Traditionally, results with fresh embryo transfer were better than with frozen embryos. However, today, thanks to advances in the field of assisted reproduction, the survival rate of embryos after thawing is quite high.
The technique used to cryopreserve embryos is vitrification, an ultra-fast freezing method that prevents the formation of crystals. However, it is important to have skill in the technique and good working protocols to avoid damaging the embryos.
Provided below is an index with the 8 points we are going to expand on in this article.
- 1.
- 1.1.
- 2.
- 3.
- 4.
- 4.1.
- 4.2.
- 4.3.
- 4.4.
- 4.5.
- 5.
- 6.
- 7.
- 8.
Frozen embryo transfer
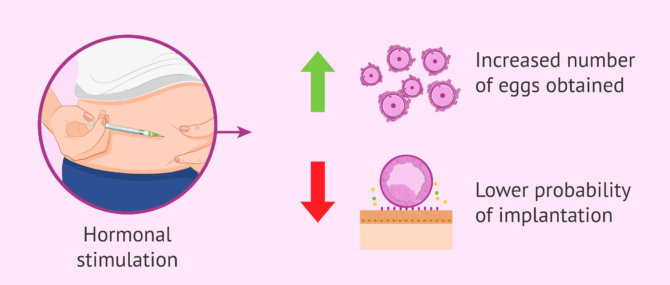
In a natural menstrual cycle, most commonly only one egg is matured and released with ovulation. For this reason, in in vitro fertilization (IVF) treatments, hormonal stimulation is performed in order to obtain a greater number of eggs. This means that, thanks to ovarian stimulation, more than one egg will reach the final stage of maturation than occurs naturally.
Although this increases the probability of success of these techniques, stimulation also has detrimental effects on the endometrium (the layer that lines the surface of the uterine cavity), negatively affecting embryo implantation in fresh cycles.
Therefore, the endometrium is more receptive in frozen embryo transfers than in fresh cycles, since it has had a whole menstrual cycle to recover from the effects of hormonal stimulation.
Until relatively recently, slow freezing was the method used to cryopreserve embryos left over from assisted reproduction treatments and the results obtained were limited.
At present, embryos are cryopreserved using the vitrification technique, which consists of ultra-rapid freezing of the embryos. Through this procedure, very high survival rates (90-95%) are achieved due to the fact that the damage suffered by the embryos in the freezing process is minimized.
Therefore, these advances in cryopreservation make it possible to vitrify embryos without compromising success rates and even improving them.
Success rates: fresh vs. vitrified embryos
One of the most frequent doubts in assisted reproduction consultations is whether freezing decreases the probability of the embryo implanting. The short answer is no; in fact, in many cases, it improves it.
Thanks to the vitrification technique (ultrafast freezing), the survival rate of blastocysts upon thawing is quite high.
According to the latest National Activity Register of the Spanish Fertility Society (SEF) for the year 2023, the results are as follows:
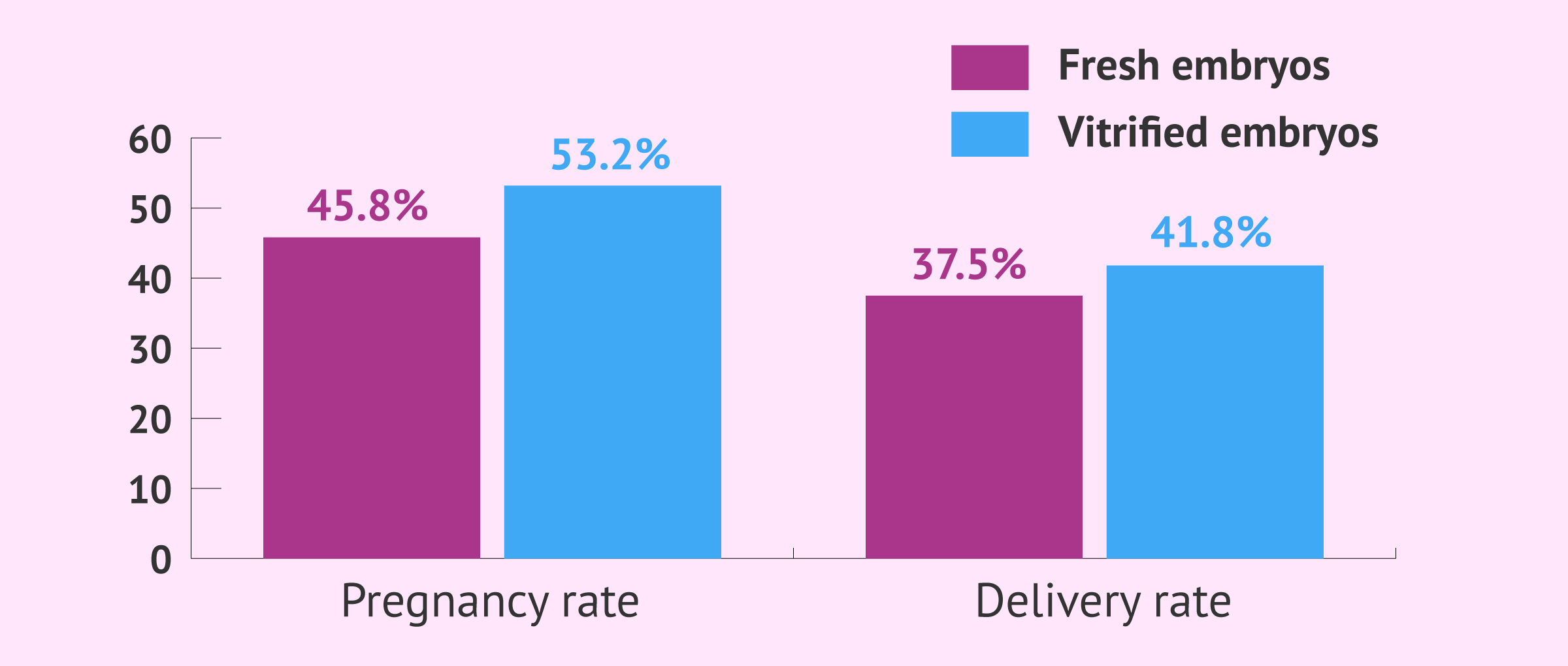
- Pregnancy rate: SEF data shows that the pregnancy rate per transfer of frozen embryos (especially when a preimplantation genetic test or PGT has been performed) is 53.2%, while with fresh embryos it is around 45.8%.
- Delivery rate: regarding the delivery rate (live birth at home), the figures for 2023 are 37.5% with fresh embryos and 41.8% with vitrified embryos.
Statistical data in this article shall not be used to imply or predict an outcome certainty to a specific individual within a population at risk.
Why transfer at the blastocyst stage?
Advances in assisted reproduction techniques have also made it possible to considerably improve embryo culture, that is, the conditions in which embryos are kept in the laboratory until they are transferred or vitrified. This has made it possible to obtain more embryos of good quality and reach the blastocyst stage.
The blastocyst stage is reached at day 5-6 of embryonic development.
Transfer at this stage has a number of advantages:
- It allows a better embryo selection, since more developmental information is obtained and only the best quality embryos are able to reach this stage.
- There is a better synchronization with the endometrium, which increases the chances of implantation.
- It offers to make more single embryo transfers to avoid multiple pregnancies without compromising the chances of success due to the above two points.

Risks
Although vitrified blastocyst transfer can provide very good implantation rates, it is not always the best option.
On the one hand, it is important that the vitrification protocol is optimized to obtain very good results. Blastocysts contain a lot of water inside and this makes the freezing process difficult, so if a good cryopreservation program is not in place, the results will be worse than in fresh.
In addition, it should be noted that not all embryos reach this stage: only those that are of good quality.

Therefore, the risk of no embryo reaching this stage must be assessed. Therefore, the transfer of vitrified blastocysts should not be performed in all patients, but should only be indicated in those who can benefit from this therapeutic option.
FAQs from users
In cases of ovodonation, is delayed blastocyst transfer recommended?
It is not mandatory as long as the endometrium is well prepared for the transfer. However, in cases in which PGD is also performed at the blastocyst stage (5th day of development), with massive sequencing as a platform for genetic analysis, it will be mandatory to vitrify the embryos, while waiting for the cytogenetic results (10-15 days).
If I forget to take progesterone after the transfer of a frozen embryo, can I spoil my transfer?
The drugs that we take have a time of activity in our organism and for this reason they are indicated with an administration interval. It follows that one should be as strict as possible with all the medication, since forgetfulness could lead to a drop in the concentrations of the drug in the body, and therefore, the partial or total loss of its effectiveness.
It is not possible to determine the negative effect of forgetting a particular dose, since it depends on several factors such as the total dose administered, the dosing interval, the number of days we have been taking it, etc... However, I do not believe that missing a single progesterone tablet has any side effects.
When we have the feeling that this has happened we should restart taking it as soon as possible and even if we have doubts we can take a supplementary pill, since no side effects have been observed from increasing the administration of progesterone from 600 to 800 or 1000 mg per day (from 3 to 5 tablets of 200 mg).
Is endometrial preparation needed for frozen embryo transfer?
Frozen embryo transfers can be performed in either a natural or a substituted cycle. In the case of the natural cycle, the natural hormones of the patient's menstrual cycle are used and the evolution of the follicle and endometrium is monitored by ultrasound, without administering any medication. Once ovulation has occurred (release of the mature egg), treatment with progesterone is initiated.
In substituted cycles, estrogens are administered to prepare the endometrium, either in the form of patches or pills. When the endometrium is observed by ultrasound to be prepared, progesterone is administered.
It will be done in one way or another depending on the characteristics of each patient: if she has a menstrual cycle, results of previous cycles.... In addition, there may also be variations in these treatment guidelines that we have mentioned, such as administering GnRH analogs, for example.
Are the symptoms after transferring frozen blastocysts the same as with fresh transfers?
Yes, since there are no differences between the two transfers, the procedure is the same. The only thing that may vary is that in the fresh transfer there are symptoms of hormonal stimulation.
Can an embryo that has been thawed be frozen again?
Yes, as long as vitrification and devitrification are carried out correctly, an embryo can survive several freezing cycles without compromising its viability and being able to carry out implantation.
Suggested for you
As mentioned above, the transfer of frozen embryos is very similar to that of fresh embryos. If you want to know in detail all the steps of this procedure, we recommend you to visit the following link: Frozen embryo transfer.
On the other hand, one of the most relevant decisions in IVF treatments is whether to perform the transfer at day 3 or at the blastocyst stage. You can learn more about the advantages and disadvantages of each of these options at the following link: Embryo transfer on day 3 or day 5?
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Abha Maheshwari, Shilpi Pandey, Edwin Amalraj Raja, Ashalatha Shetty, Mark Hamilton, Siladitya Bhattacharya. Is frozen embryo transfer better for mothers and babies? Can cumulative meta-analysis provide a definitive answer? Hum Reprod Update. 2018 Jan 1;24(1):35-58. doi: 10.1093/humupd/dmx031 (See)
Barbara Lawrenz, Carol Coughlan, Laura Melado, Human M Fatemi. The ART of frozen embryo transfer: back to nature! Gynecol Endocrinol. 2020 Jun;36(6):479-483. doi: 10.1080/09513590.2020.1740918 (See)
Mehmet Resit Asoglu, Cem Celik, Mustafa Bahceci. Frozen blastocyst transfer improves the chance of live birth in women with endometrioma. Gynecol Endocrinol. 2020 Oct;36(10):902-906. doi: 10.1080/09513590.2020.1781082.
Mei Fang Zeng, Liu Ming Li. Frozen blastocyst transfer reduces incidence of ectopic pregnancy compared with fresh blastocyst transfer: a meta-analysis. Gynecol Endocrinol. 2019 Feb;35(2):93-99. doi: 10.1080/09513590.2018.1497154 (See)
S Mackens, S Santos-Ribeiro, A van de Vijver, A Racca, L Van Landuyt, H Tournaye, C Blockeel. Frozen embryo transfer: a review on the optimal endometrial preparation and timing. Hum Reprod. 2017 Nov 1;32(11):2234-2242. doi: 10.1093/humrep/dex285.
FAQs from users: 'In cases of ovodonation, is delayed blastocyst transfer recommended?', 'If I forget to take progesterone after the transfer of a frozen embryo, can I spoil my transfer?', 'Is endometrial preparation needed for frozen embryo transfer?', 'Are the symptoms after transferring frozen blastocysts the same as with fresh transfers?', 'Can an embryo that has been thawed be frozen again?' and 'What are the risks of transferring vitrified blastocysts?'.
Authors and contributors





