Progesterone is a female sex hormone that has important functions in the female menstrual cycle and pregnancy.
Progesterone is mainly synthesized by the ovaries and placenta during pregnancy, although it is also produced by the adrenal glands and the liver in smaller quantities.
In assisted reproduction, progesterone is known to be the active ingredient of some drugs used in treatments, especially for being the main cause of some annoying symptoms.
Provided below is an index with the 9 points we are going to expand on in this article.
- 1.
- 2.
- 2.1.
- 2.2.
- 3.
- 3.1.
- 3.2.
- 4.
- 5.
- 5.1.
- 5.2.
- 5.3.
- 5.4.
- 5.5.
- 5.6.
- 5.7.
- 5.8.
- 6.
- 7.
- 8.
- 9.
What is progesterone?
Progesterone is a steroid hormone belonging to the progestogen group, i.e., the hormones responsible for maintaining pregnancy. For this reason, progesterone is also known as the pregnancy hormone.
Its production begins once a woman has reached puberty, with the first menstruation and the onset of menstrual cycles. This is why progesterone is a sex hormone that also contributes to the appearance and development of female secondary sexual characteristics.
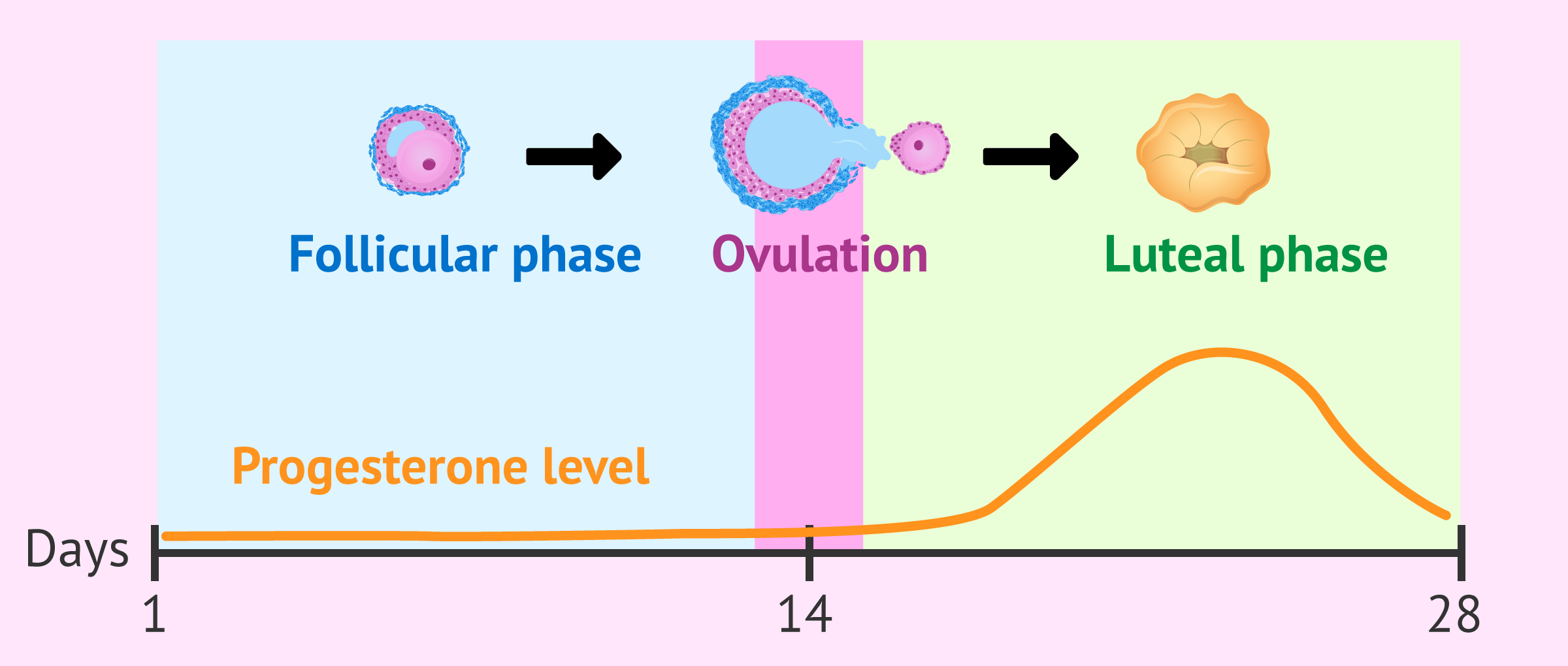
Specifically, progesterone is synthesized by the woman's ovaries after ovulation. Once the egg is expelled, the ovarian follicle becomes a corpus luteum that secretes progesterone throughout the luteal phase of the menstrual cycle until menstruation arrives.
What is progesterone used for?
The hormone progesterone has multiple functions in the human body, both in women and men.
However, in this section, we will focus on the functions of progesterone in the female reproductive system.
As mentioned above, progesterone levels increase during the second half of the menstrual cycle, just after ovulation.
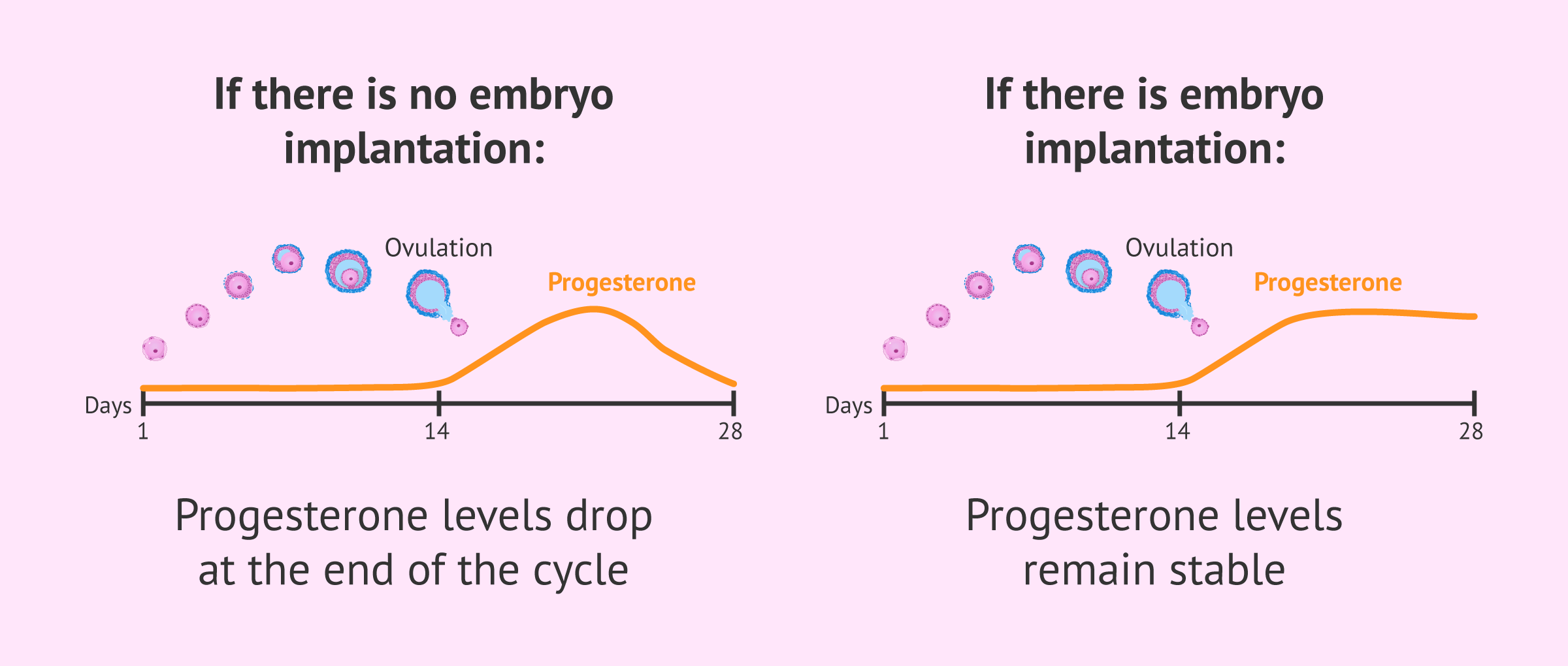
However, towards the end of the menstrual cycle, these levels begin to decrease or are maintained depending on whether or not there has been implantation of the embryo in the uterus.
In the following, we will discuss these two assumptions.
In a woman's menstrual cycle
Progesterone is synthesized in the luteal phase of the cycle with a clear objective: to make the endometrium receptive so that the embryo can nest in it and initiate a pregnancy.
If this does not occur, progesterone levels decrease during the fourth week of the menstrual cycle and this causes shedding of the endometrium in the form of menstruation. That is, as there has been no implantation or pregnancy, this endometrium has to be eliminated so that it can regenerate again in the next menstrual cycle.
The drop in progesterone is what triggers the onset of menstrual bleeding.
In addition, progesterone also causes the mammary glands to enlarge in the days leading up to menstruation.
In pregnancy
On the other hand, if the fertilized embryo has been implanted in the endometrium, the corpus luteum or yellow body of the ovary will continue to produce progesterone until about week 10 of pregnancy. The placenta will then be responsible for the secretion of progesterone until the end of gestation.
Its function is to maintain the uterine tissue in good condition throughout pregnancy. As a result, progesterone levels progressively increase month by month until they finally decline and labor is triggered.

Another function of progesterone during gestation is to thicken the cervical mucus so that it becomes impermeable to sperm.
In addition, progesterone is also responsible for breast enlargement during pregnancy and for preparing the mammary glands to secrete breast milk after giving birth.
Serum progesterone
Serum progesterone is a test that measures the level of this hormone in the blood.
This test is performed to detect any disturbance in the normal progesterone levels, which could lead to fertility problems, threatened miscarriage, etc.
The progesterone test is also used to find out if the woman has ovulated. In this particular case, the blood test should be done on day 21 of the menstrual cycle.
Progesterone values between 5 and 20 ng/ml on day 21 of the menstrual cycle indicate that ovulation has taken place days earlier.
In the following sections, we will discuss what altered progesterone levels may mean.
High progesterone
If after the blood test, the results show a higher than normal progesterone value, this could be indicative of:
- Pregnancy
- Ovarian cyst
- Molar pregnancy.
- Ovarian cancer
- Adrenal cancer
- Congenital adrenal hyperplasia

However, it is advisable to repeat the test, as well as to perform other complementary tests to obtain a more accurate diagnosis.
Low progesterone
Conversely, if progesterone levels are below baseline values, this could be indicative of:
- Anovulation (no ovulation)
- Threat of abortion
- Ectopic pregnancy
- Intrauterine fetal death

Obviously, for this test to indicate possible problems in pregnancy, pregnancy must have been confirmed beforehand, for example by means of a pregnancy test.
Progesterone testing is not usually performed in all pregnant women, only when there are signs of threatened miscarriage, such as vaginal bleeding, or when the woman has had repeated miscarriages.
Drugs with progesterone
On some occasions, it is necessary to administer progesterone artificially in order to treat some menstrual alterations, prevent risk situations or support the early stages of pregnancy.
Medications that include progesterone as an active ingredient have different presentations:
- In oral tablets
- this is the case of contraceptives that include progesterone to inhibit ovulation so that there is no risk of unwanted pregnancy. In addition, contraceptives that only include progesterone exclusively are known as mini-pills. These drugs are also used for hormone replacement therapy (HRT) in women who have reached menopause or to treat some hormonal imbalances along with estrogens.
- In vaginal ovules
- are micronized progesterone suppositories that are inserted through the vagina and are usually prescribed for luteal phase support infertility treatments, such as artificial insemination (AI) or in vitro fertilization (IVF). They are also used when there is a threat of miscarriage or when there is a risk of premature delivery. Utrogestan and Progeffik are the most popular progesterone drugs and both have the same price.
- Vaginal gel
- its form of administration is simpler than in the previous case and usually has the same indication. One of these drugs is Crinone.

- In injections
- for women who have a major progesterone deficiency or who do not assimilate the eggs or gel. They are subcutaneous or intramuscular injections that must be applied daily. One of these drugs is Prolutex and it has a much higher price than the previous formats.
Assisted procreation, as any other medical treatment, requires that you rely on the professionalism of the doctors and staff of the clinic you choose. Obviously, each clinic is different. Get now your Fertility Report, which will select several clinics for you out of the pool of clinics that meet our strict quality criteria. Moreover, it will offer you a comparison between the fees and conditions each clinic offers in order for you to make a well informed choice.
FAQs from users
What is progesterone used for after IVF?
In vitro fertilization (IVF) is a treatment in which embryos are generated in the laboratory from the gametes of the future parents or from anonymous donors. These embryos are then placed in the woman's uterus by embryo transfer.
In order for these embryos to implant in the endometrium, the endometrium must have the same characteristics as it would have had if fertilization had taken place in the uterus and not in the laboratory.
This implies that the endometrium must be exposed to the same hormonal variations as in a natural cycle. For this purpose, progesterone administered exogenously by means of vaginal or oral ovules is used.
Can I have anovulation due to lack of progesterone?
No. The lack of progesterone is conditioned by the lack of ovulation, not the other way around.
Read more
Why do some women take progesterone after embryo transfer and others do not?
In a normal cycle, after ovulation, progesterone begins to rise so that the endometrial tissue can be modified to allow implantation and the development of the eventual embryo. When we perform an embryo transfer, what we need is to reproduce this situation so that the embryo can implant.
Normally, the progesterone treatment starts a few days before the embryo transfer. In case of transfer in the same cycle as the follicular puncture, it starts the same day of the puncture, otherwise, it varies according to the stage of embryo development.
In case of transfer in a natural cycle (when no hormonal treatment is given to prepare the endometrium), progesterone is started on the same day of the transfer, but it is very unlikely that progesterone does not have to be taken after the embryo transfer because it is always preferred to support the luteal phase with exogenous progesterone.
Is it possible that my progesterone is high because I have only had eggs removed from one ovary?
No. The fact that only eggs are obtained from one ovary does not determine whether the amount of progesterone in the blood is higher or lower.
Read more
Do men also produce progesterone?
Yes, but in much lower amounts than women. Progesterone in the male sex is secreted by the adrenal glands and testes.
One of its functions in the male body is to regulate glucose levels and prevent prostate hyperplasia. In addition, progesterone is the precursor of testosterone, the male sex hormone par excellence.
Why don't I get my period after stopping progesterone?
If progesterone is taken for a long time, amenorrhoea, i.e. absence of menstruation due to atrophy of the endometrium, may occur.
Read more
What foods can I take to improve progesterone?
Through nutrition, it is possible to optimize the production of progesterone by the corpus luteum.
In general, foods that improve blood circulation are recommended, such as those rich in L-arginine and L-citrulline (watermelon, salmon, peas, green beans, chia seeds, sesame, nuts, etc.), those that stimulate the production of nitric oxide (beets, strawberries, carrots, spinach, chard, broccoli, etc.) and others that improve the health of the vascular wall (chocolate, garlic, onion, etc.).
It is also essential to maintain good levels of some micronutrients such as omega-3, zinc, vitamin B6 and antioxidants. To this end, it is recommended to include the following foods in the diet: sardines, salmon, mackerel, shellfish (rich in omega-3); whole grains, legumes, nuts and liver (rich in vitamin B6); pumpkin seeds, shellfish and white meats (rich in zinc); vegetables and fruits (rich in antioxidants).
Does the use of progesterone cause threatened miscarriage?
No, quite the opposite. Progesterone is sometimes prescribed to prevent possible miscarriages. This hormone helps to prepare the endometrium to be receptive and, therefore, to promote embryo implantation.
Progesterone also helps to keep the uterus in the ideal conditions for pregnancy to develop normally.
Recommended readings
Throughout the article, we have discussed the menstrual cycle, its phases, and the hormones involved in it. If you would like more information about this, we encourage you to continue reading here: The menstrual cycle: what happens in each of its phases?
You can also find out what are the normal values of hormones in women in the following article: Hormonal analysis in women.
Finally, you can find information about sex hormones and what their functions are in the following post: Male and female sex hormones.
Community and Support
At inviTRA we work to make monthly and rigorous information accessible to everyone. If this article has helped you, consider supporting us so we can continue accompanying more people on their journey to parenthood.
References
Czyzyk A, Podfigurna A, Genazzani AR, Meczekalski B. The role of progesterone therapy in early pregnancy: from physiological role to therapeutic utility. Gynecol Endocrinol. 2017 Jun;33(6):421-424 (View)
Maggio L, Rouse DJ. Progesterone. Clin Obstet Gynecol. 2014 Sep;57(3):547-56 (View)
Piette P. The history of natural progesterone, the never-ending story. Climacteric. 2018 Aug;21(4):308-314.
Stute P, Neulen J, Wildt L. The impact of micronized progesterone on the endometrium: a systematic review. Climacteric. 2016 Aug;19(4):316-28 (View)
FAQs from users: 'What is progesterone used for after IVF?', 'Can I have anovulation due to lack of progesterone?', 'Why do some women take progesterone after embryo transfer and others do not?', 'Why is it important to continue administering progesterone after a positive pregnancy test?', 'Is it possible that my progesterone is high because I have only had eggs removed from one ovary?', 'Do men also produce progesterone?', 'Why don't I get my period after stopping progesterone?', 'What foods can I take to improve progesterone?' and 'Does the use of progesterone cause threatened miscarriage?'.
Authors and contributors







More information about Cristina Algarra Goosman

Hi, I had a test on day 21 of my cycle and my progesterone levels were 18, what does that mean, is that normal?
Hi Katina,
Progesterone testing is done on day 21 as this is the time when progesterone is most concentrated in the body after ovulation to prepare the endometrium for a possible pregnancy.
The value obtained will indicate if ovulation has occurred, if the value is between 5 – 20 ng/mL, if ovulation has not occurred, values less than 5, or if there is a problem such as possible ovarian cysts if the value is higher than 20 ng/mL.
Your value of 18 ng/mL indicates that ovulation has occurred in the cycle and that the progesterone values are normal to prepare the endometrium for pregnancy.
I hope I could help,
Best regards.
Hello, they did a progesterone test and it came out at 120 ng/ml, I know it is high and I would like to know what I can do to lower it, thanks
Hi Kendall21,
The progesterone levels that you mention are very high, this can be for different reasons. The presence of pregnancy or some disease such as cancer or adrenal hyperplasia. I recommend that you go to the doctor so that he can assess whether it is a pregnancy or any of the conditions associated with a high level of progesterone.
I hope I’ve helped.
All the best