Gonadotropin-releasing hormone (GnRH) is a hormone produced by the neurons of the hypothalamic arcuatus nucleus and then secreted into the portal circulation of the pituitary gland.
Its function is to regulate the production of gonadotropins (FSH and LH) by the pituitary gland, which is essential for the proper functioning of the male and female reproductive systems.
In recent years, numerous GnRH analogs have been synthesized for use as drugs in assisted reproduction treatments.
Provided below is an index with the 8 points we are going to expand on in this article.
- 1.
- 2.
- 3.
- 3.1.
- 3.2.
- 3.3.
- 4.
- 4.1.
- 4.2.
- 4.3.
- 4.4.
- 5.
- 6.
- 7.
- 8.
Characteristics of GnRH
GnRH is a decapeptide, i.e. its structure is made up of 10 amino acids arranged in a linear sequence. Furthermore, since it is produced by neurons, GnRH is considered to be a neurohormone.
Other relevant characteristics of GnRH are the following:
- The gene that encodes the precursor of GnRH is located on the short arm of the chromosome 8.
- The secretion of GnRH is pulsatile, that is, it is released into the portal system by pulses of different amplitude and frequency.
- Its half-life is very short, about 2-4 minutes.
- GnRH cannot be detected in peripheral blood, so it cannot be quantified in a normal blood test.

Mechanism of action
The peak of GnRH activity begins at puberty and continues throughout the reproductive life of both men and women.
GnRH has an endocrine function: it travels to the pituitary gland through the portal system, activates its receptor and stimulates the release of FSH and LH from the adenohypophysis.
These pituitary hormones then travel through the bloodstream and exert their function on a woman's ovaries or a man's testicles.
In women, the frequency of the GnRH pulses controls the production of FSH and LH throughout the menstrual cycle, which is critical to proper cycle functioning. Unlike in men, where GnRH is secreted in pulses of constant frequency.
The pulsatile activity of GnRH can be seen interrupted or altered by different factors, which would affect the male and/or female reproductive function as the case may be. These factors are the following:
- A malfunctioning of the hypothalamus, whether due to dysfunction, trauma, or some type of tumor.
- Hyperprolactinemia: a high prolactin level decreases GnRH activity, which occurs mostly during pregnancy and breastfeeding.
- Patients with polycystic ovary syndrome (PCOS) and high insulin levels who have increased GnRH pulsation, which leads to disordered LH and FSH activity.
- Those affected by Kallmann's syndrome who have an absence of GnRH due to a congenital defect.

On the other hand, FSH and LH synthesis are also normally inhibited due to the negative feedback of androgens and estrogens on the pituitary gland.
GnRH Analogues
GnRH analogs are a type of molecule that has been artificially created by replacing some amino acids within the original GnRH molecule.
These new molecules imitate the shape of GnRH and also have a high affinity for its receptors in the pituitary gland.
Therefore, GnRH agonists can bind easily to the receptors and prevent the action of natural GnRH.
An analog is a substance with similar characteristics to another substance which, without being identical to it, can fulfill some of its functions.
In short, the action of the GnRH analogues consists of blocking the normal function of GnRH and preventing the flow of FSH and LH from the pituitary gland to the gonads.
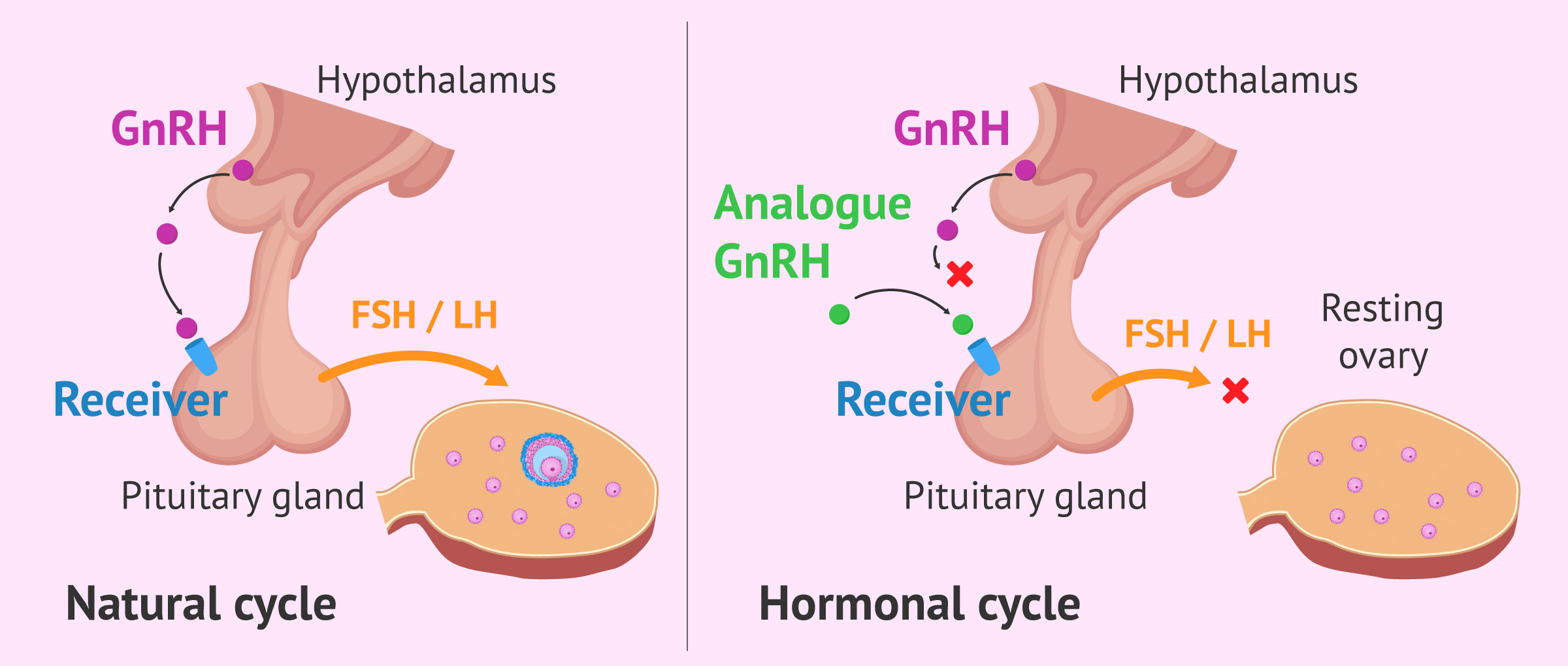
This ability of the GnRH analogs has been used to create the drugs that are administered during assisted reproduction treatments, such as artificial insemination (AI) or in vitro fertilization (IVF).
These are drugs used during the ovarian stimulation phase to achieve a stop of the pituitary gland and keep the ovaries at rest. In this way, the number of developed follicles and the moment of ovulation are controlled.
Types
There are two types of GnRH analogues that act differently:
- GnRH Agonists
- have a longer half-life and great affinity for the GnRH receptor in the pituitary gland. After agonist-receptor binding, a sudden release of gonadotropins occurs, which is known as the flare-up effect. However, if GnRH agonists continue to be administered continuously, the receptors are eventually blocked and stop responding, so that FSH and LH secretion is suspended.
- GnRH Antagonists
- its inhibitory effect is more direct. Once the antagonist has joined the receptor, the latter is immediately blocked.

Nowadays, assisted reproduction professionals tend to schedule ovarian stimulation protocols with antagonists rather than agonists due to the multiple advantages it offers.
Effects
As we have already explained, the main effect of GnRH analogs on the female body is to block the release of gonadotropins by the adenohypophysis.
This action allows the synchronization of the cohort of follicles recruited by the ovary at the beginning of ovarian stimulation. In this way, homogeneous follicular growth can take place, reducing the variability of ovarian response to gonadotropins administered exogenously.
In summary, the use of GnRH analogs allows the gynecologist to have better control of the ovarian stimulation process in the patients, and to know which is the most appropriate moment to trigger ovulation and to program the artificial insemination or ovarian puncture according to the case.
Assisted procreation, as any other medical treatment, requires that you rely on the professionalism of the doctors and staff of the clinic you choose. Obviously, each clinic is different. Get now your Fertility Report, which will select several clinics for you out of the pool of clinics that meet our strict quality criteria. Moreover, it will offer you a comparison between the fees and conditions each clinic offers in order for you to make a well informed choice.
Drugs with GnRH analoges
Depending on whether GnRH agonists or antagonists are used during the controlled ovarian stimulation phase, we will talk about long or short protocols, respectively.
This is because the agonists take longer to take effect, as we have already mentioned, while the antagonists have an immediate effect and will require fewer days of administration.
The commercial names of the agonists used in the long cycles and their active principles are as follows:
- Synarel
- This is a nasal spray containing nafarelin.
- Procrin
- the active ingredient is leuprorelin acetate and is administered subcutaneously.
- Decapeptyl
- Depending on the type of presentation, it is administered either subcutaneously or intramuscularly. It contains triptorelin as active ingredient.
As for the antagonists used in the short cycles, we find the following drugs:
- Cetrotide
- contains cetrorelix and injection is done subcutaneously
- Orgalutran
- its active ingredient is ganirelix and is administered subcutaneously.

If you are interested in obtaining more information about the drugs used in assisted reproduction, you can continue reading here: What Medication Are Used for Ovarian Stimulation?
FAQs from users
Why can't the GnRH hormone be detected in blood?
Gonadotropin-releasing hormone (GNRH) is a hormone released by neurons in the hypothalamus in a pulsatile form. It stimulates the release of gonadotropins (LH and FSH) by the adenohypophysis.
This hormone is rapidly metabolized and for this reason cannot be quantified in the blood.
Which GnRH analog drugs offer the best results?
There are several types of analogs, which differ by small variations of components of the molecule. These would be leuprorelin acetate, triptorelin, nafarelin, buserelin, and goserelin. There are several presentations (daily, monthly, quarterly ...), indicating at each time the most appropriate for the effect you want to achieve. Each type of analog also has its route of administration, which may be subcutaneous, intramuscular, or intranasal.
It has not been demonstrated that any of the agonists marketed is superior to another, although the subcutaneous route provides constant bioavailability and little variation between patients, while intranasal or inhalation absorption may be more variable.
Read more
What effect do gonadotropin-releasing hormone agonists have?
The main effects produced by the use of analogs that are GnRH agonists are, on the one hand, the initial release of gonadotropins (flare-up effect) and then blocking the release of these gonadotropins, preventing the communication between the pituitary gland and the ovary so that there is no follicular development or ovulation.
All this occurs temporarily when the reserve of FSH and LH in the pituitary is empty. Normally, the total blockage of GnRH receptors occurs between 5-10 days after the first administration of the agonist.
How does a GnRH analog treatment for uterine myomatosis look like?
Although the most common treatment for removing fibroids is surgical, GnRH agonist analogs can also serve as drug treatment to reduce the size of these fibroids.
Due to their effects, GnRH agonists cause a state of hypogonadotropic hypogonadism with very low estradiol values in women. This can help reduce fibroids and possible associated symptoms such as bleeding.
However, these drugs have unwanted side effects, and, after stopping treatment, the fibroids may grow back. For this reason, GnRH agonists are only used where indicated and as a pre-surgical step to facilitate surgery.
Suggested for you
Hemos hablado de las gonadotropinas como hormonas que tienen un efecto sobre el aparato reproductor femenino y masculino. Si quieres entrar en detalle sobre estas hormonas, puedes seguir leyendo en los siguientes artículos:
What is the Role of Follicle Stimulating Hormone (FSH)?
What is the Luteinizing Hormone or LH?
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Depalo R, Jayakrishan K, Garruti G, Totaro I, Panzarino M, Giorgino F, Selvaggi LE. GnRH agonist versus GnRH antagonist in in vitro fertilization and embryo transfer (IVF/ET). Reprod Biol Endocrinol. 2012 Apr 13;10:26 (View)
Gómez BP, Velázquez-Paniagua M. Fisiología de la reproducción: hormona liberadora de gonadotrofinas. Rev Fac Med UNAM, 2002; 45(6):252-257
Günter Emons, Carsten Gründker. The Role of Gonadotropin-Releasing Hormone (GnRH) in Endometrial Cancer. Cells. 2021 Feb 1;10(2):292. doi: 10.3390/cells10020292 (View)
Jacques Donnez, Marie-Madeleine Dolmans. GnRH Antagonists with or without Add-Back Therapy: A New Alternative in the Management of Endometriosis? Int J Mol Sci
. 2021 Oct 20;22(21):11342. doi: 10.3390/ijms222111342 (View)
Murillo EO, Cano A. Análogos de la GnRH en el tratamiento de los miomas. Med Clin (Barc). 2013 Jul;141 Suppl 1:35-9 (View)
Padula AM. GnRH analogues--agonists and antagonists. Anim Reprod Sci. 2005 Aug;88(1-2):115-26 (View)
FAQs from users: 'Why can't the GnRH hormone be detected in blood?', 'Which GnRH analog drugs offer the best results?', 'What effect do gonadotropin-releasing hormone agonists have?', 'What does it mean that GnRH agonists have a flare-up effect?' and 'How does a GnRH analog treatment for uterine myomatosis look like?'.






I’ve heard that treatment for uterine fibroids is given with GnRH, could you please tell me what it consists of.. I don’t want to undergo surgery.
Hi, I was prescribed treptorelin-decapeptyl before the transfer of the only embryo I have frozen, and I’m really afraid I’ll get it because it has too many side effects. I’ve read everything on the internet about this and I’m very afraid of this drug. If someone here has already had a treatment with this drug please tell me about your experience with the side effects.