A miscarriage or spontaneous abortion is the involuntary loss of a developing fetus before the 20th week of pregnancy.
The incidence rate of miscarriages is 1 out of 5 pregnancies, that is, 20 percent of pregnancies end up in miscarriage. Most of them occur during the first trimester, particularly between weeks 6 to 12 of pregnancy.
There exist many types of spontaneous abortion based on several factors, as one shall see in the sections below.
Provided below is an index with the 7 points we are going to expand on in this article.
- 1.
- 2.
- 2.1.
- 2.2.
- 2.3.
- 2.4.
- 3.
- 3.1.
- 3.2.
- 3.3.
- 3.4.
- 4.
- 5.
- 6.
- 7.
Types of miscarriages
The different kinds of miscarriage can be classified into various groups. First and foremost, one should learn the differences between:
- Miscarriage
- Not induced by the woman voluntarily, they occur naturally.
- Abortion
- Induced by the pregnant woman, typically in cases of unplanned pregnancy or pregnancy as a result of rape, for instance.
- Therapeutic abortion
- Abortion is induced, but due to medical reasons.

Throughout the following sections, we will focus on the different types of miscarriage, which is to say, those pregnancy losses that occur against the will of the woman.
What is a spontaneous miscarriage?
The definition of spontaneous abortion refers to the involuntary loss of the embryo or fetus before 20 weeks of gestation or when its weight is less than 500 grams.
In general, miscarriage occurs in different phases. First, there is usually the so-called threatened miscarriage, which is detected by slight vaginal bleeding and pain in the uterine area.
In this case, the woman is advised to go to the doctor for an ultrasound scan, to check whether the cervix has started to dilate, and then to rest absolutely.
Broadly speaking, a miscarriage can take place at different stages of pregnancy. The first sign is known as threatened miscarriage, which typically appears in the form of a mild vaginal bleeding and pain in the abdomen.
In such cases, the woman should visit a doctor as soon as possible. He or she will perform an ultrasound scan to see if the cervix has started dilating. If that's the case, your doctor will recommend bed rest.
Symptoms of threatened miscarriage may become more severe and may lead to heavier bleeding, which will correspond to the actual miscarriage. The woman will have more intense pain and the cervix will open to expel the fetus.
Miscarriages can be due to problems in both the fetus and the mother. If you are interested in reading more about this topic, you can continue reading in the following article: What are the main causes of miscarriage?
Miscarriage by frequency
There are two categories of abortion depending on whether they occur in a timely manner or are repeated in the same woman:
- Sporadic abortion
- appears in isolation. It is common in new mothers and does not pose any fertility problem.
- Repeated abortion
- when two or more spontaneous abortions occur. It may be primary recurrent miscarriage, if there has been no full-term pregnancy; or secondary recurrent abortion, if the woman has previous children.

Repeat abortion requires an additional study to determine its cause and to be able to apply a specific treatment that allows the woman to carry a pregnancy to term.
Get more info by clicking the following link: What Is Recurrent Miscarriage? – Causes, Symptoms & Treatment.
Miscarriage according to gestational age
As we have said, spontaneous abortion is one that can take place up to the 20th week of gestation. Within this period of time, it is possible to classify abortions according to the moment they occur:
- Early abortion
- occur before the 12th week of pregnancy and are the most frequent.
- Late-term abortion
- takes place after 12 weeks.

Early abortions can occur when the woman already knows she is pregnant or even before taking a pregnancy test. The latter go unnoticed by the woman and are confused with a simple menstrual delay.
Biochemical miscarriage
A specific case worth mentioning is biochemical abortion, also known as microabortion. These are very early pregnancy losses after a positive pregnancy test.
The most probable causes of biochemical pregnancy are the initial defects in the fertilization of the ovum with the sperm, the abnormal cell divisions of the embryo after fertilization or alterations in implantation.

You can find all the information regarding micro abortion in the following post: What Is a Chemical Pregnancy? – Symptoms, Causes & Treatment.
Miscarriage according to the gestational sac
There are two types of abortion depending on whether or not an embryo is observed inside the gestational sac:
- Anembryonic sac or blighted ovum
- The gestational sac appears empty, without an embryo inside, due to early embryonic arrest.
- Embryonic sac
- The gestational sac contains an embryo, but no fetal heartbeat can be detected due to late embryonic arrest.
Most of the miscarriages in the first trimester are due to an embryonic pregnancy, whose main causes are genetic alterations in the embryo. If you are interested in knowing more about this topic, you can continue reading in the following post: What Causes a Blighted Ovum? – Symptoms, Diagnosis & Treatment.
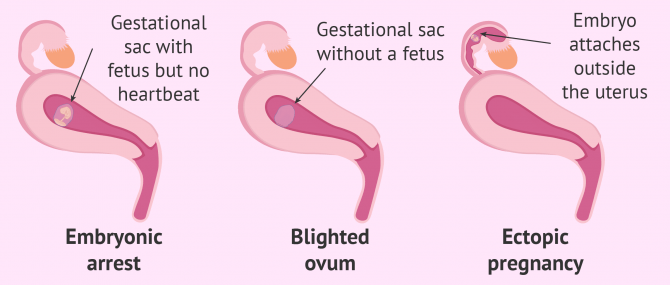
In this section we can also include the ectopic pregnancy or extrauterine. This type of pregnancy consists of the embryo implanting in a place other than the endometrium. The most common in this case is to find the gestational sac in the fallopian tube. Obviously, this is a non-viable pregnancy that ends in abortion.
To know all the types of ectopic pregnancy that exist, you can click on the following link: What Causes an Ectopic Pregnancy? – Symptoms, Diagnosis & Treatment.
Miscarriages according to the clinical variety
After pregnancy loss, it is necessary for the body to eliminate all embryonic remains naturally. Otherwise, it would be necessary to take measures to remove them, such as curettage.
Depending on whether the fetus and the abortive remains are eliminated naturally or not, the following types of abortion can be found:
- Complete or accomplished abortion
- all uterine contents have been expelled after fetal death. No further treatment is necessary, as the bleeding stops, the pain disappears, and the cervix closes on its own.
- Incomplete abortion
- the contents of the uterus are not completely expelled after fetal death. It will be necessary to remove the remains of fetal and placental tissue to prevent bleeding and infections that may pose a risk to maternal health.
- Delayed or missed abortion
- the embryo dies, but the woman is unable to eliminate the gestational sac for several weeks or even months. It usually occurs between weeks 8 and 12 of gestation. What happens is that the symptoms of pregnancy gradually disappear, the uterus stops growing, and the pregnancy tests become negative, approximately 10 days after fetal death.

Both incomplete abortion and missed abortion require medical intervention to curettage and remove the contents of the uterus. If all the fetal remains are not removed, it could lead to a septic abortion due to infection, which entails a high risk for the mother.
FAQs from users
Is delayed abortion common?
Delayed abortion, which we also know as missed abortion, is one that takes place during the first trimester of pregnancy. It is usually due to a situation where the fetus does not progress and stops growing during pregnancy.
Read more
Can you have a miscarriage before missed period?
Yes. In that case, it is called subclinical very early miscarriage, that is, the woman didn't even know that she was pregnant. Bleeding is confused with menstrual flow.
How long does miscarriage bleeding last?
It varies from woman to woman and the characteristics of each type of miscarriage. Broadly speaking, when it's a complete miscarriage, vaginal bleeding can last about a week or two approximately.
Is D&C necessary in all cases after a miscarriage?
No, in cases of complete miscarriage, or when embryo development stops at the earliest stages, the remaining pregnancy tissue is removed with menstrual flow. In other words, D&C is not necessary in these cases.
Recommended readings
In most cases, before the woman has a miscarriage, she has a threatened miscarriage, which can lead to an actual miscarriage or stop and lead to a good outcome. Check out this for information: Threatened Miscarriage - What Are the Odds of Miscarriage?
Bleeding during pregnancy can be caused by a number of factors and is associated with complications in all cases. To learn more about the potential causes of each type of bleeding, read: Causes of Bleeding During Pregnancy - What's Normal & What's Not?
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Devall AJ, Coomarasamy A. Sporadic pregnancy loss and recurrent miscarriage. Best Pract Res Clin Obstet Gynaecol. 2020 Nov;69:30-39. (View)
Dimitriadis E, Menkhorst E, Saito S, Kutteh WH, Brosens JJ. Recurrent pregnancy loss. Nat Rev Dis Primers. 2020 Dec 10;6(1):98. (View)
Jackson T, Watkins E. Early pregnancy loss. JAAPA. 2021 Mar 1;34(3):22-27. (View)
Kim C, Barnard S, Neilson JP, Hickey M, Vazquez JC, Dou L. Medical treatments for incomplete miscarriage. Cochrane Database Syst Rev. 2017 Jan 31;1(1):CD007223. (View)
Kulier R, Kapp N, Gülmezoglu AM, Hofmeyr GJ, Cheng L, Campana A. Medical methods for first trimester abortion. Cochrane Database Syst Rev. 2011 Nov 9;2011(11):CD002855. (View)
Larsen EC, Christiansen OB, Kolte AM, Macklon N. New insights into mechanisms behind miscarriage. BMC Med. 2013 Jun 26;11:154. (View)
Sapra KJ, Joseph KS, Galea S, Bates LM, Louis GM, Ananth CV. Signs and Symptoms of Early Pregnancy Loss. Reprod Sci. 2017 Apr;24(4):502-513. (View)
FAQs from users: 'What is a therapeutic abortion?', 'Is delayed abortion common?', 'Can you have a miscarriage before missed period?', 'How long does miscarriage bleeding last?' and 'Is D&C necessary in all cases after a miscarriage?'.
Authors and contributors




More information about Cristina Algarra Goosman

I had a miscarriage a couple of months ago, I was 28 weeks pregnant and it was very hard on us. I am 35 and time isn´t in our favor. I wanted to know when we could start trying again. Thanks
Hello Natasha,
After a miscarriage, specifically after a miscarriage in the second or third trimester, there is some medical and psychological consideration that has to be taken into account. Typically doctors advise you to wait 6 months more or less to try to conceive again.
On the psychological aspect, a loss is very traumatic both in the individual´s mental health as well as the couple´s dynamic and social encounters.
I recommend you visit a physician so they can evaluate your physical capability of trying to conceive, also speak to a counselor so they can assess your psychological needs and establish any changes are therapy that must be implemented before embarking on the journey again.
Here is an article that sheds some light on the topic: Pregnancy after a miscarriage – When to conceive again.
I hope I could answer your question.
All the best.
Hi, I had a positive pregnancy test on DPO 10, I kept on testing and the line got a bit darker but when my period was due I started to bleed, I tested again it was still a positive but very very faint line. Could this mean I had a miscarriage or just a faulty test?
Hello Seline,
As you have described it seems like you suffered a chemical pregnancy, a very early loss of the embryo in the early stages of development, even before it completely implants in the uterus.
I recommend you go to the doctor so they can explore you and see if everything is okay and you experienced a chemical pregnancy. You can learn more about this topic in the following article: What is a chemical pregnancy?
I hope I could help you,
All the best