IVF using donor sperm: the process, costs and its success rates
In vitro fertilization (IVF) is preferably be performed with the eggs and sperm of the intended future parents. However, when there is no male partner or when a male partner has serious fertility problems, IVF with donor sperm may be necessary.
This technique consists of the union of the eggs extracted from the future mother with the sperm from a sperm donor, who has decided to donate his gametes. Depending on the local law and private agreements, sperm donation can both be anonymous or from a known donor.
The different sections of this article have been assembled into the following table of contents.
Contents
- 1.
- 1.1.
- 1.2.
- 1.3.
- 1.4.
- 1.5.
- 1.6.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 7.1.
- 7.2.
- 7.3.
- 7.4.
- 7.5.
- 7.6.
- 7.7.
- 8.
- 9.
IVF procedure
IVF is an assisted reproduction technique that consists of the union of the gametes (egg and sperm) in the laboratory and not inside the woman's body.
This technique requires the stimulation of the ovaries to obtain various eggs, which are extracted by egg retrieval. The eggs are then fertilized with the sperm and the resulting embryo is transferred to the mother's uterus to achieve a pregnancy.

The phases that are carried out are described below.
Ovarian stimulation
The patient must undergo hormonal treatment for ovarian stimulation to occur. This step usually begins on day three of the menstrual cycle and lasts about 10 days, allowing for a larger number and size of eggs to be obtained. Various ultrasound checks are carried out throughout the phase.
When the desired number and size of the ovarian follicles are reached, their maturation is stimulated and the follicular puncture is performed.
Ovarian follicles are fluid-filled structures located in the ovaries that contain the egg that is going to mature, that is, they are structures where eggs mature inside the ovary.
Follicular puncture and sperm treatment
Follicular puncture or egg retrieval consists of a surgical procedure under ultrasound control in which the liquid from the ovarian follicles is aspirated vaginally after a small amount of sedation. The aspirated follicular fluid is analyzed in the laboratory to obtain the eggs.
In donor sperm IVF, the sperm comes from a donor bank. All donor samples are frozen after collection for a minimum of 6 months to ensure the absence of transmissible infections.

We recommend that you find out more about the egg retrieval phase in the following article: How does egg retrieval work during IVF?
Egg fertilization
Once the most suitable donor has been chosen, in compliance with current legislation and with similar characteristics to the mother-to-be or the couple, a sample is defrosted and processed in the andrology laboratory to obtain the spermatozoa.
The fertilization of the egg can be:
- Classic IVF
- the egg and a drop of donor sperm with thousands of sperm are placed in the same laboratory dish.
- ICSI
- means intracytoplasmic Sperm Injection (ICSI). In this case, the best spermatozoon selected is inserted into the egg. The process is carried out with the aid of a micro-injector.

Because the semen sample is donor sperm and of good quality, it would be possible to perform conventional IVF. However, the use of ICSI is now very common and is displacing conventional IVF.
Embryo culture in the laboratory
After completing the fertilization of the eggs, the zygote will pass to the state of an embryo and will be left in culture in incubators, controlling its development and evolution until the day of the transfer to the uterus of the future mother.
Incubators have the necessary characteristics and the right temperature for embryonic development.
Embryo transfer
The transfer consists of depositing the embryos in the uterus with the help of a fine cannula. It is advisable to go on the day of the transfer with a slightly full bladder to encourage a straight path from the cannula to the uterus. This process does not cause pain or require anesthesia.
This phase is carried out on day 2-3 or day 5-6, depending on the characteristics of the situation and the approach of each laboratory.

The number of embryos to be transferred is highly debated and also depends on the legislation of the respective country limiting the number of transferred embryos to a maximum of 2, like is the case in the U.K. In other countries with more liberal legislation such as the U.S. there is still a consensus among specialists that not more than two embryos be transferred in order to minimize the risks of multiple pregnancies as this would implicate serious consequences to the health of the mother and fetuses.
The implantation of the transferred embryo(s) can be promoted by administering estrogen and progesterone orally, vaginally, or in patches to the patient. This hormonal medication will allow your endometrium to acquire the trilaminate aspect and an optimal thickness equal to or greater than 5 mm for embryo implantation.
The rest of the embryos not transferred are preserved by freezing or vitrification for future cycles, without the need to repeat ovarian stimulation or follicular puncture. If no more cycles will be performed, there are several options:
- Keep the embryos frozen until they can be destroyed.
- Donate the embryos to other couples.
- Donate the embryos for scientific reseach purposes.

If you want to learn more about this process you can visit the link: Embryo vitrification.
Pregnancy test
To confirm whether the woman has become pregnant, a pregnancy test is performed 12-15 days after the transfer by determining betahCG (also called human chorionic gonadotropin hormone or pregnancy hormone).
Generally speaking, there are two options that can occur after embryo transfer into the uterus and they are detailed below:
- Positive outcome
- the treatment is successful. The administration of progesterone is continued until the pregnancy is confirmed by an ultrasound scan where the 6-7 week old embryo is observed and its heartbeat can be heard.
- Negative result
- the treatment is not successful and does not end in pregnancy. In this case, there is no need to despair or lose hope. If there are frozen embryos, a second cycle can be performed. If there are no frozen embryos, a second complete IVF cycle would have to be repeated.

It is very important not to do the pregnancy test before the date you have been given, due to the possibility of any erroneous results that could occur by doing so.
Sperm donor selection
Sperm donors are young, healthy boys who undergo a series of physical and psychological tests that confirm their ability to be donors. Following requirements have to be met by the sperm donors:
- Being between 18 and 45 years old.
- No family or personal history of a chronic or serious disease.
- Not being adopted since his background must be known.
- Sample with excellent sperm quality and a high concentration and mobility of the spermatozoa. Furthermore, since all samples are to be frozen, it is essential that the spermatozoa pass the thawing test, i.e. that they survive the sperm freezing.
- Karyotype without chromosomal alterations.
- Negative serologies for HIV, Hepatitis B, syphilis, etc.
- No sexually transmitted deseases such as chlamyidia and gonococcus.

The donation can be anonymous or from a known donor and is a voluntary act which is remunerated. If an anonymous donor is used a donor with the most similar phenotypical characteristics to the recipient or her partner will be selected. The recipients may receive general information about the donor such as eye color or height but no identifying information.
When is it necessary?
The main indications for in vitro fertilization with donor sperm are as follows:
- Women without partner who want to become single mothers.
- Women in a lesbian relationship.
- Severe male factor: important alterations of the sperm quality might require a male gamete donation. Severe alterations in seminal concentration (oligospermia), motility (asthenospermia), morphology (teratozoospermia), or the combination of some or all of them, may make patients consider the use of donor sperm. These are usually cases in which one or more attempts have been made to use the partner's semen with poor results and in which the main factor involved in the failure of the technique is considered to be low seminal quality. Likewise, those patients who present a high level of sperm DNA fragmentation that does not revert with antioxidant treatment or who want to maximize their chances of success may be an indication for switching to a sperm donor.
- Genetic diseases of the male: Certain diseases that cannot be diagnosed by Pre-implantation Genetic Diagnosis (PGD) as well as the impossibility or desire of couples not to resort to it, may make it necessary to use a sperm donor to avoid transmission to the offspring of the disease.
- Karyotype alterations: patients with karyotype alterations who do not wish to resort to PGD techniques or who, after having resorted to it, due to the high number of chromosomally altered embryos, decide to switch to the sperm bank.

In any case, it is essential to follow all the advice of the specialists to achieve the highest possilibity of getting pregnant from the treatment.
Success rates of IVF with donor sperm
The success rate of assisted reproduction treatments varies depending on the technique and the individual cases of each patient who undergoes them.
The success of IVF with donor sperm depends, to a great extent, on the age of the woman, since in order to be a sperm donor the sperm quality must be very good.
However, maternal age is one of the limiting factors when it comes to the success of IVF, since the female reproductive capacity decreases as age increases, this decrease being especially marked after the age of 35. This is due to the fact that the oocytes decrease in quality and quantity with the passage of time.
Other aspects to be taken into account for the effectiveness of IVF treatment may be:
- The characteristics of the uterus and endometrium.
- The conditions of the embryo culture.
- The fertilization technique: there are differences between conventional fertilization and ICSI.
- Whether the process is being carried out with previously vitrified embryos.
- The number of embryos transferred. As the number of embryos transferred increases, there is a greater possibility that one of them will implant, resulting in gestation. However, the greater the number of embryos transferred, the greater the risk of multiple gestation, which is dangerous for the mother and the fetuses.

According to the data recorded by the Spanish Fertility Society (National Registry of Activity 2023- SEF Registry), the rate of gestation per transfer of fresh embryos from IVF with own eggs and donor sperm is 37,0%, while the rate of delivery per transfer performed with fresh embryos is 27,1%.

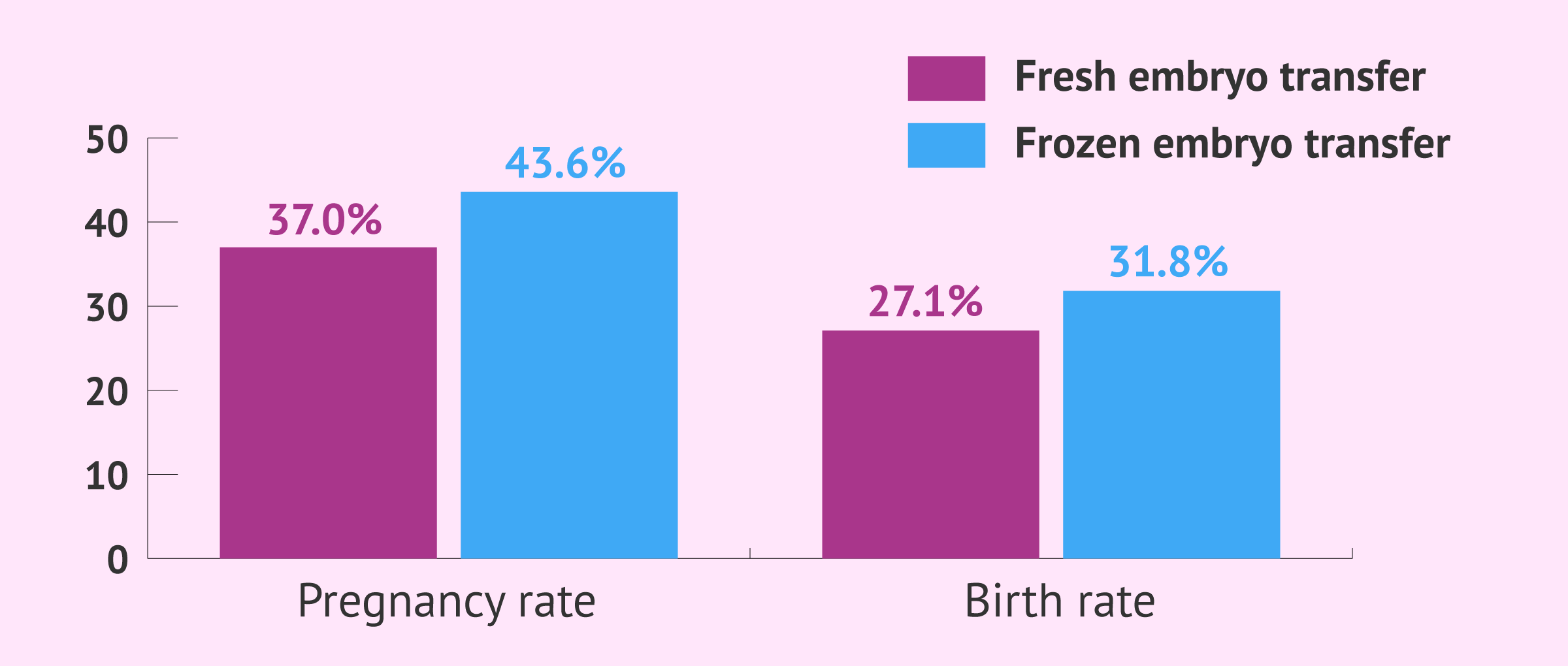
In the case of frozen embryos, the data collected decrease slightly, being 43,6% and 31,8% respectively.
Statistical data in this article shall not be used to imply or predict an outcome certainty to a specific individual within a population at risk.
How much does IVF with donor sperm cost?
In general, using donor sperm instead of the husband's increases the overall cost of an IVF cycle. On average, the cost of IVF with sperm donation ranges from €3,000 to €5,000, although it varies by country and clinic.
In the UK, for instance, treatment on the NHS may be offered to some couples aged 23 to 29 years provided that they meet all the requirements established by the local health authorities.
Often, this amount does not include:
- Prior medical tests: Since they vary from person to person depending on the medical history, giving a fixed price quotation is difficult.
- Medications: Although medications needed depend also on each patient, the average cost ranges from £350 to £650.
- Donor compensation: Donors are paid a compensation of about £40-50 per clinic visit.
Did you know that we can help you to choose a fertility clinic for your IVF with donor sperm cycle? All you have to do is get your Fertility Report now. This easy-to-use tool is capable of filtering the best clinics and tailor an individual report exclusively for you with useful tips that will help you make a well informed decision.
If you decide to do IVF abroad, the costs derived from travel and accommodation should be added to the overall cost as well. Some fertility clinics arrange travel plans to make it easier and more affordable for their patients.
Reciprocal IVF
For same sex female couples, there is a variant of in vitro fertilization treatment called reciprocal IVF or co-IVF.
Reciprocal IVF consists of obtaining the eggs from one of the women, which are fertilized with the sperm from a donor bank. The embryos generated are transferred to the uterus of the second woman, i.e. the one who has not provided the eggs. Therefore, the reciprocal IVF is the same as a normal IVF, but taking into account that both women participate in the process.
The costs of reciprocal IVF is similar to sperm donation IVF for which the costs are situated around €3,900–€5,900 plus the cost of fertility drugs.

If you want to learn more about this reproductive technique, we recommend you read on here: What is reciprocal IVF?
FAQs from users
Is IVF with donor sperm or embryo adoption better for single women?
This will depend on the particular characteristics of each person and their circumstances (economic level, partner, age of the patient, etc.).
A single woman can undergo in vitro fertilization (IVF) or artificial insemination (AI) with donor sperm to achieve pregnancy. If Artificial Insemination (AI) is not possible due to poor ovarian response, an In Vitro Fertilization (IVF) with her eggs and donor sperm will be considered.
If after fertilization a poor response has been obtained, in this particular case, we could consider the need to perform an IVF with donor eggs and donor sperm. This is what we call double donation. Although embryo adoption could also be considered.
What are the requirements for donors to donate their semen?
Sperm Banks ask donors to undergo a comprehensive health evaluation, including genetic screening and infectious disease testing with a complete physical exam.
Basic Requirements vary but examples are:
- Donors of all ethnicities, races and nationalities are encouraged to apply
- 5’7” tall for most donors (5’4” for donors of Hispanic or Asian descent)
- Between the ages of 18 and 44
- Physically and emotionally healthy
- College-educated professional, student pursuing a degree or certificate beyond high school, or in a successful, long-term career (i.e. Civil Service, Trade Specialty)
- Be willing to commit to a minimum of one visit per week for a minimum of 90 days
What are the main indications for IVF with donor sperm?
IVF treatment with donor sperm is usually indicated for women between 18 and 43 years old, single women, couples of women or women whose partner has azoospermia, poor sperm quality or genetic alterations.
For women who do not present alterations in fertility (low ovarian reserve, endometriosis, obstructed tubes, early ovarian failure...), we can evaluate the option of artificial insemination with donor sperm before performing an IVF, although In Vitro Fertilization always gives better results. IVF is indicated in these cases when no pregnancy has been achieved after 3-4 artificial inseminations.
Before undergoing assisted reproduction treatment, even if the woman does not present infertility, it is important to study the case of each patient or couple. With a basic fertility study, we can guide the patient or couple to the most appropriate treatment.
Can IVF be done using half donor sperm and half partner sperm?
In some countries, this practice is perfectly possible. Some fertility clinics offer this possibility to women in order to increase their chances for success in a single cycle. Some eggs are fertilized with donor sperm, and others with that of the husband/partner. Usually, embryo transfer is firstly done with the embryos obtained with the husband's sperm, and the remainder only in case the first cycle fails.
Is it possible to do IVF with both donor eggs and sperm?
Yes, it is. This technique is known as double-donor IVF and is indicated in the following cases: problems in the ovaries (either because of age or other unknown causes), sperm problems (zero or low sperm count, or poor motility), and single females.
For further information, we recommend you to visit the following post: What is double-donor IVF?
Are there any changes needed in the woman's treatment when using donor sperm?
No, the hormonal treatment of ovarian stimulation and the egg retrieval do not differ when performing IVF with partner or donor sperm. The process only changes if donated eggs are used instead of the woman's own eggs.
With respect to treatment with donor sperm, everything relative to the woman (future mother) is the same.
How is an anonymous sperm donor assigned to the recipient?
A sperm donor is selected on the basis of genetic compatibility, similar phenotipic characteristics and physical likeness to the recipient woman or the partner.
You can find more information on this topic in this article: Sperm donor selection: What criteria is followed?.
Suggested reading
It has been mentioned that women undergo an ovarian stimulation phase during the IVF treatment process. Therefore, if you would like to learn more about the prices of the medication that is administered, do not hesitate to read the following article: The cost of hormonal medication in assisted reproduction treatments
If you also want to find out more about embryo development or types of culture, you can go to the following link: Embryo culture in the in vitro fertilization laboratory (IVF)
We make a great effort to provide you with the highest quality information.
🙏 Please share this article if you liked it. 💜💜 You help us continue!
References
Bruna I, Sánchez de Rivera MD, Collado O. Protocolo de diagnóstico básico de la disfunción reproductiva. En: Diagnóstico y prevención de la disfunción reproductiva. Documentos de consenso SEGO, 2011, pp 71-89.
Comisión Nacional de Reproducción Humana Asistida (CNRHA) (2015). Aspectos legales y éticos de la donación. En: Registro Nacional de Donantes de Gametos y Preembriones. Ministerio de Sanidad, Consumo y Bienestar Social de España (View)
Ferraretti AP, La Marca A, Fauser BCJM, Tarlatzis B, Nargund G, Gianaroli L ESHRE consensos om the definition of “poor response” to ovarian stimulation for in Vitro fertilization: the Bologna criteria. Human Reproduction 2011; 26 (7): 1616-1624.
Gardner D, Rizk B, Falcone T. Human Assisted Reproductive Technology. Cambridge University Press 2011
Goldberg JM, Mascha E, Falcone T, Attaran M. Comparison of intrauterine and intracervical insemination with frozen donor sperm: a meta-analysis. Fertil Steril. 1999 Nov; 72(5):792-5 (View)
Ley 14/2006, de 26 de mayo, sobre técnicas de reproducción humana asistida. Jefatura del Estado «BOE» núm. 126, de 27 de mayo de 2006 Referencia: BOE-A-2006-9292 (View)
Sociedad Española de Fertilidad. Registro Nacional de Actividad 2023-Registro SEF (View)
Sociedad Española de Fertilidad (SEF) (febrero de 2012). “Saber más sobre fertilidad y reproducción asistida”. En colaboración con el Ministerio de Sanidad, Política Social e Igualdad del Gobierno de España y el Plan de Calidad para el Sistema Nacional de Salud.
Sociedad Española de Fertilidad (SEF) (2011). Manual de Andrología. Coordinador: Mario Brassesco. EdikaMed, S.L. ISBN: 978-84-7877.
W.N. Spellacy,S.J. Miller,A. Winegar. A pregnancy after 40 years of age. Obstet Gynecol, 68 (1986), pp. 452-454.