balanced diet.
- Pharmacological treatment.
- Bariatric surgery.
Bariatric surgery involves a set of surgical procedures to achieve weight loss in the patient. An example of bariatric surgery is a gastric bypass.
Losing weight can improve menstrual irregularities and other reproductive problems caused by PCOS. Moreover, it can reduce insulin resistance.

Obviously, in patients with normal weight, these tips are unnecessary. As a matter of fact, losing weight can even worsen the situation at the hormonal and metabolic levels.
Hormonal contraception
In women with PCOS, the pill is used to regulate menstrual cycles, prevent periods of amenorrhea, and treat hyperandrogenism.
Contraception is used only in women with PCOS who do not want to conceive yet, since the use of the pill means that periods are regulated, but at the same time pregnancy is prevented.

Another major advantage of the pill is that it reduces the risk of endometrial cancer, since it promotes endometrial shedding every 28 days. However, one should note that it is only effective while being taken. If a woman stops using the pill, menstrual cycles will be irregular again.
Ovulation Induction (OI)
The main infertility problem of women with PCOS is anovulation. Thus, in order for these patients to get pregnant, inducing ovulation artificially is required. To this end, the following fertility drugs are the most commonly ones used:
Clomiphene citrate
Clomiphene is the drug of choice when it comes to inducing ovulation in women with Polycystic Ovary Syndrome (PCOS). It is an effective, safe, easily-administered, and cheap medication.
It works by inhibiting the effect of the estrogens produced by the ovaries. By preventing this hormone from having an effect over the hypothalamus, it is unable to detect an increase in estradiol levels and continues producing GnRH (gonadotropin-releasing hormone). This, at the same time, causes it to continue producing FSH and LH. As a result, follicle growth increases.
Clomiphene citrate is administered by mouth route between the third and eighth day of menstruation. When follicle growth is adequate, ovulation is triggered with a dose of Ovitrelle, and intercourse is scheduled for the next 36 hours.
The side effects of this drug appear in less than 10% of the patients, and can include:
- Hot flashes.
- Visual disturbances.
- Nausea.
- Swollen breasts.

To avoid multiple pregnancies, it is essential to take this medication under medical prescription, as well as to perform constant ultrasound controls.
Letrozole
When treatment with clomiphene fails to cause ovulation, this type of drugs are used.
The goal of using Letrozole is the same as clomiphene, that is, increasing the levels of FSH and LH, the hormones responsible for follicle growth and maturation.
The mechanism of action of Letrozole is different, though. Instead of blocking the connection between estradiol and the hypothalamus, it blocks the estrogen-producing hormone. By doing this, the hypothalamus increases GnRH secretion after detecting that estrogen levels are insufficient. Again, FSH and LH levels increase.
The administration protocol of Letrozole is similar to that of clomiphene, since it is also administered orally during the first week of menstruation. Through ultrasound scan and bloodworks, follicle growth is monitored.

When the desired follicle size is achieved, ovulation is triggered and IUI or intercourse are scheduled for the next 36 hours.
Gonadotropins
Gonadotropins are the most recurrent treatment for PCOS patients in whom none of the above described treatments have worked.
As in the case of clomiphene citrate and Letrozole, the purpose of Gonadotropins is to increase FSH and LH levels to trigger follicle growth. Contrary to clomiphene and Letrozole, growth is achieved directly, as medications containing gonadotropins do not alter the mechanism or the production of estrogens.
Since PCOS patients have a greater amount of follicles in the ovaries, starting with low doses of gonadotropins is essential to prevent a multiple pregnancy and the risk of Ovarian Hyperstimulation Syndrome (OHSS).
As for the administration protocol, it is done in the form of daily subcutaneous injections from the 5th or 6th day of the menstrual period. When the specialist observes through ultrasound scan the presence of 1-3 ovarian follicles larger than 12 mm, ovulation is triggered with an Ovitrelle injection. Then, within 36 hours, IUI or intercourse is scheduled.
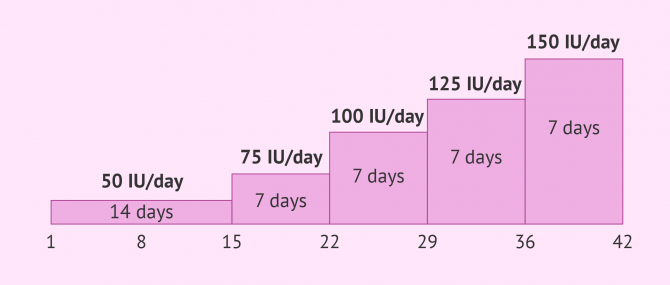
If ultrasound monitoring shows that follicle growth path is slower than normal, the dosage of gonadotropins can be increased until the desired follicle size is achieved.
Insulin-sensitizing drugs
Insulin resistance is highly associated with PCOS. This disorder, at the same time, causes the organism to release extra amounts of insulin, since it detects that normal insulin levels are insufficient. This condition is known as hyperinsulinemia.
Insulin-sensitizing drugs, like metformin, enhance the effect of this hormone by preventing hyperinsulinemia. When insulin levels in blood decrease, the levels of these hormones vary as well:
- Sex hormone binding globulin (SHBG)
- By increasing SHBG levels, the amount of free androgens decreases, which inhibits their effect. This prevents them from interfering in follicle development.
- Androgens
- Too elevated insulin levels increase the release of these male hormones in the ovary and the suprarrenal glands, which prevents follicle growth and maturation.
A decrease in androgen levels prevents other side effects of these hormones, such as hirsutism or acne.
Surgery
Treating PCOS by means of surgery is the least common option of all. It is the option of choice when none of the above mentioned treatment protocols work. Since it is an invasive procedure, it should be used in very specific cases.
There exist two types of surgical procedures to treat PCOS, which are typically carried out through laparoscopic surgery.
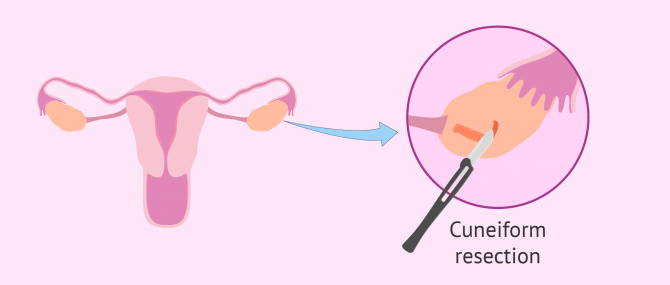
Cuneiform resection of the ovaries
With this surgical procedure, the surgeon removes part of the ovarian tissue to eliminate a large part of the tissue that produces male hormones. The goal is to reduce testosterone levels.
Within several days after surgery, hormone levels are normalized and the woman ovulates again.
Several days after surgery, these hormones are leveled off, allowing the woman to recover ovulation.
This surgical procedure can cause post-op ovarian adhesions due to the cuts performed during surgery. This can increase the risk of having blocked Fallopian tubes.
Although recovery is permanent in some cases, most of them have anovulatory cycles again after various months of regular cycles. A small group of women has no response to this treatment and are unable to reestablish ovulatory cycles.
Ovarian drilling
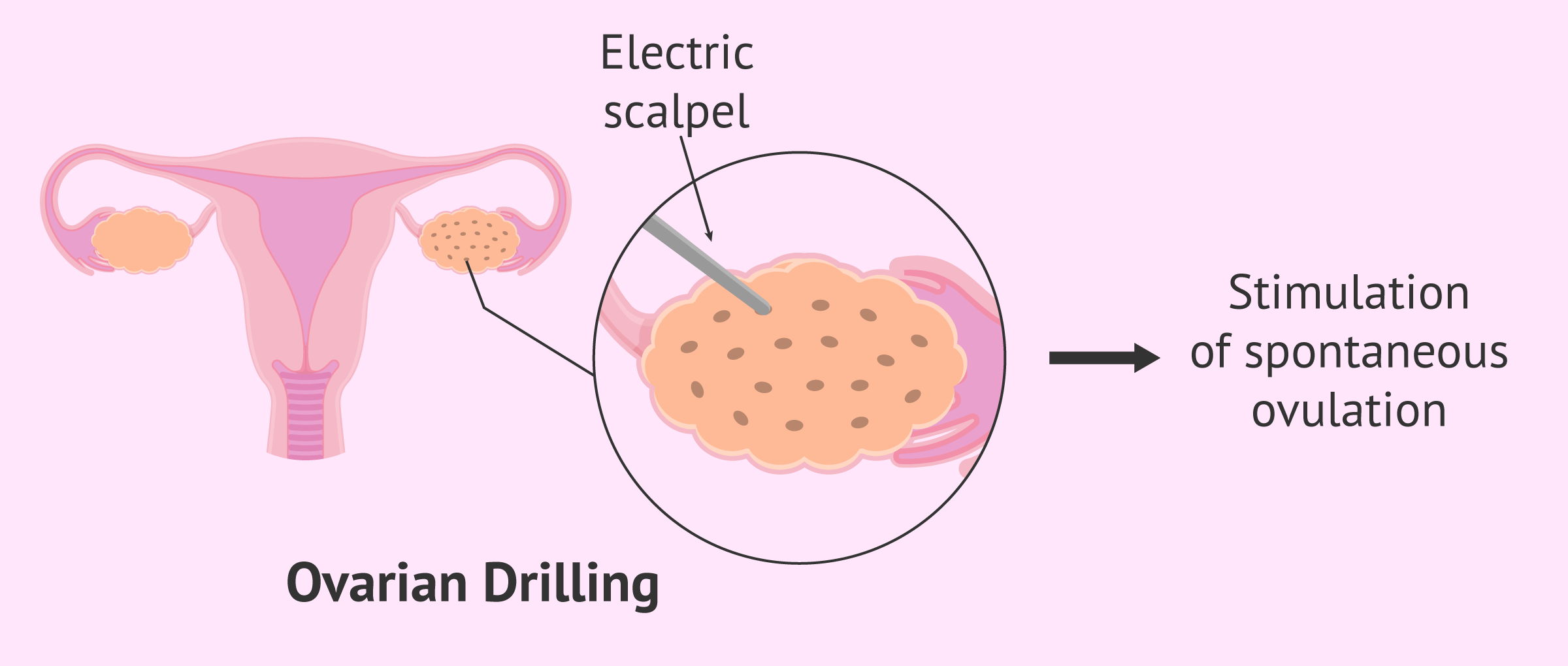
Laparoscopic ovarian drilling (LOD) is a surgical procedure whereby multiple perforations are performed over the ovarian surface using an electric laser or scalpel in order to stimulate spontaneous ovulation.
The following are the advantages of this procedure over a cuneiform resection:
- Less physical damage.
- Reduced chance of developing ovarian adhesions.
- Very effective: ovulatory cycles are achieved in almost all cases.
- It increases sensitivity to clomiphene citrate.
Once the intervention has been performed, it is essential to monitor the patient to evaluate whether spontaneous ovulation has resumed. In addition, it will be convenient to remember the importance of maintaining sexual relations in the days close to ovulation if pregnancy is desired.
Considering seeing a fertility specialist? Don't forget that, in the field of Reproductive Medicine, as in any other medical area, it is crucial that patients rely on the doctors and staff that will help them through their treatment cycle. Logically, conditions vary from clinic to clinic. For this reason, we recommend that you generate your Fertility Report now. It will offer you a list of clinics that have passed our rigorous selection process successfully. Furthermore, the system will make a comparison between the fees and conditions of each clinic so that you can make a better-informed decision.
FAQs from users
Can PCOS be treated naturally?
The most common homeopathic treatment used for PCOS is vitex. This medicinal herbs is a home remedy that has been traditionally used to level off hormone levels, avoid irregular menstrual periods, and reestablish ovulation.
Women with PCOS are recommended to take between 150 and 200 g of vitex daily for at least 3 or 4 months for it to be effective.
What are the benefits of using birth control to treat PCOS?
By administering the pill, hyperandrogenism problems disappear, since it has an effect on various levels:
- Estrogens increase the production of sex hormone binding globulin (SHBG) in the liver, thereby diminishing the amount of free testosterone
- On the other hand, the hypothalamus reduces the release of GnRH, diminishing LH levels, and preventing the ovary from producing more estrogens.
Aside from reducing androgen levels, the pill allows the woman to have regular menstrual cycles, and brings several benefits against acne.
Nowadays, one can find a wide range of oral birth control. The most recommended ones to reduce the effects of male hormones are those that have a greater amount of estrogen and contain progesterone, since this helps to reduce the side effects to the minimum.
For how long should I try with clomiphene until moving on to letrozole to achieve pregnancy with PCOS?
Normally, treatment with clomiphene is typically used for 2 to 6 months. If ovulation has not occurred during this time period, we recommend that you change to another protocol.
If I get pregnant after taking metformin, should I stop treatment?
According to experts, once the patient achieves pregnancy, treatment with metformin should be immediately stopped, except in particular cases where the doctor determines that it should be continued.
What is ovarian drilling?
Ovarian drilling using laparoscopic surgery involves the creation of multiple perforations (about 15 small holes) in the ovarian surface using a laser or electric scalpel to trigger spontaneous ovulation.
This treatment, followed by the administration of clomiphene citrate, seems to be as effective as using gonadotropins. The difference is that is eliminates its disadvantages, since it reduces the risk of OHSS and multiple pregnancy.
Ovarian drilling can be done to one or both ovaries.
Suggested for you
Infertility is one of the main side effects of Polycystic Ovary Syndrome (PCOS), since it is estimated that almost 75% of women who suffer from it have trouble getting pregnant. Get more info by clicking the following link: How Does PCOS Affect Female Fertility?
One of the main risks of women with PCOS who undergo ovarian stimulation is the Ovarian Hyperstimulation Syndrome (OHSS). Want to learn more about it? Click here: What Is OHSS & What Causes It?
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
ACOG Committee on Practice Bulletins—Gynecology. ACOG Practice Bulletin No. 108: Polycystic ovary syndrome. Obstet Gynecol. 2009; 114(4):936-949 (View)
Costello M, Shrestha B, Eden J, Sjoblom P, Johnson N. Insulin-sensitising drugs versus the combined oral contraceptive pill for hirsutism, acne and risk of diabetes, cardiovascular disease, and endometrial cancer in polycystic ovary syndrome. Cochrane Database Syst Rev. 2007;(1): CD005552 (View)
Dafopoulos K, Venetis C, Pournaras S, Kallitsaris A, Messinis IE. Ovarian control of pituitary sensitivity of luteinizing hormone secretion to gonadotropin-releasing hormone in women with the polycystic ovary syndrome. Fertil Steril. 2009;92(4):1378-1380 (View)
Dunaif A. Insulin resistance and the polycystic ovary syndrome: mechanism and implications for pathogenesis. Endocr Rev. 1997;18(6):774-800 (View)
Harrison CL, Lombard CB, Moran LJ, Teede HJ. Exercise therapy in polycystic ovary syndrome: a systematic review. Hum Reprod Update. 2011; 17(2):171-183 (View)
Legro RS, Arslanian SA, Ehrmann DA, et al.; Endocrine Society. Diagnosis and treatment of polycystic ovary syndrome: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2013;98(12):4565-4592 (View)
Legro RS, Brzyski RG, Diamond MP, et al.; NICHD Reproductive Medicine Network. Letrozole versus clomiphene for infertility in the polycystic ovary syndrome [published correction appears in N Engl J Med. 2014; 317(15):1465]. N Engl J Med. 2014;371(2):119-129 (View)
Radosh L. Drug treatments for polycystic ovary syndrome. Am Fam Physician. 2009;79(8):671-676 (View)
Tang T, Lord JM, Norman RJ, Yasmin E, Balen AH. Insulin-sensitising drugs (metformin, rosiglitazone, pioglitazone, D-chiro-inositol) for women with polycystic ovary syndrome, oligo amenorrhoea and subfertility. Cochrane Database Syst Rev. 2012;(5):CD003053 (View)
FAQs from users: 'Can PCOS be treated naturally?', 'What are the benefits of using birth control to treat PCOS?', 'For how long should I try with clomiphene until moving on to letrozole to achieve pregnancy with PCOS?', 'If I get pregnant after taking metformin, should I stop treatment?' and 'What is ovarian drilling?'.
Authors and contributors




